Place du Centre, 4th floor
200 Promenade du Portage
Gatineau QC K1A 1K8
29 May 2023
The Honourable Bill Blair, P.C., M.P.
President of the King’s Privy Council for Canada
House of Commons
Ottawa ON K1A 0A3
Dear Minister,
In accordance with subsection 13(3) of the Canadian Transportation Accident Investigation and Safety Board Act, the Board is pleased to submit, through you, its Annual Report to Parliament for the period 1 April 2022 to 31 March 2023.
Yours sincerely,
Original signed by
Kathleen Fox
Chair
Message from the Chair
The end of fiscal year (FY) 2022–23 marks the completion of a busy year for the Transportation Safety Board of Canada (TSB). We focused on completing many of our long-running investigations, some of which have highlighted significant safety issues present in Canada’s transportation system.
This year we released 59 investigation reports, well exceeding the output of 39 in FY 2021–22, including five reports in which the TSB issued a total of nine recommendations on needed changes in the air, marine, and rail sectors. Additionally, the TSB assessed the responses to 62 previous recommendations to ensure progress is being made.
In May 2022, we released our investigation report into the 2019 fatal sinking of the small fishing vessel Sarah Anne, off the coast of Newfoundland. The investigation prompted a recommendation to Fisheries and Oceans Canada to require that any Canadian vessel that is used to commercially harvest marine resources have a current and accurate Transport Canada (TC) registration. In August, we released our report into a 2019 collision between two freight trains near Portage la Prairie, Manitoba, in which we released two recommendations to TC, one of which builds on outstanding recommendations going back more than two decades. This accident highlights major issues in the rail industry and reinforces TSB’s call for physical fail-safe train controls.
In March 2023, we released our report into the fatal 2021 collision with terrain of a private aircraft near Lacombe, Alberta, in which we issued a recommendation to TC to routinely review and update the Handbook for Civil Aviation Medical Examiners to ensure it contains the most effective screening tools for assessing medical conditions, including cardiovascular disease. In the same month, we also released our report into the fatal sinking of the tug Ingenika, in which we issued four recommendations. The first two recommendations were addressed to TC to improve and expand regulatory surveillance of tugs under 15 gross tonnage. The other two recommendations were to the Pacific Pilotage Authority to address gaps in the issuance of pilotage waivers.
In October 2022, we released the most recent edition of the TSB Watchlist, putting the spotlight on key safety issues and actions that need to be addressed to make Canada’s transportation system even safer. The Watchlist highlights eight key safety issues that require government and industry attention, and are the result of hundreds of investigations, compelling findings and data, and active TSB recommendations. Some of these issues date back to well over a decade – a stark indication that while progress has been made, more needs to be done. Realizing that these issues are complex and take time to resolve, the Watchlist is moving to a three-year cycle to allow time for meaningful progress to be made by industry and the regulators.
To ensure industry stakeholders are well-informed on the work of the TSB, we conducted a series of outreach events, with TSB personnel sharing important safety messages at more than 50 industry events across the country.
This last fiscal year and the coming one will see some changes to the Board. On December 31, 2022, long-standing Board Member Faye Ackermans retired after serving a total of three terms.
My second term as Chair will come to an end this August and I have announced my intention to retire. It has been an honour to serve as the Chair of the TSB and I am proud of the progress the TSB has made as a world-leading safety investigation organization that influences change. Regardless of who serves on the Board in the future, the mandate and focus of the TSB’s work to advance transportation safety will not change, and nor will the dedication and professionalism of our staff.
Kathleen Fox
The year in results
In 2022–23, staff from the Transportation Safety Board of Canada (TSB) assessed thousands of accidents and incidents that occurred across Canada in the air, marine, pipeline, and rail transportation sectors (see the definitions in the Policy on Occurrence Classification).
TSB personnel deployed to the sites of some of these occurrences to collect data and carry out analysis in order to identify what happened and why, and to highlight known and emerging safety issues—all in an effort to improve transportation safety in Canada.
The total number of occurrences reported to the TSB (as required under the Transportation Safety Board Regulations) in the 2022 calendar year (3541) was 14% higher than the 2021 total of 3118 (Figure 1).
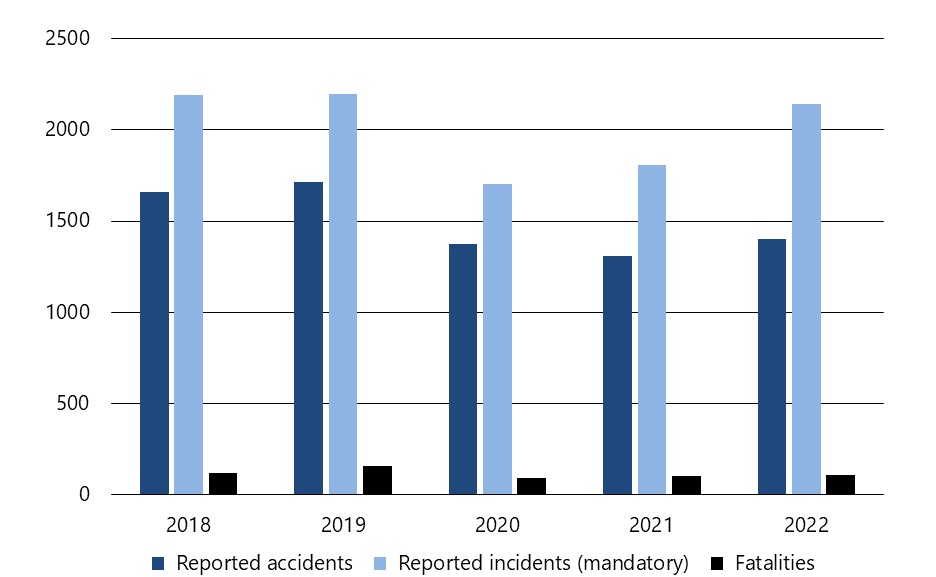
Figure 1. Data table
| Occurrences reported to the TSB | 2018 | 2019 | 2020 | 2021 | 2022 |
|---|---|---|---|---|---|
| Reported accidents | 1,659 | 1,713 | 1,376 | 1,311 | 1,402 |
| Reported incidents (mandatory) | 2,188 | 2,197 | 1,704 | 1,807 | 2,139 |
| Fatalities | 117 | 159 | 94 | 102 | 107 |
In 2022, there were 1402 accidents reported, 7% above the 2021 total of 1311, but 10% below the 10‑year average of 1555.
There were 5% more fatalities (107) across all transportation sectors in 2022 than there were in 2021 (102). However, the 2022 total represents a 16% decrease in fatalities from the 10-year average of 128.
The total of 2139 incidents reported to the TSB in 2022 was an 18% increase from the 2021 total of 1807 and a 12% increase from the 10-year average of 1915.The TSB at work
Deployments
TSB investigators deployed 69 times during 2022–23 (up from 46 the previous year) in response to occurrences in all sectors. These deployments took staff from the TSB regional offices and head office to locations across the country.
Investigations
In 2022–23, the TSB began 50 new investigations and completed 59 across all four transportation sectors (air, marine, pipeline, and rail) and in four classes of investigations (from in-depth and complex to limited scope) (Table 1).
| Investigations | 2021–22 | 2022–23 |
|---|---|---|
| Started during year | 55 | 50 |
| Completed during year | 39 | 59 |
| In progress on 31 March | 75 | 66 |
Average completion times increased, both overall and for the various classes of investigations. Class 4 investigations accounted for 41% of the total investigations completed during the reporting year. In these limited scope investigations, the TSB gathers data, conducts limited analysis, and reports the facts regarding less complex occurrences to raise awareness of relevant safety issues.
In support of TSB investigations, engineers, technical specialists, and human factors investigators began 145 projects and completed 152 technical reports in 2022–23. They also began three projects and completed eight technical reports for foreign investigation agencies.
Safety communications products
| Safety advisories | Safety information letters | Safety concerns | Recommendations |
|---|---|---|---|
| 11 | 6 | 2 | 9 |
Each year, the Board assesses progress made on outstanding recommendations as part of ongoing efforts to urge stakeholders to act on the safety issues identified in TSB investigations. In 2022–23, the Board assessed four responses to outstanding recommendations as Fully Satisfactory: three air transportation safety recommendations and one rail transportation safety recommendation.
Since 1990, the Board has made 626 recommendations. By the end of 2022–23, it had given 83.5% of the responses to these recommendations the highest rating of Fully Satisfactory. This means that stakeholders, including TC, have acted to substantially reduce the safety deficiencies the Board has identified (Figure 2).
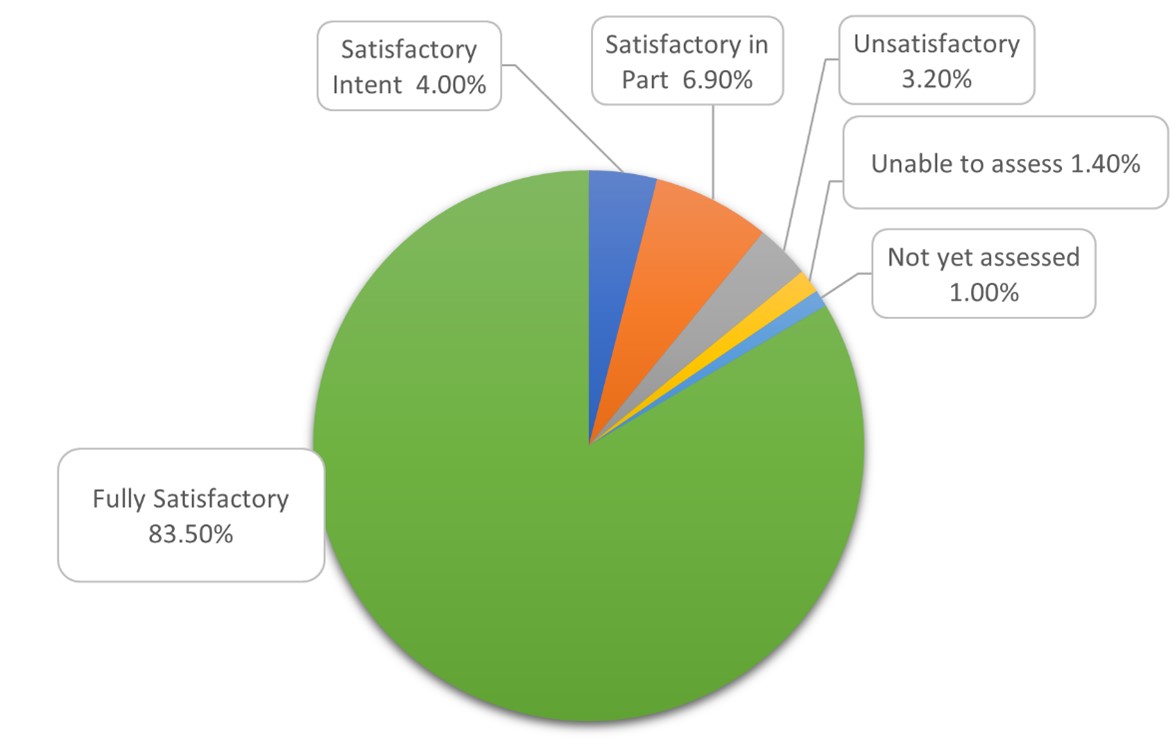
Figure 2. Data table
| Fully satisfactory | 83.50% |
|---|---|
| Satisfactory intent | 4.00% |
| Satisfactory in part | 6.90% |
| Unsatisfactory | 3.20% |
| Unable to assess | 1.40% |
| Not yet assessed | 1.00% |
At 31 March 2023, there were 87 outstanding recommendations, less than half of which date from 10 years ago or more (Table 3).
| Age of recommendations | Air transportation safety | Marine transportation safety | Rail transportation safety | Total (%) |
|---|---|---|---|---|
| Less than 1 year | 1 | 6 | 2 | 9 (10.30%) |
| 1 year to less than 7 years | 20 | 10 | 5 | 35 (40.20%) |
| 7 years to less than 10 years | 3 | 0 | 6 | 9 (10.30%) |
| Sub-total | 24 | 16 | 13 | 53 (60.92%) |
| 10 years to less than 15 years | 4 | 3 | 0 | 7 (8.05%) |
| 15 years to less than 20 years | 11 | 2 | 0 | 13 (14.94%) |
| 20 years or more | 8 | 3 | 3 | 14 (16.09%) |
| Sub-total | 23 | 8 | 3 | 34(39.08%) |
| Total | 47 | 24 | 16 | 87 (100.00%) |
Watchlist 2022
In October 2022, the TSB published the latest edition of its Watchlist, which identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer. These issues are supported by investigation reports, Board safety concerns, and recommendations.
There are eight issues currently on the Watchlist. Some of these issues date back to well over a decade—a stark indication that while efforts have been made, more needs to be done.
Leading up to the development of the current Watchlist, the TSB organized a series of discussions with its stakeholders at industry events to gauge progress made and discuss any emerging issues. These events included meetings of the Air Transport Association of Canada, the Helicopter Association of Canada, the Canadian Marine Advisory Council, and a TSB-led discussion session with the rail sector. The results of these discussions were used to inform Watchlist 2022.
Realizing that these issues are complex and take time, the Watchlist is moving to a three-year cycle to allow time for meaningful progress to be made by industry and TC.
SECURITAS
Through the TSB’s SECURITAS program, transportation industry employees and the public can report, in confidence, unsafe actions and conditions they observe.
The TSB received a total of 188 SECURITAS reports in 2022–23 (Table 4). This number is slightly higher than the 172 reports received the previous year.
| Air transportation safety | Marine transportation safety | Pipeline transportation safety | Rail transportation safety | |
|---|---|---|---|---|
| Reports received | 81 | 29 | 0 | 78 |
| Reports closed | 81 | 29 | 0 | 76 |
Of the 81 SECURITAS reports concerning air transportation safety , 80 were of a regulatory nature. These reports were redirected to TC. The other report submitted was about information related to an ongoing investigation and the reporter did not wish to remain anonymous, therefore the information was relayed to the investigator-in-charge.
In 2022–23, the TSB received 29 reports concerning marine transportation safety, a decrease of 35% from the previous year (44). The trusted agents responsible for handling SECURITAS matters on behalf of the Marine Branch closed all 29 reports. The reports covered a wide range of unsafe conditions on commercial fishing, passenger, and cargo vessels. These regulatory matters were resolved in collaboration with TC.
This year, the TSB received 78 SECURITAS reports on rail transportation safety. These included reports about inadequate railway employee familiarization and misaligned rail signals. By year-end, the trusted agents had closed all but two of the SECURITAS reports that the TSB had received.
Communications and outreach
Regular communications and outreach are important aspects of the TSB’s efforts to advance transportation safety. Through its website, social media channels, and participation in in-person and virtual events, the TSB reaches industry and government stakeholders as well as media and members of the public across Canada and around the world (tables 5, 6, and 7).
| Media requests | Interviews | News conferences | Industry outreach events |
|---|---|---|---|
| 430 | 58 | 4 | 54 |
| Deployment notices | Investigation webpages | Media advisories | News releases | Investigation reports |
|---|---|---|---|---|
| 47 | 37 | 5 | 64 | 59 |
| YouTube followers | Flickr followers | Twitter followers | LinkedIn followers | Facebook followers |
|---|---|---|---|---|
| 5362 | 607 | 26 087 | 5186 | 1192 |
Outreach activities
The TSB took part in over 50 industry events and meetings during the year, some online and others in person, to discuss matters in transportation safety including:
- Air Line Pilots Association annual conference
- Association québécoise du transport aérien annual conference
- Air Transport Association of Canada annual conference
- Helicopter Association of Canada annual conference
- Canadian Owners and Pilots Association annual conference
- Canadian Ferry Association annual conference
- Canadian Maritime Advisory Council annual and semi-annual conferences
- Passenger & Commercial Vessel Association
- Crude-by-Rail conference
- National Railway Day
- Wheel Rail Interface Conference 2022
Behind the scenes
Working toward the TSB’s strategic objective of becoming digital by default, we continued implementation of our new project tracking tool to support TSB project tracking, monitoring, searching, and reporting. This new tool will provide a single location for recording project information and a means of standardizing project information across the organization. After having onboarded our Engineering Laboratory to support the TSB’s engineering and human factors projects in 2021–22, this fiscal year the IT team completed its work on the tool to onboard the Communications Branch to track the lifecycle of investigation reports and related communications products.
Air transportation safety
The year in review
The TSB received 889 reports of air occurrences in 2022 (165 accidents and 724 incidents), including 34 fatalities (Figure 3).
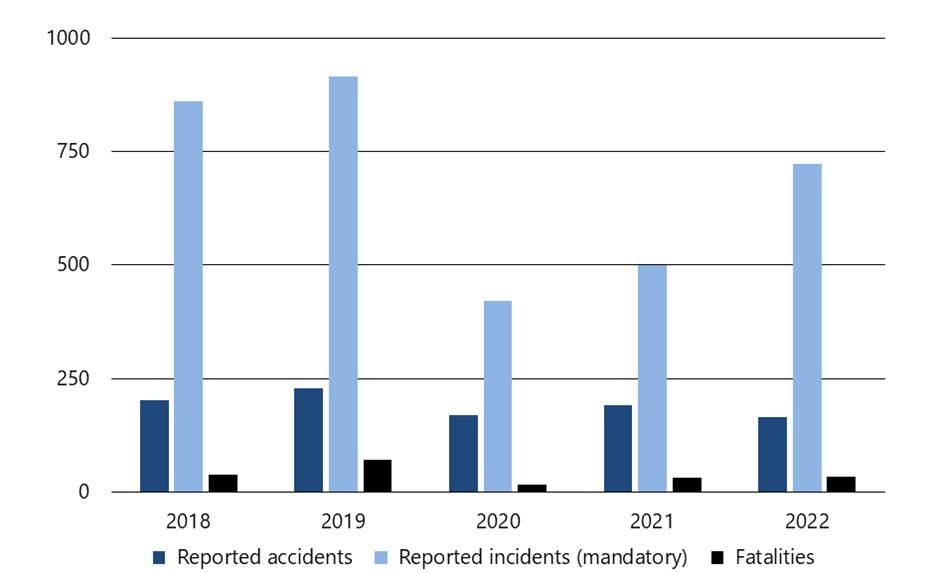
Figure 3. Data table
| 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|
| Reported accidents | 201 | 228 | 170 | 191 | 165 |
| Reported incidents (mandatory) | 860 | 915 | 421 | 500 | 724 |
| Fatalities | 38 | 70 | 16 | 31 | 34 |
A total of 165 accidents were reported in 2022. This number is 14% lower than the previous year’s total of 191 accidents and 29% below the yearly average of 233 accidents reported in the prior 10 years, 2012 to 2021. Most (152) of the accidents in 2022 took place in Canada and involved Canadian-registered aircraft. In general, the number of air transportation accidents has been decreasing in the last decade.
The TSB recorded 24 fatal air transportation accidents involving 34 fatalities in 2022. This is up slightly from 22 fatal accidents involving 31 fatalities in 2021, but is still 9% below the average of 26.4 fatal accidents involving 43 fatalities over the ten years from 2012 to 2021. Ten of the 34 air transportation fatalities in 2022 involved commercial operations: 3 of them under air taxi regulations (Civil Aviation Regulations Subpart 703 [CARs 703]), 6 under aerial work (CARs 702), and 1 under flight training operations (CARs 406). There were no fatalities involving airliner operations (CARs 705), or commuter operations (CARs 704) in 2022. The remaining 24 (of 34) fatalities in 2022 were linked to privately registered aircraft and involved recreational operators.
Seven accidents in 2022 involved a release of dangerous goods. This is above the average of 5 per year over the previous 10 years.
In addition, 724 air transportation incidents were reported. This represents an increase of 45% from the 500 that were reported in 2021, and it is 1% below the average of 733 incidents per year between 2012 and 2021. The majority of incidents in 2022 (490 or 68%) occurred in Canada and involved Canadian-registered aircraft.
Accident rate: A measure of air transportation safety
The overall air transportation accident rate of 2.6 accidents per 100 000 aircraft movements in 2022 is based on 138 accidents in Canada involving Canadian- and foreign-registered airplanes and helicopters (ultralights, gyroplanes, gliders, and remotely piloted aircraft are excluded) and the estimated 5.211 million movements at Canadian airports. The accident rate has fallen from 3.9 accidents per 100 000 aircraft movements in 2012 to a low of 2.6 in 2022. This accident rate is the lowest that the TSB has recorded since 2007, when it began publishing a rate based on movements (Figure 4).
Past editions of the TSB Annual Report used an accident rate based on the number of hours flown by Canadian aircraft. However, TC has indicated that it has temporarily suspended the collection of the data for the 2022 Annual Airworthiness Information Report (AAIR), which has been the source for information on hours flown. The air accident rate based on aircraft movements relies on data collected from multiple sources. While this metric represents most of the flying activity in Canada and is used by the TSB in other publications, it lacks information about aircraft movement activity that takes place at many small aerodromes or away from aerodromes entirely.
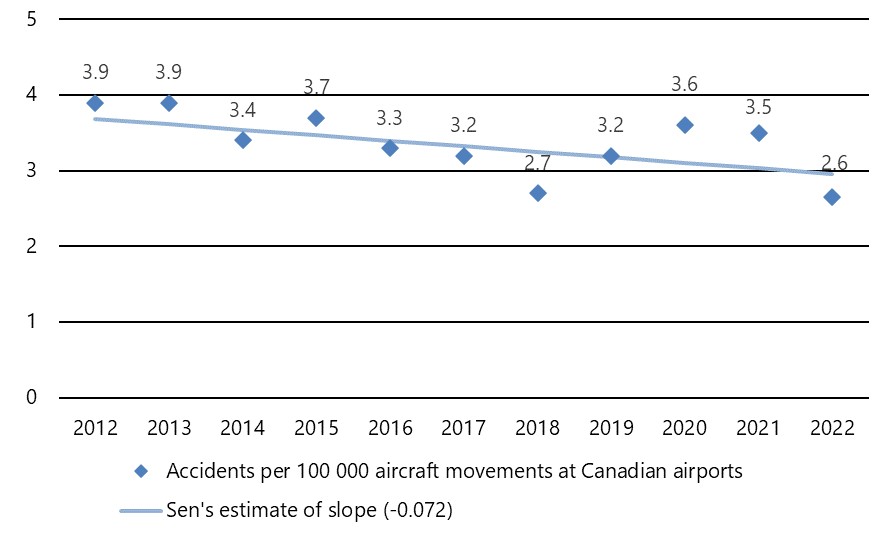
Figure 4. Data table
| Year | Accidents per 100 000 aircraft movements at Canadian airports | Sen's estimate of slope (-0.072) |
|---|---|---|
| 2012 | 3.9 | 3.68 |
| 2013 | 3.9 | 3.61 |
| 2014 | 3.4 | 3.54 |
| 2015 | 3.7 | 3.47 |
| 2016 | 3.3 | 3.40 |
| 2017 | 3.2 | 3.32 |
| 2018 | 2.7 | 3.25 |
| 2019 | 3.2 | 3.18 |
| 2020 | 3.6 | 3.11 |
| 2021 | 3.5 | 3.03 |
| 2022 | 2.6 | 2.96 |
Investigations
TSB staff deployed to 48 air transportation occurrences in 2022–23 (21 more than in 2021–22), began 34 investigations, and completed 39 (tables 8 and 9).
| Activities | 2021–22 | 2022–23 |
|---|---|---|
| Deployments | 27 | 48 |
| Investigations started | 37 | 34 |
| Investigations completed | 21 | 39 |
| Investigations in progress on 31 March of each year | 37 | 32 |
| Class (investigation type) | Completed investigations | Completion target (days) | Average duration (days) | ||
|---|---|---|---|---|---|
| 2021–22 | 2022–23 | 2021–22 | 2022–23 | ||
| 1 (safety issue) | 1 | n/a | 730 | 1219 | n/a |
| 2 (complex) | 3 | 2 | 600 | 1007 | 1073 |
| 3 (detailed) | 7 | 17 | 450 | 491 | 517 |
| 4 (limited scope) | 10 | 20 | 220 | 203 | 208 |
Deficiencies in regulatory surveillance and safety management highlighted following collision with terrain in instrument meteorological conditions
The TSB investigation into the December 2019 loss of control and collision with terrain of a Douglas DC3C Basler Turbo Conversions TP67 aircraft operated by North Star Air, near Sachigo Lake, Ontario, found that the decision to depart on, and continue, a daytime visual flight rules (VFR) flight in instrument meteorological conditions (IMC) was influenced by a distorted perception of risk resulting from successful past experience in similar situations (A19C0145).
The aircraft was scheduled to conduct a VFR cargo flight in northern Ontario. Weather conditions obtained by the captain for the flight route were marginal for VFR, with reports of IMC. During the descent from cruising altitude, the aircraft passed through cloud cover and broke out of cloud at very low level, and the aircraft was not in a position to continue with the planned visual approach. The captain made low-level manoeuvres in an attempt to land, before colliding with terrain southwest of the runway.
A results-oriented subculture of some of North Star Air’s DC3-TP67 pilots, which emphasized mission completion over regulatory compliance, resulted in VFR flights, such as the occurrence flight, being conducted in IMC.
Safety management is an issue on the TSB Watchlist, and is a concern in the air, marine, and rail transportation modes.
A lack of timely and effective regulatory surveillance to ensure operators in all modes are compliant is also an issue on the TSB Watchlist.
The report includes findings related to safety management and regulatory surveillance, two continuing issues on the TSB Watchlist. North Star Air’s safety management system did not identify the underlying factors that led to the reported instances of company aircraft operating VFR flights into IMC, nor were any additional measures taken to monitor its operation to ensure flights were being conducted in accordance with regulations. As a result, previously identified unsafe practices persisted and played a direct role in this occurrence.
In 2017, TC had provided information to the company of allegations regarding VFR flights in IMC for its internal investigation. A 2018 TC inspection of company operations did not include information about these allegations, about corrective action, or that the company investigation into these allegations was still open after almost two years. As seen in this occurrence, the unsafe practice of operating under VFR in IMC persisted unbeknownst to the regulator. If TC relies on operators to investigate allegations of regulatory non-compliance without monitoring them, there is an increased risk that the unsafe practices that are being investigated will persist.
The results of this investigation reflect the TSB’s ongoing concerns about safety management and regulatory surveillance, both issues on the TSB Watchlist for 2022.
Safety culture and medical examinations for pilots identified as issues in the investigation into main rotor blade failure during emergency landing
The TSB investigation into the September 2019 loss of control and collision with terrain of a Bell helicopter in Campbell River, British Columbia (A19P0142), found that an engine power anomaly likely occurred while the helicopter was in cruise flight and, as a result, the pilot reversed course and entered a descent consistent with an autorotation. At some point during the flight, the main rotors became deformed. In the last moments of the flight, likely as a result of the deformed blades, the main rotor rpm decreased to a point that could not sustain autorotational flight, and the helicopter fell vertically to the ground, striking a building and two vehicles. The pilot was fatally injured. The helicopter was destroyed by the impact forces and a post-impact fire.
The investigation revealed that the engine fuel system did not have the appropriate accumulators and double check valve for installation on the Bell 206 helicopter. During the installation of the engine, the company maintenance control system was ineffective at ensuring that the engine installation complied with the manufacturer’s recommendations.
The investigation examined the air operator’s safety culture. The pilot was the company’s owner, accountable executive, and operations manager. The investigation revealed that many operational and maintenance-related decisions were being made based on a single opinion, rather than a process of validation by a hierarchy of independent and skilled supervisors. In addition, several opportunities to improve the safety of the flight had been missed.
Finally, the investigation examined TC’s approach to managing cardiovascular health and hypertension in pilots. Using a variety of different risk calculators and all available medical information about the occurrence pilot, an independent cardiology review was conducted as part of this investigation and revealed that the pilot possessed many of the key indicators for a high-risk cardiac event. In this occurrence, TC’s civil aviation medical examination to assess pilot fitness did not identify the level of risk presented by the pilot. If TC guidance material and the civil aviation medical examination report do not require a Civil Aviation Medical Examiner to perform a global cardiovascular assessment, when appropriate, there is an increased risk that a pilot with high cardiovascular risk factors will be incapacitated while operating an aircraft as a result of a medical event.
Runway incursion and risk of collision at Toronto/Lester B. Pearson International Airport
The TSB investigation into the March 2020 runway incursion and risk of collision between an Air Canada Embraer 190 and an Air Canada Boeing 777 at Toronto/Lester B. Pearson International Airport, Ontario (A20O0029), found that the Embraer 190’s transponder transmitted that the aircraft was in the air after it accelerated past 50 knots, even though it was still on the runway. As it was accelerating during its take-off roll, the Embraer 190 struck a bird, and the flight crew initiated a rejected takeoff. At about the same time, the Boeing 777 was cleared for takeoff on the same runway. As the aircraft was accelerating on its take-off roll, the flight crew observed that the Embraer 190 was still on the runway and initiated a rejected takeoff. Both aircraft eventually exited the runway and returned to the terminal. There were no injuries to passengers or crew members. There was no damage to either aircraft.
The transponders on both the Embraer 190 and the Boeing 777 transmitted inaccurate in-air statuses during their respective take-off rolls. Based on this data, NAV CANADA’s runway incursion monitoring and conflict alert sub-system (RIMCAS) inaccurately identified both aircraft as being in air when in fact they were still on the ground. This resulted in late and inaccurate RIMCAS alerts and delayed the air traffic controller’s response to the risk of collision. The risk was only mitigated when the Boeing 777 flight crew rejected their takeoff after recognizing that the Embraer 190 was still on the runway ahead of them.
Runway incursions lead to an ongoing risk of aircraft colliding with vehicles or other aircraft. This issue has been on the TSB Watchlist since 2010.
The risk of collisions from runway incursions has been on the TSB Watchlist since its inception in 2010. The Watchlist calls for effective defences tailored to address identified hazards at airports and in aircraft, vehicles, and air traffic service facilities across Canada.
Following the occurrence, the TSB issued Aviation Safety Advisory A20O0029-D1-A1 to highlight the importance of accurate flight status data being validated and transmitted by transponders and how this data is received, validated, and used by runway monitoring and conflict alert systems to ensure maximum safety benefit.
Joint air/marine transportation safety investigation into an aircraft and water taxi collision
The TSB conducted a joint air/marine transportation safety investigation (A21P0111/M21P0290) into the October 2021 collision between a float-equipped de Havilland DHC-2 MK. I (Beaver) aircraft and a water taxi (Rocky Pass) in the vicinity of the First Street dock in the harbour at Tofino, British Columbia. The aircraft was substantially damaged and came to rest inverted with just the floats above the surface of the water. The five passengers and pilot on board the aircraft were able to egress safely. Three of the aircraft passengers received minor injuries. The vessel sustained minor damage and one passenger on it received minor injuries. The emergency locator transmitter on the aircraft did not transmit a signal.
The investigation found that the visual perception of both the aircraft pilot and the vessel operator was affected by several factors leading up to the collision, including
- the aircraft’s lowered left wing during the turn to final, coupled with the pilot’s seating position, interfered with the pilot’s view out the left-side window;
- the Rocky Pass’s entry into the harbour, which was unexpected in an otherwise clear area;
- the pilot’s attention, which was primarily focused straight ahead, combined with the little or no relative movement of the vessel in the left windscreen and the obstructions caused by the aircraft’s nose and left window post; and
- the speed at which the vessel was travelling and the relatively stationary position of the aircraft in the vessel operator’s peripheral vision.
As a result, neither the aircraft pilot nor the vessel operator recognized that their routes would conflict until it was too late for evasive action to be effective.
Framework for routine review of and improvement to Transport Canada’s guidelines for civil aviation medical examiners
As a result of its investigation into the fatal collision with terrain of a privately registered, amateur-built Cavalier SA102.5 aircraft near Lacombe Aerodrome, Alberta (A21W0089), the Board issued a recommendation to TC aimed at improving the guidelines for civil aviation medical examiners. The investigation report concluded that cardiovascular disease was a contributing factor to the pilot’s death; however, it could not be determined whether this resulted in an in-flight incapacitation or his death before or after the collision with terrain.
Since 2000, the TSB has investigated eight accidents, including this one, involving commercial pilots in which cardiovascular disease was identified as a finding as to risk or finding as to cause.
At March 2023, there was no framework in place at TC to routinely review the guidance document for medical examiners to ensure it contains the most effective screening tools for assessing medical conditions. Therefore, the Board recommended that the Department of Transport establish a framework for routine review and improvement to the Handbook for Civil Aviation Medical Examiners to ensure it contains the most effective screening tools for assessing medical conditions such as cardiovascular health issues (TSB Recommendation A23-01).
Following the occurrence, the Board issued Air Transportation Safety Advisory Letter A21W0089-D2-A1 (referenced below) to TC in January 2023 concerning physicians’ requirement to report to TC.
Safety advisories and safety information letters
The TSB issued one air transportation safety advisory letter as part of its investigations in 2022–23.
Physicians’ requirement to report to Transport Canada
As part of Air Transportation Safety Investigation A21W0089, the TSB issued Air Transportation Safety Advisory Letter A21W0089-D2-A1 to TC.
The investigation into this occurrence revealed that the pilot had been prescribed medications that may have affected his cardiovascular health and, therefore, could have affected flight safety. The family physician was not aware of the requirement under the Aeronautics Act to provide such information to TC; therefore, neither the medications nor the condition for which they were prescribed were reported. The pilot also did not report either the condition or the medications. The safety advisory letter encouraged the TC Civil Aviation Medical Branch, in cooperation with the Canadian Medical Association, to develop communication strategies to increase the awareness of the reporting requirements for physicians.
Progress on outstanding recommendations
Of the 30 responses to air transportation safety recommendations the Board assessed in 2022–23, five were closed. Of the five closed recommendations, three were closed after being rated Fully Satisfactory, and the other two were closed Satisfactory in Part. The remaining 25 recommendations obtained the following ratings: Satisfactory Intent (11), Satisfactory in Part (10), and Unable to Assess (four). No responses were assessed as Unsatisfactory.
This year, the responses to three recommendations issued as a result of the Swissair investigation (A98H0003) were assessed as Fully Satisfactory and closed:
- Recommendation A00-19 related to deficiencies regarding in-flight odour/smoke checklists. In the time since this recommendation was issued, many actions have been taken by TC and industry that the Board believes will substantially reduce the safety deficiency identified. These changes in industry, which are reflected in emergency checklists that use the voluntary guidelines developed in 2005, should assist flight crews in optimizing their response to conditions of smoke, fire, or fume events of unknown origin, and thus reduce the risk of an in-flight fire being ignited or sustained.
- Recommendation A01-03 related to material flammability test requirements for aircraft wiring. In the time since this recommendation was issued, a number of actions have been taken by TC and the United States Federal Aviation Administration to address the safety deficiency identified in this recommendation regarding mandating a certification test regime that evaluates aircraft electrical wire failure characteristics under realistic operating conditions and against specified performance criteria, with the goal of mitigating the risk of ignition. The Board believes these actions have been effective in addressing the risks identified in the recommendation. Similar actions have been adopted by the European Union Aviation Safety Agency.
- Recommendation A01-04 related to evaluating all aircraft systems in the pressurized portion of an aircraft to ensure that systems whose failure could exacerbate a fire in progress are designed to mitigate the risk of fire-induced failures. Many regulatory and industry actions have been taken over the years that have addressed the safety deficiencies identified in this and other recommendations issued as a result of the Swissair investigation. The Board believes these actions have been effective in addressing the risks identified in the recommendation. Similar actions have been adopted by the European Union Aviation Safety Agency.
As part of Air Transportation Safety Issue Investigation A17O0038, the Board issued Recommendation A18-07 to the Greater Toronto Airports Authority in January 2019. It was recommended that physical changes be made to the taxiway layout at Toronto/Lester B. Pearson International Airport to address the risk of incursions between the closely spaced parallel runways known as the south complex and that further improvements be made in the meantime to increase the conspicuity of the runway holding positions. An operational trial of angled hold position installations on two taxiways was launched in April 2021, and by February 2023, approximately 29 000 aircraft had used the new hold positions with no runway incursions. This, plus the proposed expansion of the trial to three additional taxiways, was encouraging and showed meaningful progress. However, until the trial has concluded and the results are assessed, there remains a residual risk for runway incursions on taxiways that adjoin the south complex runways. Therefore, the Board considers the response to Recommendation A18-07 to show Satisfactory Intent.
The issue of runway overruns is on the TSB Watchlist 2022 and is the subject of Recommendation A07-06, which was issued as a result of Air Transportation Safety Investigation A05H0002. The Board is encouraged to see that activity to meet the International Civil Aviation Organization’s (ICAO’s) 150 m runway end safety area (RESA) standard has begun at some airports, and that others have already implemented ICAO’s 300 m RESA recommendation. However, the Board is not convinced that the residual risk at airports with runways not required to comply with ICAO’s standard is as low as reasonably practicable. Additionally, the Board believes that TC should require operators of airports with runways longer than 1800 m that have a RESA shorter than ICAO’s recommended length of 300 m to conduct formal runway-specific risk assessments and to take action to mitigate the risks of overruns to the public, property, and the environment. The Board is of the opinion that, despite the actions taken to date, the safety risks associated with this recommendation remain. Therefore, the Board considers the response to Recommendation A07-06 to be Satisfactory in Part.
Recommendation A16-12, one of 14 recommendations issued as a result of Air Transportation Safety Investigation A13H0001, recommends that TC require all commercial aviation operators in Canada to implement a formal safety management system (SMS). The issue of safety management has been on the Watchlist since 2010. As highlighted in the most recent Watchlist, released in 2022, progress has been slow to extend the application of SMS beyond CARs Subpart 705 operators. While the Board is encouraged that TC is conducting a policy review that will assist in developing recommendations to modernize and expand SMS requirements, until this review is complete and changes are implemented to the requirements, it is unclear whether these efforts will address the safety deficiency identified in the recommendation. Therefore, the Board considers the response to Recommendation A16-12 to be Satisfactory in Part.
For all active recommendations, the TSB will continue to monitor the progress of planned actions and call for action to reduce or eliminate these deficiencies.
Marine transportation safety
The year in review
The TSB received 1209 reports of marine transportation occurrences in 2022 (241 accidents and 968 incidents), including seven fatalities.
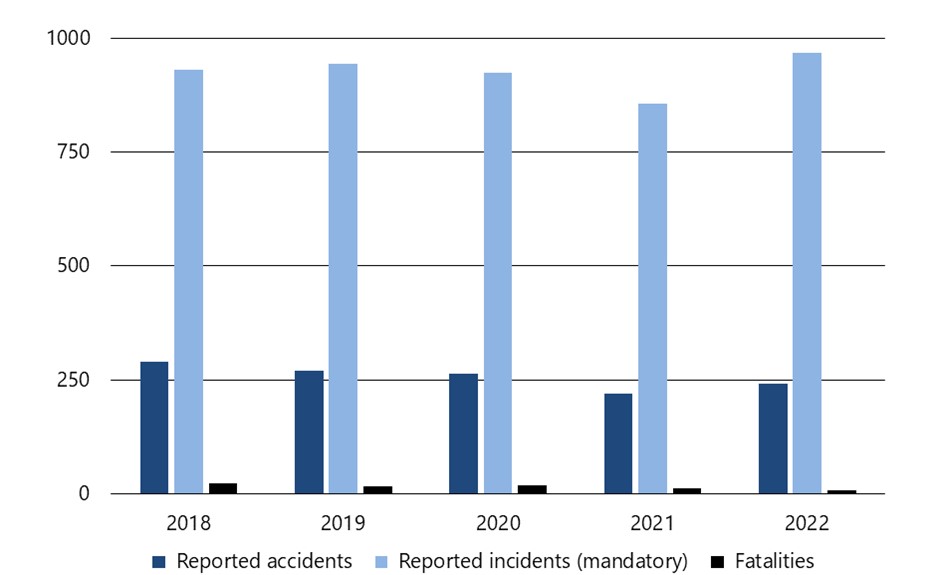
Figure 5. Data table
| 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|
| Reported accidents | 290 | 271 | 264 | 220 | 241 |
| Reported incidents (mandatory) | 931 | 945 | 925 | 856 | 968 |
| Fatalities | 22 | 17 | 18 | 11 | 7 |
The total of 241 marine transportation accidents represents an increase from the 220 accidents in 2021 but is lower than the 10-year average of 276. In 2022, 82% of accidents were shipping accidents (when a ship, for example, sinks, founders, or capsizes), the same as the previous 10-year average (82%). The remaining 18% of accidents in 2022 were aboard a ship (when a person is killed or seriously injured when, for example, boarding a ship or by falling overboard), also the same as the previous 10-year average (18%).
There were seven marine transportation fatalities in 2022, fewer than the 11 in 2021 and lower than the 10-year average of 15. Of the 7 fatalities, 2 involved shipping accidents. Over the previous 10 years, fatalities were fairly evenly divided between shipping accidents and accidents aboard ship.
As in previous years, the highest proportion of the fatalities (three of the seven) was related to commercial fishing (Canadian-flag vessels in Canadian waters). Due to this continuing trend, commercial fishing safety remains a key safety issue on the TSB Watchlist.
There were 229 vessels involved in the 197 shipping accidents that took place in 2022. In 2021, 200 vessels were involved in 177 shipping accidents. The increase was observed in all regions.
The 968 marine transportation incidents reported to the TSB in 2022 represent a 13% increase from 2021 and a 25% increase from the 10-year average of 776. As in previous years, most reportable incidents (82%) were related to the total failure of machinery or technical systems. The increase in incidents of this type is due largely to changes made in 2014 to TSB reporting requirements.
Accident rate: A measure of marine transportation safety
According to TC, 2022 marine activity (commercial vessel-kilometres) for Canadian commercial non-fishing vessels with a gross tonnage of over 15 (excluding passenger vessels and cruise ships) was 10% above the 2013-to-2021 average. The 2022 accident rate was 3.0 accidents per million commercial vessel-kilometres, lower than the 2013-to-2021 average of 4.0.
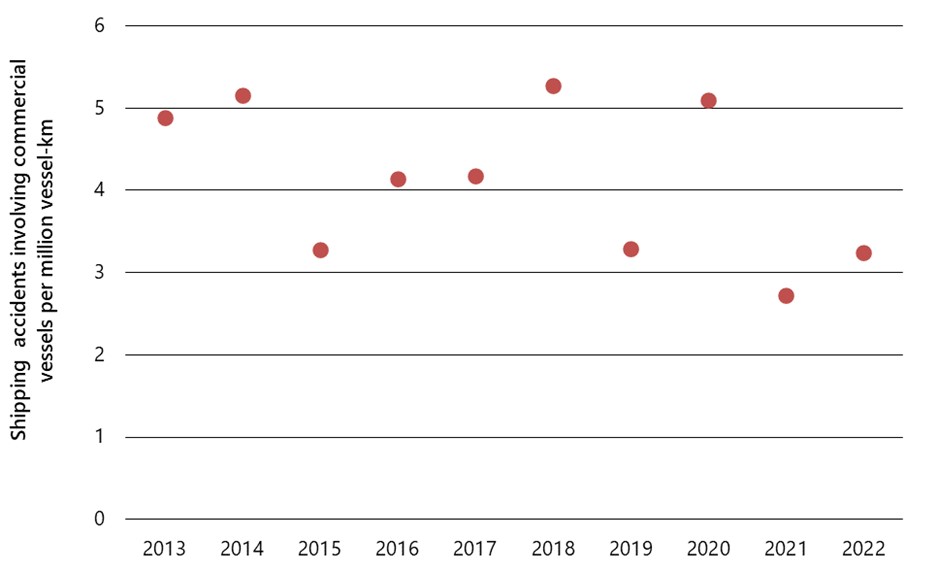
Figure 6. Data table
| Year | Shipping accident rate |
|---|---|
| 2013 | 4.9 |
| 2014 | 5.2 |
| 2015 | 3.3 |
| 2016 | 4.1 |
| 2017 | 4.2 |
| 2018 | 5.3 |
| 2019 | 3.3 |
| 2020 | 5.1 |
| 2021 | 2.7 |
| 2022 | 3.2 |
Investigations
In 2022–23, TSB staff deployed to 12 marine transportation occurrences (five more than in 2021–22), began nine investigations, and completed 10 (Table 10).
| Activities | 2021–22 | 2022–23 |
|---|---|---|
| Deployments | 7 | 12 |
| Investigations started | 9 | 9 |
| Investigations completed | 8 | 10 |
| Investigations in progress on 31 March of each year | 18 | 17 |
| Class (investigation type) | Completed investigations | Completion target (days) | Average duration (days) | ||
|---|---|---|---|---|---|
| 2021–22 | 2022–23 | 2021–22 | 2022–23 | ||
| 1 (safety issue) | 0 | 0 | 730 | n/a | n/a |
| 2 (complex) | 1 | 1 | 600 | 1001 | 1208 |
| 3 (detailed) | 6 | 7 | 450 | 771 | 791 |
| 4 (limited scope) | 1 | 2 | 220 | 234 | 345 |
Industry-wide surveillance issue related to written safety procedures
Following its investigation into the fatal 2020 sinking of the fishing vessel Chief William Saulis (M20A0434) near Digby, Nova Scotia, the TSB issued a recommendation to the Department of Transport to ensure that each inspection of a commercial fishing vessel verifies that each required written safety procedure is available to the crew and that the crew are knowledgeable of these procedures (M23-05). Both the Canada Shipping Act, 2001 and the Fishing Vessel Safety Regulations require a vessel’s authorized representative to provide written safety procedures that familiarize vessel crews with operational and emergency activities. While the vessel owner had provided a manual for vessel operations and safety, most of the safety procedures were based on templates provided by TC. The investigation found that these templates did not include all procedures required by regulation.
As seen with the Chief William Saulis, many company manuals may be incomplete if based mostly on these TC templates. Without TC oversight to validate that the written procedures required by regulation on board fishing vessels have been developed and that crew are knowledgeable of their content, there is a risk that fishing operations will continue without guidance critical to support the safety of the crew and the vessel.
The TSB has been monitoring commercial fishing safety since 1999, and this issue has been on the TSB Watchlist since 2010. Every year, the same safety deficiencies on board fishing vessels continue to put at risk the lives of thousands of Canadian commercial fish harvesters and the livelihoods of their families and communities.
The issue of fatigue management has been on the TSB Watchlist for rail transportation since 2016 and was expanded in 2018 to include air and marine operations.
A lack of timely and effective regulatory surveillance to ensure operators in all modes are compliant is an issue on the TSB Watchlist.
Safety management is an issue on the TSB Watchlist and is a concern in the air, marine, and rail transportation modes.
The ongoing lack of regulatory oversight means that fishing crews are routinely operating on vessels without even knowing how to stay safe or how to respond when things go wrong.
This occurrence raised concerns around four systemic safety issues identified on the TSB Watchlist: regulatory surveillance, commercial fishing safety, fatigue management, and safety management.
Enhancing the safety of tugs of 15 gross tonnage or less
Following its investigation into the fatal 2021 sinking of the tug Ingenika in the Gardner Canal, British Columbia (M21P0030), the TSB issued four recommendations aimed at enhancing the safety of tugs of 15 gross tonnage (GT) or less.
Currently, TC does not certify tugs of 15 GT or less, nor are these vessels required to undergo regular inspections. There were no records to indicate that TC had inspected the Ingenika at any point during its 50 years of operation.
Numerous TSB investigations have found that while vessel owners and operators have the primary responsibility to manage safety, it is vital that TC provide effective oversight. Although the TSB issued a safety concern to TC in 2016, the issue of regulatory surveillance for tugs of 15 GT or less persists and investigation findings continue to show that without adequate surveillance by the regulator, shortcomings in the safety management and operations of such tugs will continue to go unaddressed, leading to more accidents.
The TSB has also noted that there is currently no requirement for towing companies to assess any of the risks that might be present in their operations. This means that risks in towing operations will continue to go undetected and unmitigated, placing crews, tugs, tows, and the environment at risk.
Therefore, the Board recommended that the Department of Transport
- expand its surveillance program to include regular inspections of tugs of 15 GT or less to verify that these vessels are complying with regulatory requirements (M23-01); and
- require authorized representatives of tugs of 15 GT or less to assess the risks present in their operations, including the suitability of their tugs for the specific towing operations they are undertaking (M23-02).
At the time of the occurrence, the Ingenika was operating in a compulsory pilotage area that falls under the responsibility of the Pacific Pilotage Authority, which is mandated to establish, operate, maintain, and administer safe and efficient pilotage services in British Columbia.
The Pacific Pilotage Authority has a system under which vessels may obtain pilotage waivers that exempt them from having to take a licensed pilot on board if the operators and vessels meet certain requirements. However, it does not verify that the information submitted meets regulatory requirements, which leads to an increased risk that non-compliance will go undetected and compromise safety in compulsory pilotage waters.
The TSB identified similar issues regarding the Pacific Pilotage Authority’s pilotage waiver process in occurrences involving the Ocean Monarch (M17P0244) in 2017 and the Nathan E. Stewart (M16P0378) in 2016.
Therefore, the Board recommended that the Pacific Pilotage Authority
- verify that eligibility requirements are met before issuing pilotage waivers to companies operating tugs in compulsory pilotage areas (M23-03); and
- implement a process to verify ongoing compliance with waiver conditions by companies operating tugs in compulsory pilotage areas (M23-04).
Improving coordination between federal departments to improve the safety of commercial fishing in Canada
As a result of its investigation into the fatal 2020 sinking of the fishing vessel Sarah Anne in Placentia Bay, Newfoundland and Labrador (M20A0160), the TSB recommended that the Department of Fisheries and Oceans require all commercial fishing vessels to have a current and accurate TC registration (M22-01). Vessel registration gives TC the opportunity to provide safety oversight and guidance to fishing vessel owners. This recommendation is meant to push for improved coordination between the two primary federal departments that interact with the commercial fishing sector. Their combined efforts can work to increase the awareness and compliance with safety requirements among all commercial fish harvesters.
This investigation highlighted a number of systemic factors that were identified by the TSB’s 2009–2012 safety issues investigation into fishing safety in Canada (M09Z0001). These include vessel modifications and their impact on stability; the lack of, or failure to use, lifesaving equipment, such as personal flotation devices (PFDs), immersion suits, and emergency signaling devices; and inadequate regulatory oversight.
The investigation found that the vessel likely capsized suddenly, resulting in all crew members entering the water unexpectedly, before they had the chance to put on lifejackets, personal flotation devices or immersion suits, deploy the life raft, or make a distress call. Without critical pieces of lifesaving equipment, the crew would have remained in the cold water, likely unassisted, and drowned. Also, the Sarah Anne did not have a formal stability assessment, and there was no information available regarding its stability. Without this critical information, the crew made operating decisions without knowing the vessel’s actual safe operating limits. This may have negatively affected the vessel’s stability and led to it capsizing and sinking. The voyage of the Sarah Anne was not actively monitored by any external system and no distress signal was received. This resulted in a delay of several hours in the search and rescue response, severely reducing the crew’s chances of survival.
Regulators, vessel owners, and fish harvesters each must take ownership of safety to reduce accidents and preventable loss of life. Vessel owners can have their vessels assessed for stability, and equip them with the proper lifesaving equipment to survive a sudden capsizing. Crew members aboard fishing vessels can greatly increase their likelihood of survival by carrying a personal locator beacon, to signal for help to get out of the water as soon as possible, and by wearing a PFD to remain afloat until help arrives.
Safety advisories and safety information letters
The TSB issued three marine transportation safety advisories and information letters as part of its investigations in 2022–23.
Safety during docking and undocking operations
As part of Marine Transportation Safety Investigation M22C0005 into the fatal injury of a crew member on the Canadian-flagged roll-on/roll-off ferry Madeleine II in the Cap-aux-Meules harbour, Québec, the TSB issued Marine Transportation Safety Advisory Letter 03/22 to TC in October 2022. The letter identified that according to statistics from the TSB database, from January 2017 to March 2022, 13 occurrences (including the Madeleine II) were reported in Canada on Canadian- and foreign-flagged vessels. As a result of these occurrences, 12 people were seriously injured and two people were fatally injured.
The letter went on to explain that one of the main risks present during mooring operations is snap-back, which is the sudden release of built-up energy in a mooring line under tension. A common practice to mitigate this risk is to paint snap-back zones on the deck at mooring stations. The latest version of the UK Maritime & Coastguard Agency’s Code of Safe Working Practices for Merchant Seafarers now recommends considering the entire mooring deck be considered a snap-back zone and that clear and visible signage be posted to alert the crew. TC was provided this information for whatever follow-up action was deemed appropriate.
Safety issues on passenger vessels owned by the City of Toronto
The TSB conducted Marine Transportation Safety Investigation M22C0231 into the passenger ferry Sam McBride striking the dock while berthing at the Jack Layton Ferry Terminal in Toronto, Ontario. As part of the investigation, the TSB issued Marine Transportation Safety Advisory Letter 02/22 to the City of Toronto. Important safety issues were identified, relating to emergency preparedness, passenger safety management, and lifesaving equipment on one or more vessels operated by the city. For example, pre-departure safety briefings were not being consistently provided to passengers, the vessel’s crew complement for the maximum number of passengers did not allow tasks set out on the evacuation plan and muster list to be completed simultaneously, and passengers were counted using a hand-held tally counter. Furthermore, children, infants, and other passengers who may require extra assistance were not counted separately, and no infant lifejackets were on board.
The safety issues identified in this letter were communicated before the investigation was complete to ensure that those best able to take remedial action and effect change were made aware of the identified safety issues in a timely manner. Resulting from the communication of these safety issues, the City of Toronto’s website was updated to encourage caregivers to bring lifejackets for infants weighing less than 15 kg.
Failure of personal flotation devices to inflate
The TSB conducted Marine Transportation Safety Investigation M22A0332 into a fatality involving the pilot vessel APA No. 18 near St. John’s, Newfoundland and Labrador. A deckhand wearing an auto-inflating personal floatation device (PFD) fell overboard, but the device did not actually inflate. TSB laboratory inspection revealed that the inflator cap and body of the PFD were not mated, causing it to not be sealed and thus not inflate.
As a result, the TSB issued Marine Transportation Safety Advisory Letter 01/23 to the Atlantic Pilotage Authority in February 2023. The letter referred to TC’s Ship Safety Bulletin 12/2019, which highlighted the need to inspect and service inflatable lifejackets regularly and according to the manufacturer’s instructions.
Progress on outstanding recommendations
Of the 18 responses to marine transportation safety recommendations the Board assessed in 2022–23, none were closed, and no recommendations received a rating of Fully Satisfactory. The responses assessed were rated as Satisfactory Intent (six), Satisfactory in Part (nine), and Unsatisfactory (three).
In Recommendation M99-02, issued in November 1999, the Board recommended that the provinces review their workplace legislation with a view to presenting it in a manner that will be readily understood by those to whom it applies, and to help ensure that the enforcement mechanism and the regulatory regime complement each other. By 2021–22, all but two provinces had submitted responses that were assessed as Fully Satisfactory. In 2022–23, the Province of New Brunswick’s response was assessed as Fully Satisfactory with the passing of the bill An Act Respecting the Health and Safety of Fishers. This leaves the Province of Ontario, which continues to conduct consultations with stakeholders and partners to ensure that employers of the commercial fishing sector understand health and safety requirements but still does not have occupational health and safety regulations or guidance in place that is specific to the fishing sector. The Province of Ontario’s response was therefore assessed as being Satisfactory in Part.
For all active recommendations, the TSB will continue to monitor the progress of planned actions and call for action to reduce or eliminate these deficiencies.
Pipeline transportation safety
The year in review
The TSB received 67 reports of pipeline transportation occurrences in 2022–23, of which 66 were incidents and one was an accident. There were no fatalities arising directly from the operation of any federally regulated pipeline, as has been the case since the TSB’s inception in 1990.
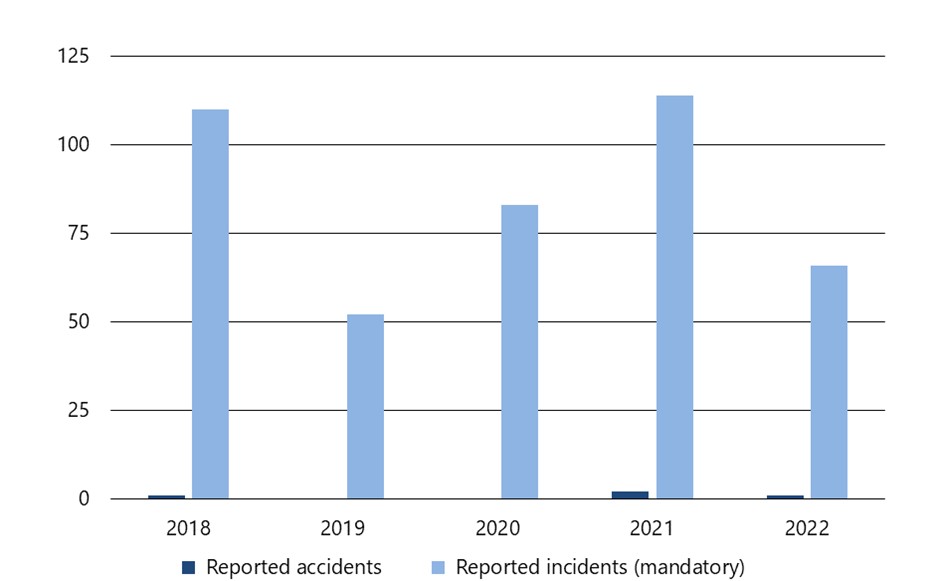
Figure 7. Data table
| 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|
| Reported accidents | 1 | 0 | 0 | 2 | 1 |
| Reported incidents (mandatory) | 110 | 52 | 83 | 114 | 66 |
| Fatalities | 0 | 0 | 0 | 0 | 0 |
This number of occurrences in 2022 (67) is 42% below the number reported in 2021 (116) and 40% below the average of 112 for the previous 10 years. The one accident in 2022 represented a decline from the two in 2021 and is also below the average of three accidents per year over the previous decade. Changes that were introduced in 2014 to the occurrence reporting criteria continue to distinguish more recent years from the years prior to the change.
Of the 67 occurrences in 2022, 25 involved a release of product:
- This was the highest number of occurrences with product release since 2018 (41), but lower than any of the years from 2012 to 2017.
- These occurrences represent 37% of those reported in 2022, and 57% below the 10-year average.
- The majority of these occurrences involved a release of hydrocarbon gas (60%), as has been the case each year since 2015.
- Seven occurrences involved the release of low vapour pressure hydrocarbons, namely crude oil; this was the highest number of such releases since 2014.
The TSB’s Statistical Summary: Pipeline Transportation Occurrences in 2022 contains more information on product releases during the year.
In 2022, 14 occurrences involved geotechnical, hydrotechnical or environmental activity—slope movements or river erosion, for example—roughly one-quarter the number reported in 2021, and slightly below the average of 17 such events per year over the previous 10 years. There were 13 reports of pipelines being contacted by an object in 2022 compared with the average of eight reports per year during the previous 10 years; there were also six occurrences with unauthorized third-party activity, compared with a 10-year average of three per year.Occurrence rate: A measure of pipeline transportation safety
There were 68 700 km of federally regulated pipeline operating in Canada in 2022, according to the Canada Energy Regulator. The 67 pipeline transportation occurrences reported to the TSB for the year resulted in a rate of 1 occurrence per 1000 km of operating pipeline. This is below the 2021 rate of 1.7 and the average rate of 1.6 from 2012 to 2021.
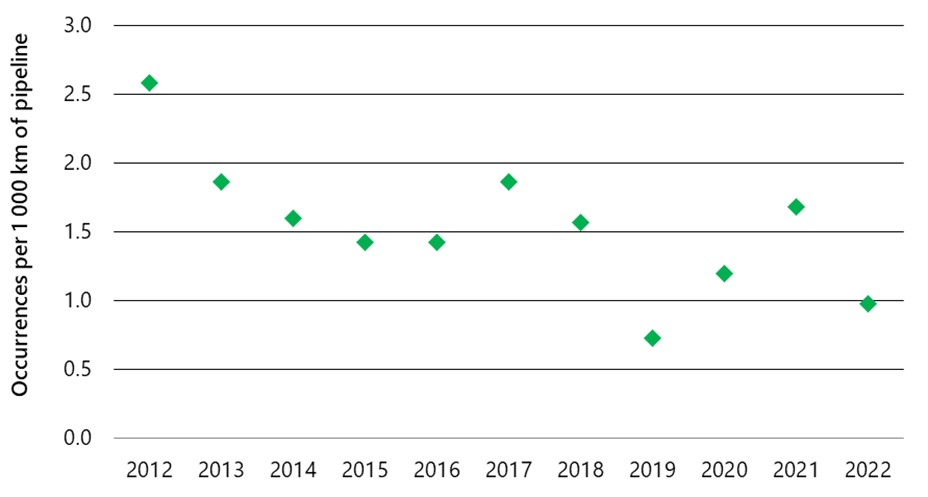
Figure 8. Data table
| Year | Occurrences per 1000 km |
|---|---|
| 2012 | 2.6 |
| 2013 | 1.9 |
| 2014 | 1.6 |
| 2015 | 1.4 |
| 2016 | 1.4 |
| 2017 | 1.9 |
| 2018 | 1.6 |
| 2019 | 0.7 |
| 2020 | 1.2 |
| 2021 | 1.7 |
| 2022 | 1.0 |
Investigations
TSB staff deployed to one pipeline transportation occurrence in 2022–23 and began one investigation (Table 12).
| Activities | 2021–22 | 2022-23 |
|---|---|---|
| Deployments | 1 | 1 |
| Investigations started | 1 | 1 |
| Investigations completed | 1 | 1 |
| Investigations in progress on 31 March of each year | 1 | 1 |
The TSB completed one pipeline investigation in 2022–23, a detailed class 3 investigation that took 527 days (Table 13).
| Class (investigation type) | Completed Investigations | Completion target (days) | Average duration (days) | ||
|---|---|---|---|---|---|
| 2021–22 | 2022–23 | 2021–22 | 2022–23 | ||
| 1 (safety issue) | 0 | 0 | 730 | n/a | n/a |
| 2 (complex) | 0 | 0 | 600 | n/a | n/a |
| 3 (detailed) | 0 | 1 | 450 | n/a | 527 |
| 4 (limited scope) | 1 | 0 | 220 | 304 | n/a |
Natural gas pipeline rupture
The TSB released one pipeline transportation safety investigation report in 2022–23, concerning the 2021 rupture of a natural gas pipeline near McAuley, Manitoba (P21H0143).
The Minell pipeline, a 6-inch natural gas pipeline operated by Manitoba Hydro, was struck by a farm tractor blade as it was scraping the ground in an agricultural field. The pipeline ruptured and released approximately 84 000 m³ of natural gas.
The investigation found that the depth of ground cover over the pipeline at the occurrence location was insufficient to prevent the ground-scraping blade from contacting the pipeline. Over time, the removal of weeds and silt from the drainage ditch gradually reduced the depth of cover over the pipeline. This was not identified by Manitoba Hydro’s damage prevention program, and, as a result, the pipeline kept operating with reduced ground cover.
The investigation analyzed the response time from when the rupture took place until the ruptured section of the pipeline was isolated. The rupture occurred near TC Energy’s Moosomin compressor station, which supplies the Minell pipeline. However, Manitoba Hydro’s procedures at the time of the occurrence did not identify TC Energy as a possible resource in the response to an occurrence, and the flow of gas continued into the ruptured section of pipeline until Manitoba Hydro was able to isolate it, 106 minutes after the rupture was suspected.
Following the occurrence, the TSB issued Pipeline Transportation Safety Advisory Letter 01/22 to Manitoba Hydro and indicated that pipeline operators need to be aware of the depth of cover over their pipelines to ensure they are adequately protected against normal agricultural activities that do not require explicit authorization. Manitoba Hydro completed a depth of cover survey for the entire Minell pipeline, in response to an order issued by the Canada Energy Regulator with respect to the occurrence. Ten locations were found to have cover less than 0.65 m, and these were staked and/or barricaded. The company also met with the affected landowners and provided written notifications in November 2021 prohibiting agricultural work, vehicle crossings, and other ground disturbance activities in these locations.
Safety advisories and safety information letters
The TSB did not issue any pipeline transportation safety advisories or safety information letters as part of an investigation in 2022–23.
Progress on outstanding recommendations
The Board did not issue any pipeline transportation safety recommendations in 2022–23 and had previously assessed all responses to pipeline transportation safety recommendations as Fully Satisfactory.
Rail transportation safety
The year in review
The TSB received 1376 reports of rail transportation occurrences in 2022 (995 accidents and 381 incidents), including 66 fatalities.
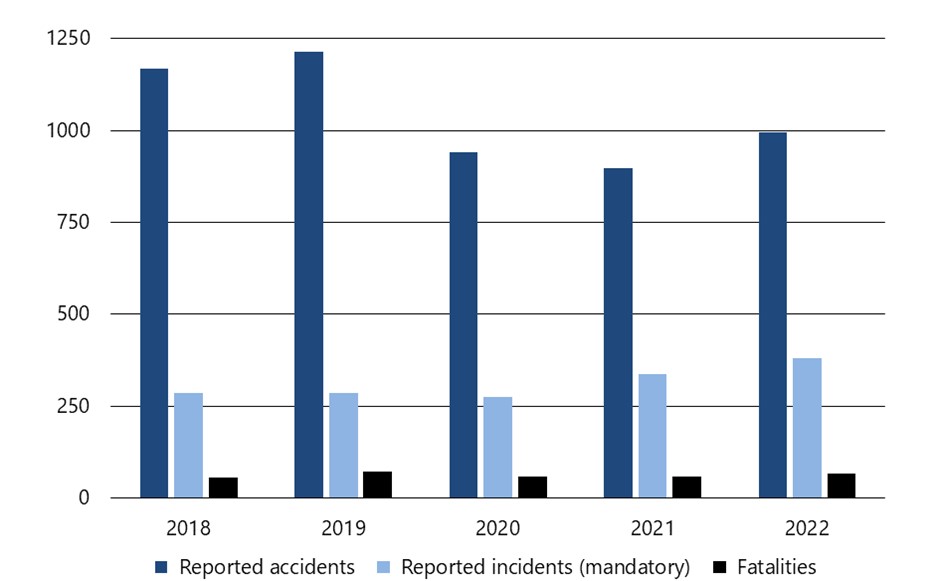
Figure 9. Data table
| 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|
| Reported accidents | 1167 | 1214 | 942 | 898 | 995 |
| Reported incidents (mandatory) | 287 | 285 | 275 | 337 | 381 |
| Fatalities | 57 | 72 | 60 | 60 | 66 |
The 995 accidents represent an 11% increase from 2021 (898), but a 5% decrease from the 10-year average of 1043.
The 66 rail transportation-related fatalities reported in 2022 are up compared to 60 in 2021 but below the 10 year average of 70. Among the fatalities, 52 involved trespassers, compared to 41 in 2021 and the 10-year average of 40. There were no railway employee fatalities in 2022.
The number of crossing accident fatalities decreased in 2022 (14) compared to 2021 (17) and is lower than the 10-year average of 22.
Among all rail transportation accidents, 111 involved dangerous goods. This is up from 86 in 2021 but is lower than the 10-year average of 121. Two accidents in 2022 resulted in dangerous goods being released.
There were 381 rail transportation incidents reported to the TSB in 2022, a 13% increase from 2021 (337). Incidents involving movements that exceeded limits of authority accounted for 35% (134) of all rail transportation incidents in 2022, 25 more than in 2021 and above the 10-year average of 128.
Accident rate: A measure of rail transportation safety
According to TC data, 2022 main-track (non-yard) rail activity increased by 2% from 2021. The main-track accident rate in 2022 was 3 accidents per million main-track train-miles, up from 2.9 in 2021 and above the 10-year average of 2.4.
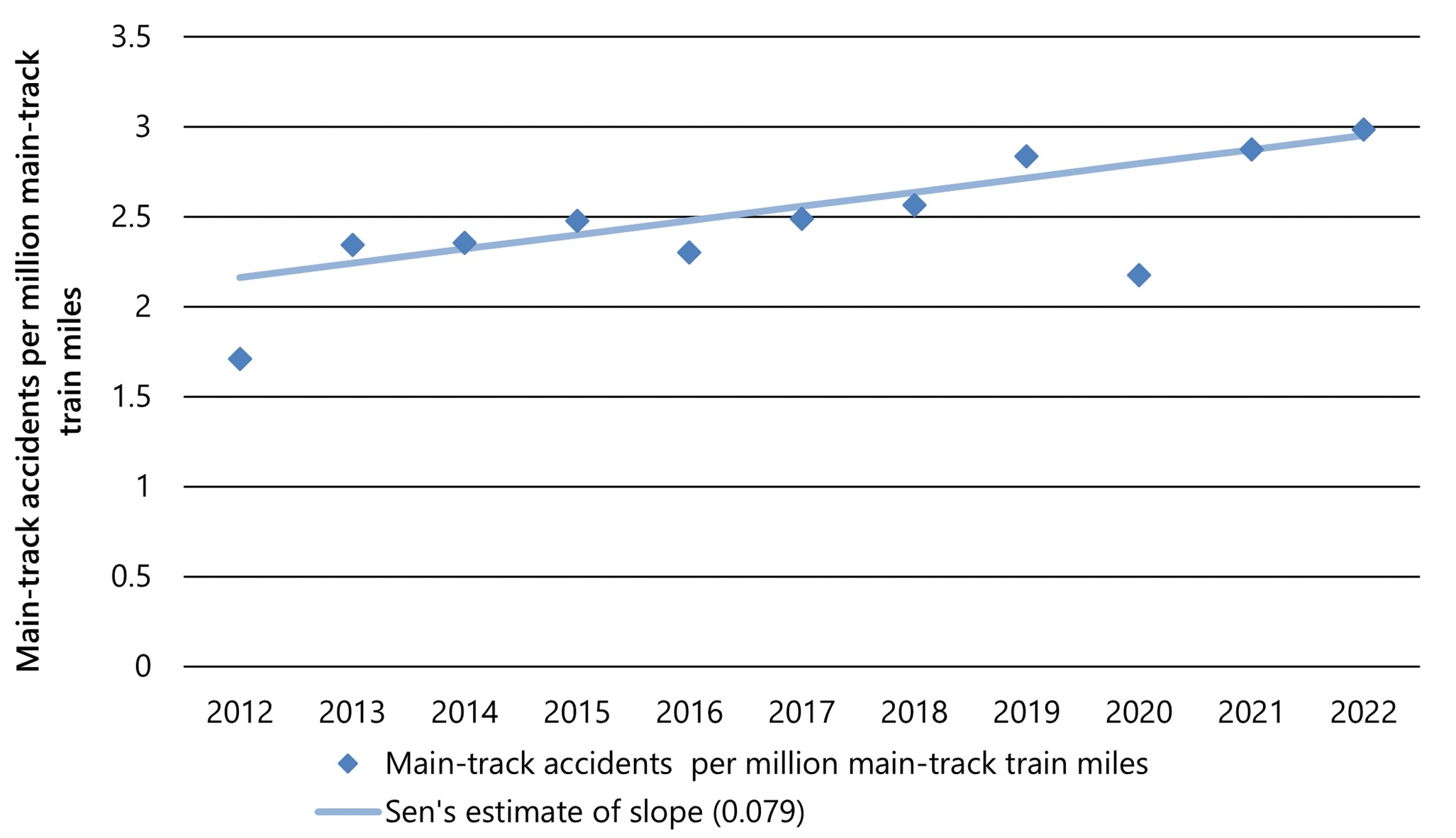
Figure 10. Data table
| 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Main-track accidents per million main-track train miles | 1.7 | 2.3 | 2.4 | 2.5 | 2.3 | 2.5 | 2.6 | 2.8 | 2.2 | 2.9 | 3.0 |
| Sen's estimate of slope (0.079) | 2.16 | 2.24 | 2.32 | 2.40 | 2.48 | 2.56 | 2.64 | 2.72 | 2.79 | 2.87 | 2.95 |
Investigations
TSB staff deployed to eight rail transportation occurrences in 2022–23, three fewer than in 2021–22, and began six investigations (Table 14).
| Activities | 2021–22 | 2022-23 |
|---|---|---|
| Deployments | 11 | 8 |
| Investigations started | 8 | 6 |
| Investigations completed | 9 | 9 |
| Investigations in progress on 31 March of each year | 19 | 16 |
| Class (investigation type) | Completed investigations | Completion target (days) | Average duration (days) | ||
|---|---|---|---|---|---|
| 2021–22 | 2022–23 | 2021–22 | 2022–23 | ||
| 1 (safety issue) | 0 | 0 | 730 | n/a | n/a |
| 2 (complex) | 1 | 4 | 600 | 1151 | 1161 |
| 3 (detailed) | 3 | 3 | 450 | 658 | 759 |
| 4 (limited scope) | 5 | 2 | 220 | 299 | 398 |
Automated train control systems and formal crew resource management training
As a result of its investigation into the 2019 collision of two Canadian National Railway Company (CN) freight trains near Portage la Prairie, Manitoba (R19W0002), the Board issued two recommendations to TC regarding the implementation of physical fail-safe train control systems and formal crew resource management training for railway operating employees.
First, the Board recommended that TC require all major Canadian railways to expedite the implementation of physical fail-safe train controls on Canada’s high-speed rail corridors and on all key routes (R22-04). The United States has fully implemented a positive train control system on all high-hazard track required by its federal legislation. This includes the United States operations of both CN and Canadian Pacific Kansas City Railway Company (CPKC), which have invested significantly in their locomotive fleets and infrastructure. This accident highlighted major issues in the rail industry and reinforced the TSB’s call for physical fail-safe train controls for over two decades through recommendations R13-01 and R00-04. The railway industry must act more quickly to implement a similar form of automated or enhanced train control system on Canada’s key routes to improve rail safety and avoid future rail disasters.
Second, the Board recommended that TC require Canadian railways to develop and implement formal crew resource management as part of the qualification training for railway operating employees (R22-05). This type of training could provide additional tools and strategies to train crews to mitigate inevitable human errors, and provide significant safety benefits in the rail industry.
The issue of following railway signal indications has been on the TSB Watchlist since 2012. If railway signals are not consistently recognized or followed, there is a risk of train collisions or derailments that can have catastrophic consequences.
The issue of fatigue management in freight train operations has been on the TSB Watchlist since 2016.
The issues identified in this investigation also highlighted two recurring TSB Watchlist issues: following railway signal indications and fatigue management.
Following this occurrence, CN distributed a system notice throughout its Canadian operations warning train crews that there was an increase in occurrences where crews failed to stop at signal indications requiring them to do so, primarily due to a lack of focus on situational awareness.
Failure of a misaligned rail joint led to the derailment of a crude oil train
In its investigation report, the TSB determined that a recently replaced rail joint failed as a result of a misaligned joint bar, causing the derailment of a crude oil train near St-Lazare, Manitoba, in 2019 (R19W0050).
The misalignment led to a loosening of the joint and initiated fatigue cracking in the joint bars that failed beneath the train as it traversed the area. A total of 17 of the derailed tank cars were breached, which resulted in the release of about 815 000 litres of product. About 1000 feet of track was damaged or destroyed.
The failed joint had been repaired about six weeks prior to the accident. However, during the repair, a compromise joint bar, an offset joint bar used for joining two rails of different sizes that looks similar to a standard joint bar, was inadvertently installed with a standard joint bar. A joint assembled in this manner is unstable, will loosen over time, and can result in premature failure such as in this occurrence.
Following this accident and two additional serious CP crude oil unit train derailments near Guernsey, Saskatchewan (R19W0320 and R20W0025), the TSB issued Rail Safety Advisory Letter 02/20 and Rail Safety Advisory Letter 03/20 to TC . In response, TC issued Ministerial Orders instructing the industry to develop revised Rules Respecting Key Trains and Key Routes and Rules Respecting Track Safety. The rules were subsequently revised and now contain a number of safety improvements related to the operation of key trains and track infrastructure.
Since this accident, CN now requires the outside surface of all compromise joint bars that are exposed when installed in track to be spray-painted royal blue by the supplier. This allows compromise joint bars to be more easily differentiated from standard joint bars.
From 01 March to 31 December 2019, on the Rivers Subdivision, CN eliminated a total of 1019 temporary plug rails (2038 rail joints) and installed 192 867 feet of continuous welded rail.
Board safety concern about Ontario’s safety oversight of its provincially regulated railways
As a result of its investigation into a 2019 accident in which a GO Transit commuter train struck and seriously injured an adult and a child at a public crossing in Kitchener, Ontario (R19T0191), the Board issued a safety concern stating that the Province of Ontario does not provide effective safety oversight of provincially regulated railways.
The investigation was completed by the TSB at the request of the Ministry of Transportation of Ontario (MTO), as provincial railways fall outside of the mandate of the TSB.
Although the MTO is responsible for the safety oversight of provincially regulated railways such as Metrolinx, it has no overall provincial regulatory framework in place and relies on inspection agreements with TC and Metrolinx to aid in complying with the standards set out in federal rules and regulations. Moreover, the MTO does not have employees with technical railway knowledge, experience, and expertise.
While the MTO can outsource inspections to TC, it cannot outsource the responsibility for the safety of rail operations. Therefore, while TC inspectors can identify safety hazards and aid Metrolinx in mitigating the risks, it does not have the authority to compel them to take remedial action.
Despite the clear need for thorough safety oversight, as it is vital in identifying and addressing risks present at crossings, none of the parties involved – CN, Metrolinx, the Region of Waterloo, or the MTO – were aware of the observed hazards that existed at the crossing.
Given the complexity of multiple separate agreements with different parties, this accident demonstrates that there are gaps in the Province of Ontario’s regulatory surveillance of its provincially regulated railways.
In 2021, the TSB issued Rail Safety Advisory Letter 01/21 to TC regarding second-train events at multi-track level-grade crossings that have a high level of pedestrian traffic and experience frequent and extended grade crossing warning device activations. The advisory suggested assessing the likelihood of second-train events and implementing additional safety measures to minimize the risk of accidents.
Following the accident, Metrolinx made several physical safety improvements at the Lancaster Street West crossing, and now requires train operators approaching the crossing to sound the horn if it is occupied by another train.
Since the accident, the MTO identified a need to update the oversight framework for urban and regional rail transit that would better support the province’s growing rail network and the diversity of operators. In January 2022, the MTO updated its agreements with both TC and Metrolinx. In making these updates, the MTO worked closely with TC to strengthen the MTO’s accountability role in the agreement, with respect to Metrolinx, to verify that non-compliances and deficiencies that may arise are appropriately addressed.
Employee fatality at Canadian National Railway Company’s MacMillan Yard caused by a string-line derailment
In April 2022, the TSB released its investigation report into a 2019 derailment at CN’s MacMillan Yard, Vaughan, Ontario, that resulted in the death of a railway yard operating employee (R19T0147). The employee was manoeuvring a remote control locomotive system (RCLS) yard assignment using a beltpack and was stationed on the left side of the leading end of the 27th car of the movement. As the assignment negotiated a 15-degree left-hand curve, the trailing end of the 26th car behind the locomotives string-lined, causing it to derail along with the next eight cars. String-lining is the tendency of a long cut of cars to shortcut a curve when being pulled, a problem that is amplified in a heavier train when handling light cars that are followed by significantly heavier cars. All nine cars that derailed were empty multi-level autorack cars.
The investigation found that, when the trailing end of the 26th car string-lined, the car derailed to the inside of a 15-degree curve. As it derailed, the 26th car pulled sideways on the 27th car, causing cars 27 to 29 to overturn to the inside of the curve, pinning the employee and causing fatal injuries.
A series of train dynamic simulations were conducted in support of the investigation. The results identified that the RCLS programming caused an aggressive throttle response that, in turn, led to a rapid acceleration and run-out of train slack on the long tail-end heavy assignment. It was also determined that, since a lighter cut of autorack cars equipped with hydraulic end-of-car cushioning devices was placed between two heavy cuts, the devices were compressed during the previous deceleration. Therefore, the aggressive acceleration of the assignment likely resulted in a rapid run-out of train slack, which contributed to the string-line derailment. Additionally, it was found that the air brakes likely remained on the 63rd car, which also contributed to the accident.
If railways do not reinforce safe, smooth train handling options for RCLS use during yard operations and provide more specific guidance for identifying conditions that are conducive to string-line events, the risk for a string-line event will remain.
Following the accident, TC completed an investigation under the Canada Labour Code, Part II. CN, for its part, implemented several new processes system-wide, revised instructions for MacMillan Yard, and re-configured a portion of the track in an effort to prevent similar accidents from occurring in the future.
Safety advisories and safety information letters
The TSB issued six rail transportation safety advisories as part of its investigations in 2022–23.
Operational experience of employees paired for remote control locomotive system yard assignments
As part of Rail Transportation Safety Occurrence R22T0060 into a collision between an RCLS yard assignment and a stationary yard assignment in CPKC Railway’s Toronto Yard in Toronto, Ontario, the TSB issued Rail Transportation Safety Advisory Letter 02/22 to TC in July 2022. The letter stated that TC might wish to consider an alternate approach to the pairing of employees to work RCLS yard assignments to ensure that newly qualified employees are mentored by more experienced employees until they gain sufficient expertise to operate safely.
Trespassing on the Canadian Pacific Railway Company’s Outremont spur
As part of Rail Transportation Safety Occurrence R22D0058 into the striking of a pedestrian trespassing on the up track near the Outremont spur in Montréal, Québec, the TSB issued Rail Transportation Safety Advisory Letter 03/22 to TC in August 2022. The letter stated that TC might wish to consider reviewing the risk management measures in place against trespassing on the Outremont spur (monitoring by CP, no trespassing signage, community awareness programs, and a fence repair program) and updating these measures as necessary.
Procedures and guidelines relating to train operations
As part of two rail transportation safety occurrences (R22Q0095 and R22Q0062) into derailments of Quebec North Shore and Labrador Railway (QNS&L) trains with locomotives that were equipped with alternating current traction motors, the TSB issued Rail Transportation Safety Advisory Letter 04/22 in November 2022 to TC. Although the QNS&L general operating instructions contain guidelines for the use of air brakes and warnings about slack action when operating trains, there are currently no specific instructions for the use of dynamic brakes, particularly on AC locomotives. The letter stated that TC might wish to consider reviewing QNS&L’s procedures and guidelines for the use of dynamic braking, especially when operating trains that are equipped with locomotives with alternating current traction motors.
Ongoing failures of cartridge roller bearing assemblies on Ottawa Light Rail Transit vehicles
As part of Rail Transportation Safety Occurrence R22H0037 into the failure of a cartridge roller bearing assembly on an Ottawa Light Rail Transit (OLRT) light rail vehicle (LRV), the TSB issued Rail Transportation Safety Advisory Letter 01/23 in February 2023 to the City of Ottawa. At the time the letter was issued, there had been two serious main-track derailments and a near-catastrophic component failure that all involved OLRT LRV cartridge assemblies. While the materials used to manufacture the cartridge assemblies conformed to the manufacturer’s specifications, the three cartridge assemblies examined by the TSB exhibited numerous types of failures. The observed damage was widely spread throughout the assemblies and was not limited to any one particular component. Furthermore, areas of heat discolouration observed on several components and the condition of some grease samples suggested that the assemblies had been subjected to a higher-than-average heat event that was likely related to a deteriorating cartridge assembly condition that went undetected. The letter stated that the City of Ottawa might wish to ensure that all parties involved in the OLRT work together to resolve design, operational, and maintenance risks to safety, as they emerge. Furthermore, the parties involved should ensure that effective on-board monitoring systems for safety-critical LRV components, such as cartridge roller bearing assemblies, are put in place to protect the travelling public.
Deficient track conditions on Canadian Pacific Railway Company’s Swift Current Subdivision
As part of Rail Transportation Safety Occurrence R23S0009 into the derailment of a CP train on the Swift Current Subdivision near Chaplin, Saskatchewan, the TSB issued Rail Transportation Safety Advisory Letter 02/23 in February 2023. According to documentation provided by CP, the track in the vicinity of the derailment had been inspected in accordance with the Rules Respecting Track Safety and CP’s Red Book of Track & Structures Requirements. The most recent visual track inspection (13 January 2023), heavy track geometry inspection (05 December 2022), and rail flaw detection (RFD) testing (29 December 2022) did not identify any defects in the area.
The most recent TC inspection of the Swift Current Subdivision before the derailment had been conducted in October 2022. During this inspection, the area of the point of derailment on the main track between the siding switches was not inspected. Following the inspection, TC issued a letter to CP identifying 10 non-compliance defects and 60 areas of concern, most of which were for track gauge conditions. CP responded to TC that the non-compliant defects had been repaired and that the areas of concern would be monitored and corrected in 2023 or 2024.
During site activities after the derailment, TSB investigators visually inspected the track in the vicinity of the point of derailment and identified the presence of rail corrugation and seven track deficiencies.
The safety advisory letter stated that, given the condition of the track observed by the TSB near the derailment, there might be gaps in CP’s track inspection and maintenance programs as well as TC’s track inspection and follow-up for the section of track. The letter further stated that TC might wish to perform a thorough review of CP’s track inspection and maintenance practices and conduct a detailed regulatory inspection of the entire Swift Current Subdivision.
Progress on outstanding recommendations
Of the 14 responses to rail transportation safety recommendations the Board assessed in 2022–23, one was closed as Fully Satisfactory. Of the other 13 responses, seven were assessed as Satisfactory Intent, four were Satisfactory in Part, and two were unable to be assessed.
Recommendation R20-01 is related to the Watchlist 2022 issue of unplanned/uncontrolled movements of railway equipment, as well as to Recommendation R14-04 (physical defences to prevent runaway equipment). The Board acknowledged the significant safety action taken to date by both TC and industry: changes to the Canadian Rail Operating Rules, revisions to the Railway Locomotive Inspection and Safety Rules, a joint workshop to assess the effectiveness of measures taken and explore next steps, an online consultation on a proposal to modernize the Railway Employee Qualification Standards Regulations, and further research on human factors and new technologies. However, the desired outcome of significantly reducing the frequency and associated risks of uncontrolled movements while switching without air has not yet been achieved. In 2022, there were 23 uncontrolled movements related to switching without air, a number slightly greater than the average for 2010 to 2022 (20) and greater than the number of occurrences in 2020 and 2021 (19 and 16, respectively). Therefore, the Board assessed the response to the recommendation as showing Satisfactory Intent.
Since the TSB first issued Recommendation R15-03 in December 2015, TC has taken several steps toward the eventual implementation of dedicated, crashworthy event data recorders (EDRs) on commercial passenger buses, and has been working to establish international consensus on a baseline standard for heavy vehicle event data recorders (HVEDRs) to ensure harmonization with the United States. TC has been developing a guidance document on HVEDRs, with an expected publication date in winter 2023. The purpose of this document is to provide best practices and lessons learned for the construction and installation of HVEDRs to truck and bus manufacturers, tier suppliers, fleet managers, and drivers. The Board recognized TC’s efforts toward the development and adoption of the SAE J2728 standard. However, the Board was concerned that no timelines for the completion of next steps to introduce HVEDRs to Canadian commercial passenger vehicles had yet been established, and that there was no clear workplan for the roll-out of planned changes to the Canada Motor Vehicle Safety Standards. Therefore, the Board was unable to assess the response to the recommendation.
Recommendation R15-02, one of five recommendations issued in December 2015 as a result of the fatal collision between an OC Transpo transit bus and a VIA Rail train in Ottawa, Ontario (R13T0192), relates to the development and implementation of crashworthiness standards for commercial passenger buses. TC completed a multi-year transit bus crashworthiness program in the fall of 2022. As a result of the department’s research, TC has concluded that it would not be prudent to incorporate structural crashworthiness standards for transit buses into the Canada Motor Vehicle Safety Standards due to the potential for negative impacts on occupant safety. TC has instead refocused its efforts on occupant protection; its research has demonstrated that there are opportunities to improve the protection of occupants in low-to-moderate severity transit bus collisions. The Board notes that TC continues to progress research and development in the area of occupant protection and is planning to publish a guidance document by the spring of 2024. However, beyond this future guidance document, there is an absence of specificity and timing with respect to action that will reduce the risk of injury to occupants of commercial passenger buses in the event of a collision. Therefore, the Board is unable to assess the response to the recommendation.
For all active recommendations, the TSB will continue to monitor the progress of planned actions and call for action to reduce or eliminate these deficiencies.
Who we are and what we do
The TSB advances transportation safety in the air, marine, pipeline, and rail transportation sectors in Canada:
- It conducts independent investigations into selected occurrences and makes findings about their causes and any contributing factors.
- It identifies safety deficiencies arising in transportation occurrences and makes recommendations to eliminate or reduce them.
- It reports publicly about its investigations and findings.
As part of its investigations, the TSB reviews developments in transportation safety and identifies safety risks that governments and the transportation industry must address in order to reduce the risk of injury and loss.
Role of the Board
The Board, which comprises up to five members, including the Chair, approves all investigation reports, makes findings, and issues recommendations.
The Board
Chair
Board member
Board member
Board member
The TSB website contains biographies of each Board member. On December 31, 2022, long standing part-time Board Member Faye Ackermans retired after serving a total of three terms.
In making findings, the Board does not assign fault or determine civil or criminal liability for an occurrence. Rather, it seeks to find out what happened and why in an objective manner, independent from government and all other departments and agencies involved in transportation, and free from any conflict of interest. It also draws impartial conclusions and makes recommendations to those best placed to act.
About the TSB
A staff of 227, led by the Chief Operating Officer and senior management, supports the Board. The work of the organization is guided by a five-year strategic plan and five core values:
- Respect: We are committed to inclusiveness and to treating all individuals and organizations with consideration, courtesy, discretion, and fairness.
- Openness: We actively share and exchange information to advance transportation safety.
- Safety: We maintain and promote a positive and proactive safety culture.
- Integrity: We are guided by honesty, transparency, impartiality, propriety, and accountability for our actions and decisions.
- Excellence: We maintain a highly skilled and knowledgeable team of professionals through leadership, innovation, and commitment to continuous improvement in the delivery of our products and services.
TSB investigators are professionals with years of experience in the various transportation modes the TSB covers. They work in collaboration with engineering and technical specialists, human factors investigators and industry analysts, all of whom are supported by small teams of communications specialists, corporate services professionals ,and administrative officers.
The TSB’s head office is in Gatineau, Québec. The TSB also has a laboratory in Ottawa, and regional offices in Vancouver, Edmonton, Calgary, Winnipeg, Toronto, Montréal, Québec, and Dartmouth.
The investigation process
There are three main phases of the investigation process. During the field phase, investigators collect data and assess the occurrence. This generally involves travelling to the scene of the occurrence, securing the site and documenting it, conducting interviews and selecting wreckage for further examination. Unless the investigation is limited to data collection, an investigation page is created and posted to the website, and is updated periodically as the investigation progresses.
During the examination and analysis phase, investigators review the data to determine the sequence of events leading to the occurrence and the underlying causes and contributing factors.
In the report phase, investigators draft a report on the investigation, which then goes through a review and approval process, prior to public release.
Appendices
Appendix A: Investigation reports released in 2022–23 and related safety actions
The following is a list of the investigation reports TSB released during 2022–23. Each entry includes details of any safety actions taken during the investigation and after the report was published, and a link to the main page for the investigation. The list is organized by transportation sector and in the order in which the occurrences took place.
These safety actions taken by industry stakeholders and regulators in the air, marine, pipeline, and rail transportation sectors are the tangible outcome of the TSB’s investigative work to advance transportation safety. Their efforts as a result of our findings contribute to making our transportation system even safer.
Air transportation sector
INVESTIGATION REPORT A19C0145: Controlled flight into terrain, North Star Air Ltd. Douglas DC3C Basler Turbo Conversions TP67, C-FKAL, Sachigo Lake Airport, Ontario, 03 December 2019
| SAFETY ACTIONS | Following the occurrence, North Star Air Ltd. implemented a flight operations quality assurance program. In December 2020, TC conducted a process inspection (PI), focusing on the evaluation and effectiveness of the long-term corrective action plan related to the flight operations findings from the December 2019 PI. TC concluded that the long-term corrective actions taken by North Star Air Ltd. were effective. |
|---|
INVESTIGATION REPORT A19P0142: Main rotor blade failure and collision with terrain, E & B Helicopters Ltd. Bell 206B (helicopter), C-GEBY, Campbell River, British Columbia, 24 September 2019
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A20C0107: Runway excursion, Calm Air International LP, Avions de Transport Régional ATR 42-300, C-FAFS, Naujaat Airport, Nunavut, 26 November 2020
| SAFETY ACTIONS | On 09 December 2020, Calm Air International LP issued Flight Operations Bulletin 2020-07, which describes a condition known as “pitch lock.” It further describes:
In February 2021, the operator introduced to its ATR 42 recurrent simulator training scenarios in which the propeller enters a pitch-lock condition. |
|---|
INVESTIGATION REPORT A20O0029: Runway incursion – risk of collision, NAV CANADA Toronto Control Tower and Air Canada Embraer ERJ 190-100 IGW, C-FMZW and Air Canada Boeing 777-333ER, C-FJZS, Toronto/Lester B. Pearson International Airport, Ontario, 07 March 2020
| SAFETY ACTIONS | On 30 November 2020, the TSB issued Aviation Safety Advisory A20O0029-D1-A1 to highlight the importance of accurate flight status data being validated and transmitted by transponders and how this data is received, validated, and used by runway monitoring and conflict alert (RMCA) systems to ensure maximum safety benefit. The safety advisory encouraged manufacturers of aircraft transponder systems and of advanced surface movement guidance and control systems (A-SMGCSs) with RMCA systems, along with certification authorities and air traffic service providers, to work together to ensure that these systems interact effectively to transmit, receive, and validate an accurate airborne status and that alerts work as intended to reduce the risk of collisions on runways. On 08 December 2020, NAV CANADA published Urgent Air Traffic Control Information Bulletin (2020-003) for all Toronto Tower personnel. The bulletin cautioned controllers that runway incursion monitoring and conflict alert sub-system (RIMCAS) stage 1 and stage 2 alerts may not be generated when Embraer E-jets and some aircraft manufactured by Dassault, Gulfstream, Learjet, and Textron Aviation (formerly Cessna) are departing. The bulletin also advised that stage 1 and stage 2 alerts may not be produced for aircraft or vehicles approaching the active runway when one of these aircraft types is departing, and reminded to monitor these situations closely. On 03 May 2021, TC published Civil Aviation Safety Alert (CASA) No. 2021‑03 to raise awareness to aircraft owners, operators, and air navigation services providers of the potential for inaccurate airborne status transmitted by transponders and its effect on runway monitoring and conflict alert (RMCA) systems. On 20 December 2021, TC published an update to CASA No. 2021-03. The changes address potential variability of transponder airborne status thresholds, their variability from aircraft to aircraft, and how these can be adjusted by the original equipment manufacturers and not specifically the transponder manufacturers. |
|---|
INVESTIGATION REPORT A21A0024: Stall and collision with terrain, Forest Protection Limited, Air Tractor, Inc. AT-802, C-GJJX, Popple Depot, New Brunswick, 11 August 2021
| SAFETY ACTIONS | After the occurrence, Forest Protection Limited revised its Fire Suppression Manual in a focus group with its most experienced fire suppression pilots and in consultation with the Provincial Forest Firefighting Centre. The manual was amended to include the following new practices:
Forest Protection Limited also amended its training to include:
|
|---|
INVESTIGATION REPORT A21C0078: Loss of control and collision with terrain, MAG Aerospace Canada Corp., Rockwell International Aero Commander 690B, C-GYLD, Thunder Bay Airport, Ontario, 16 August 2021
| SAFETY ACTIONS | Following the occurrence, MAG Aerospace Canada Corp. (MAG Canada) took the following safety actions:
|
|---|
INVESTIGATION REPORT A21O0056: Wire strike and collision with terrain, Apex Helicopters Inc., Robinson R44 (helicopter), C-FVPA, Brantford, Ontario, 25 July 2021
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A21O0069: Mid-air collision, York Regional Police DJI Matrice M210 (remotely piloted aircraft), C-2105569275, and Canadian Flyers International Inc. Cessna 172N, C-GKWL, Toronto/Buttonville Municipal Airport, Ontario, 1.2 NM NW, 10 August 2021
| SAFETY ACTIONS | The York Regional Police has amended its Command Directive LE-388 to include the addition of a pre-flight risk assessment tool and an updated Remotely Piloted Aircraft Pilot Checklist. There is also additional guidance for the role of visual observer, including a quick reference card outlining their roles and responsibilities, as well as a requirement to have a visual observer present for all operational remotely piloted aircraft flights. |
|---|
INVESTIGATION REPORT A21O0085: Loss of control and collision with terrain, Privately registered Mooney M20J, C-FLJL, Sundridge/South River Airpark, Ontario, 16 September 2021
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A21O0127: Runway overrun, I.M.P. Group Limited, Embraer EMB-505 (Phenom 300E), C-GRIA, Kingston/Norman Rogers Airport, Ontario, 30 November 2021
| SAFETY ACTIONS | The aircraft operator, I.M.P. Group Limited, has updated procedures to include the task of notifying the airport operator of planned arrivals when environmental conditions may be affecting the runway condition, and to require pilots to request updated runway condition reports if conditions warrant. |
|---|
INVESTIGATION REPORT A21P0018: Loss of control and collision with terrain, Airspan Helicopters Ltd.. Bell 212, C-GNYI, Bowen Island, British Columbia, 05 March 2021
| SAFETY ACTIONS | As a result of the accident, Airspan Helicopters Ltd.:
|
|---|
INVESTIGATION REPORT A21P0069: Loss of control at liftoff and overturn, Atleo River Air Service Ltd. Cessna A185F, C-GYJX, Tofino Harbour Water Aerodrome, British Columbia, 26 July 2021
| SAFETY ACTIONS | Atleo River Air Service Ltd., through its scheduling, has increased the time between flights by an additional 15 minutes to provide the pilots with more time to complete their pre-flight duties. |
|---|
INVESTIGATION REPORT A21P0111: Collision between an aircraft and a water taxi, Tofino Air de Havilland DHC-2 MK. I (Beaver), C-FMXR, and Eagle Adventures Water Taxi water taxi C12997BC (Rocky Pass), Tofino, British Columbia, 18 October 2021
| SAFETY ACTIONS | On 08 February 2022, the TSB issued Marine Safety Information Letter MSI 01/22 advising TC that there are no speed limits for vessels in the Tofino harbour and that the local authorities in Tofino were unaware of the Vessel Operation Restriction Regulations (VORR). TC responded to the TSB by reiterating that the local authority has the responsibility to apply for vessel operations restrictions. TC does not plan to take further action to raise awareness about the VORR. Since the accident, flight training at Tofino Air has included more complete scanning techniques (moving torso to scan, scanning to pick up on any stationary object illusions, and addressing blind spots) and a “landing scan” check box was added to Tofino Air’s flight training form. On 04 November 2021, the pilot completed additional training on emergency procedures, including the different types of personal flotation devices and their limitations. On 26 April 2022, TC reached out to the Nuu-chah-nulth Tribal Council regarding occurrences in and near the Tofino harbour in 2021 and early 2022. TC offered a follow-up discussion to share information about the current regulatory regime and better understand the Council’s perspectives about transportation safety in the Tofino area. |
|---|
INVESTIGATION REPORT A21P0124: Loss of control and collision with terrain, Privately registered Cessna R182, C-FBKJ, Hope Aerodrome, British Columbia, 18 NM NE, 15 November 2021
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A21Q0024: Collision between sling load and tail rotor, Héli-Express Inc. Airbus AS350 B2 (helicopter), C-GHEX, Les Escoumins, Quebec, 1.5 NM NNE, 11 May 2021
| SAFETY ACTIONS | Following this accident, Hydro-Québec
|
|---|
INVESTIGATION REPORT A21Q0083: Loss of control and collision with terrain, Privately registered Piper J3C-65 (floatplane), CF-SVT La Tuque Aerodrome, Quebec, 25 NM ENE, 12 September 2021
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A21Q0090: Collision with water and capsizing, Privately registered Piper PA-18S-150 (floatplane), C-FVPZ, Rivière du Lièvre, Ferme-Neuve, Quebec, 24 September 2021
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A21Q0092: Loss of engine power and collision with terrain, Publicité AERO-GRAMME Inc. Cessna 172M, C-FFRV, Montréal/Pierre Elliott Trudeau International Airport, Quebec, 8.45 NM E, 02 October 2021
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A21W0001: Collision with terrain, Privately registered Robinson R44 Raven II (Helicopter), C-FBGT, Grande Prairie, Alberta, 39 NM NE, 01 January 2021
| SAFETY ACTIONS |
|
|---|
INVESTIGATION REPORT A21W0045: In-flight breakup, Yellowhead Helicopters Ltd. Bell Textron Inc. 212 (helicopter), C-GYHQ, Evansburg, Alberta, 4 NM WNW, 28 June 2021
| SAFETY ACTIONS | On 05 July 2021, Bell Textron Inc. (Bell) issued 4 alert service bulletins covering model 204B, 205, 205B, and 212 helicopter fleets. The alerts required the review of the aircraft’s technical record to determine if any main rotor hub strap retaining pins with the serial number prefix FNFS were installed. If pins with the affected prefix were installed, they were to be replaced with pins of a different serial prefix before further flight. On 05 July 2021, TC issued an emergency airworthiness directive (CF-2021-23) mandating compliance with the Bell alert service bulletins affecting model 204, 205, and 212 aircraft fleets in Canada before further flight. On 06 July 2021, the U.S. Federal Aviation Administration (FAA) issued an emergency airworthiness directive (AD 2021-15-51), mandating compliance, before further flight, with Bell alert service bulletins affecting model 204, 205, and 212 aircraft fleets. In March 2022, the FAA issued a follow-on AD (AD 2022-06-03), which included the Bell 210 model and clarified wording in the original AD. On 08 July 2021, the European Aviation Safety Administration (EASA) issued an emergency airworthiness directive (AD 2021-165-E), mandating the replacement of main rotor hub strap pins with the serial number prefix FNFS on European-registered model 204, 205, and 212 aircraft fleets before further flight. On the evening of 28 June 2021, shortly after the occurrence, Yellowhead Helicopters Ltd. stood down all aircraft operations. On the afternoon of 29 June 2021, the Bell 206 and Airbus AS350 fleets were returned to service. The Yellowhead Helicopters Ltd. Bell 212 fleet remained grounded until the Bell alert service bulletin 212-21-165 was issued, and it had been confirmed that the remaining aircraft did not have main rotor hub strap retaining pins with the affected serial number range installed. The Bell 212 fleet was returned to service on the afternoon of 05 July 2021. |
|---|
INVESTIGATION REPORT A21W0089: Collision with terrain, Privately registered Cavalier SA102.5 (amateur-built aircraft), C-FBWF, Lacombe Aerodrome, Alberta, 14 NM E, 09 October 2021
| SAFETY ACTIONS | On 11 January 2023, the Transportation Safety Board of Canada issued Air Transportation Safety Advisory Letter A21W0089-D2-A1 to TC. The letter informs TC that not all physicians are aware of the requirement to report medical issues for their patients that hold a pilot licence. It also encourages TC to work with the Canadian Medical Association to develop communication strategies to increase the awareness of the reporting requirements for physicians under the Aeronautics Act. On 19 January 2023, TC responded to the TSB’s Safety Advisory Letter A21W0089-D2-A1. It its response, TC stated that TC Civil Aviation Medicine had coordinated with the Canadian Medical Association to increase awareness of the reporting requirements for physicians. Safety action required: Screening tools for pilot medical exams On 09 October 2021, the privately registered, amateur-built Cavalier SA102.5 aircraft (registration C-FBWF, serial number 6958) was conducting a local recreational flight from Lacombe Aerodrome, Alberta, with 1 pilot and 1 passenger on board. When the aircraft was 14 nautical miles east of the aerodrome, it entered an aerodynamic stall, resulting in a left-hand spin and collision with terrain. The pilot, who was seated in the left seat, was fatally injured; the passenger received serious injuries. The aircraft was substantially damaged; there was no post-impact fire. The Office of the Chief Medical Examiner in Alberta reported that the cause of death was attributed to blunt force trauma with cardiovascular disease as a significant contributing factor. The report also noted that the pilot had evidence of a heart attack, although it was not possible to determine the exact time of this event. The pilot’s Category 1 medical certificate, which was valid until 01 February 2022, did not list any limitations. The occurrence pilot, who was older than 40, regularly attended a TC medical examination every 12 months as required for his airline transport pilot licence. For each visit, a medical examination report was completed as required. However, for his most recent medical certificate, issued in 2021, the pilot did not undergo a medical examination. Instead, he completed and signed an attestation that he did not have any limitations or restrictions or other conditions that could impair his ability to exercise the privileges of the licence. This attestation was allowed in accordance with an exemption issued by TCFootnote 1 due to the global COVID-19 pandemic. There was no cardiovascular risk profiling performed as part of any of the pilot’s medical examinations. However, using data from the Civil Aviation Medical Examiner (CAME) medical examinations, the blood lipids from the family physician’s records, and various risk-profiling methods, including the Framingham risk scoring tool, an independent cardiology review performed for this investigation confirmed that the pilot’s calculated annual risk for a cardiovascular event was approximately 1% per year. This is considered a low-to-average risk for his age, and acceptable for commercial pilot operations. Even if the CAME had performed risk profiling, these results would not have triggered secondary screening testing for underlying coronary disease. The independent cardiology review highlighted that, although most cardiovascular disease is indicative via blood lipids, some 10–20% of heart attack victims do not present with these traditional risk factors. Therefore, cardiologists advise that other mechanisms may also be required to screen for coronary atherosclerosis. For example, elevated lipoprotein Lp(a) has been identified as a significant additional hereditary risk factor in some individuals. Lipoprotein Lp(a) measurement has been incorporated into the recommended periodic screening for cardiovascular risk.Footnote 2 An independent cardiology review performed for another TSB investigationFootnote 3 highlighted that, based on the consensus of a multinational consortium of aviation cardiologists published in 2019,Footnote 4 cardiovascular risk screening should be required for all pilots over the age of 40, and for those pilots identified to be at an increased risk (based on risk calculation). Such screening should always include an assessment of blood lipids and, in some cases, other methods might be needed for the 10–20% of heart attack victims that do not present with traditional risk factors. Current TC CAME guidelines, which were published in 2012, only recommend—they do not mandate—enhanced screening using laboratory data, such as screening for blood lipids. Given that it is not policy to screen using laboratory data, CAMEs are not required to use such screening for periodic certification examinations, even for those applicants over the age of 40. The cardiology reviews conducted for both this occurrence and for TSB Air Transportation Safety Investigation A19P0142 indicate that the TC Civil Aviation Medicine Cardiovascular Guidelines from 2012 have not been updated to include the significant advances in the recommended approach to screening for coronary atherosclerosis. The cardiology review for this occurrence also stated that options for screening could include blood lipids and potentially enhanced laboratory testing for Lp(a), as well as CT (computed tomography) cardiac imaging where possible. In this occurrence, the cardiologist concluded that if such screening methods were followed, risk factors contributing to the pilot’s heart attack may have been identified. In 2011, following the TSB investigation into a loss of control and collision with terrain that took place in Miramichi, New Brunswick, on 23 April 2010,Footnote 5 the Board issued the following Safety Concern:
In 2012, the TC Civil Aviation Medicine Cardiovascular Guidelines were updated. As of October 2022, there were 32 900 pilots in Canada with Category 1 medical certificates. Of these, 16 607 (approximately 50%) were over the age of 40. Since 2000, there have been 8 accidents, including this one, involving commercial pilots in which cardiovascular disease was identified as a finding as to riskFootnote 6 or finding as to cause.Footnote 7 If TC guidance material and the civil aviation medical examination report do not include up-to-date cardiovascular screening methods to perform a global cardiovascular assessment when appropriate, there is an increased risk that cardiovascular disease will remain unidentified and pilots may become incapacitated while operating an aircraft. Therefore, the Board recommends that the Department of Transport establish a framework for routine review and improvement to the Handbook for Civil Aviation Medical Examiners to ensure it contains the most effective screening tools for assessing medical conditions such as cardiovascular health issues. |
|---|
INVESTIGATION REPORT A21W0090: Loss of control during landing, Privately registered Daher TBM700 N (TBM 910), C-FFYM, Westlock Aerodrome, Alberta, 10 October 2021
| SAFETY ACTIONS | After the accident, TC learned of the pilot’s use of a non-approved prescription medication and suspended the pilot’s medical certificate until further reassessment is completed. |
|---|
INVESTIGATION REPORT A21W0098: Fuel starvation, Air Tindi Ltd. de Havilland DHC-6-300 Twin Otter, C-GNPS, Fort Providence, Northwest Territories, 6.7 NM NW, 01 November 2021
| SAFETY ACTIONS | The following actions were taken by Air Tindi Ltd. after the occurrence:
|
|---|
INVESTIGATION REPORT A22C0016: Collision with terrain, Bamaji Air Inc. Cessna 208 Caravan, C-GIPR, Sioux Lookout, Ontario, 17 NM NNW, 08 March 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22C0027: Loss of control and collision with terrain, Privately registered Piper Cherokee PA-28-140, C-GLKD, Sioux Lookout Airport, Ontario, 19 NM SSE, 29 April 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22C0035: Collision with obstacle on approach, Sandy Lake Seaplane Service Ltd. Cessna U206G, C-GBGJ, Sandy Lake First Nation, Ontario, 26 May 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22O0032: Collision with obstacle on approach, Brantford Flying Club Cessna 172RG, C-GOFD, Brantford Aerodrome, Ontario, 21 March 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22O0046: Collision with terrain, Privately registered Piper PA24-250 (Comanche), C-GEWK, Wawa, Ontario, 11.5 NM SSW, 14 April 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22O0118: Collision with obstacle on takeoff, Privately registered Piper Aircraft Corporation PA-28-180 (Cherokee), C-FYSZ, Canton Aerodrome, Ontario, 13 August 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22O0125: Collision with terrain, Privately registered Grumman Aircraft Engineering Corp. G44 (Widgeon), C-FNGD, Stratford Municipal Airport, Ontario, 1.3 NM ENE, 23 August 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22O0140: Collision with terrain, Privately registered Quad City Ultralight Aircraft Corporation Challenger II (advanced ultralight), C-IYDD, Westport/Rideau Lakes Aerodrome, Ontario, 11 NM WSW, 24 September 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22P0019: Collision with terrain, Kootenay Valley Helicopters Ltd. Airbus Helicopters AS350 B3, C-GWTQ, Nelson, British Columbia, 35 NM N, 16 March 2022
| SAFETY ACTIONS | Following the accident, Kootenay Valley Helicopters Ltd. implemented a policy of in-flight briefing, which was reviewed with all pilots: before starting the approach to a blasting site, the crew must hold a briefing to discuss the suitability of the avalanche start zone, current weather conditions, and the adequacy of visual reference for approach, deployment of the charge, and departure from the blasting site. If, during the approach phase, a new site is selected, the approach is discontinued. A thorough assessment of the new location is subsequently conducted and briefed, and a new approach is initiated. In compliance with WorkSafeBC requirements, the BC Ministry of Transportation and Infrastructure (MOTI) completed an internal investigation of its avalanche control operations. The MOTI examined in-depth several aspects of the operations and arrived at several findings and recommendations pertaining to the work activity, work conditions, execution, materials and equipment, communications, training, safe-work procedures, emergency procedures, personal protective equipment , and other factors such as post-occurrence worker assistance, and general coordination and planning. |
|---|
INVESTIGATION REPORT A22P0061: Collision with terrain, Privately registered Cessna 172P, C-GGSN, Qualicum Beach Airport, British Columbia, 24 July 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22Q0029: Controlled flight into terrain, Airbus AS350 B2 (helicopter), C-GFBW, Sept-Îles Airport, Quebec, 7.5 NM W, 17 March 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22Q0084: Collision with cable, Privately registered Bellanca 7GCBC (Citabria), C-GOQZ, Shawinigan, Quebec, 17 July 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22W0005: Loss of control and collision with terrain, Delta Helicopters Ltd. Bell 206B JetRanger II (helicopter), C-FCQJ Camrose Aerodrome, Alberta, 23 NM ESE, 23 January 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22W0027: In-flight icing and collision with terrain, Privately registered Mooney M20K, C-GQMS, Calgary/Springbank Airport, Alberta, 0.6 NM S, 22 April 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22W0057: Collision with terrain, Privately registered Zlin Aviation s.r.o. Savage Cub (advanced ultralight), C-IILH, Didsbury, Alberta, 7 NM E, 13 July 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT A22W0078: Collision with terrain, Arty’s Air Service Ltd. Air Tractor, Inc. AT-502B, C-FJVL, Bawlf (Blackwells) Aerodrome (CFR2), Alberta, 18 NM S, 12 September 2022
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
Marine transportation sector
INVESTIGATION REPORT M19C0054 : Striking of a mooring dolphin, Roll-on/roll-off ferry Apollo, Matane, Quebec, 16 March 2019
| SAFETY ACTIONS | On 17 March 2019, after boarding the Apollo, the TSB notified TC that there were safety issues on the vessel relating to the vessel’s watertight integrity, electrical wiring, and firefighting system. On 17 May 2019, the TSB followed up with TC by issuing Marine Safety Advisory Letter 01/19 about the safety issues. The TSB requested to be informed of any action taken by TC. A response was received on 14 June 2019 that indicated that TC had inspected the Apollo on 21 March 2019 and had issued a restriction from sailing. Following the occurrence, the Société des traversiers du Québec (STQ) conducted a risk assessment and internal investigation. The report from the internal investigation found that the bow thruster was not functioning and that the master did not have indicators allowing him to determine the wind speed, the rpm of the main engines and bow thruster, or the vessel’s course over ground, all of which were essential for him to judge the situation and effect an adequate manoeuvre. The STQ’s report also made mention of a general pressure that was present, especially after the earlier striking in February 2019, that mostly related to the vessel’s operation and came from both internal sources (as a result of a desire to continue offering service on this route) and external sources (as a result of media coverage). The report made the following recommendations:
In response to the recommendations, the STQ took the following actions:
|
|---|
INVESTIGATION REPORT M19C0403: Engine room fire, Bulk carrier Tecumseh, Detroit River, Windsor, Ontario, 15 December 2019
| SAFETY ACTIONS | On 26 June 2020, the TSB issued Marine Safety Advisory Letter No. 01/20, entitled “Shipboard firefighting capabilities of fire departments neighboring Canadian ports” to the Association of Canadian Port Authorities, copying related authorities. The letter highlighted the fact that few Canadian ports have access to fire brigades that are trained in marine firefighting and that the lack of training prevents firefighters from boarding vessels to help with suppression of shipboard fires. The letter also identified that few shore-based fire brigades are aware of the existence of international shore connections. Finally, the letter noted that few Canadian port authorities have emergency preparedness plans to address firefighting on board vessels docked at the port. In June 2022, TC began revising the advanced firefighting portion of the current TP 4957 Marine Emergency Duties training courses to include additional mandatory knowledge requirements about how to monitor before re-entering a compartment following a fire. Lower Lakes Towing Ltd. took the following safety actions:
In 1996, following a fire on board the self-unloading bulk carrier Ambassador, the Board identified concerns with training of shore-based fire brigades. In response, the Board recommended that the Department of Transport, in collaboration with ports and harbour authorities, take measures to ensure that shore-based fire brigades expected to support on-board firefighting, receive appropriate training. Following this recommendation, the Canadian Association of Fire Chiefs (CAFC), with the assistance of TC, circulated a short questionnaire to assess the firefighting capabilities of municipal fire departments responsible for fighting fires in Canadian ports. In February 1998, in light of preliminary information coming from a subsequent investigation into an explosion and fire on board the tanker Petrolab, the TSB issued Marine Safety Advisory 03/98 to TC and the CAFC. They were asked to expedite their safety audit and review of risks and contingency measures in Canadian ports and harbours that contained oil terminals and wherever the installations were more susceptible to catastrophic damage should a fire break out on board a vessel at the dock. By July 1998, the CAFC had received a limited response to the survey questionnaire. However, the CAFC found that the survey provided enough information to raise concerns that the firefighting services available in municipalities with public ports might not be adequate to provide firefighting services in the event of a fire on board a vessel. The CAFC indicated that it was interested in working with TC to pursue research in this area. Following a fire on board the bulk carrier Windoc in August 2001 that resulted in the vessel’s total constructive loss, the TSB found that, among other factors, the responding fire department’s lack of training and experience in fighting shipboard fires hindered an effective firefighting response. When Recommendation M96-07 was issued in 1996, TC had regulatory authority over most of Canada’s ports but had begun to transfer port facility ownership and operations to interested parties. In 1998, control of 18 ports was transferred to individual Canada Port Authorities (CPAs),Footnote 8 which operate at arm’s length from the federal government. Although the CPAs fall under the Canada Marine Act and its associated regulations, they operate as self-sufficient commercial entities with no federal funding. Since then, the responsibility for port operations, including the responsibility for shore-based firefighting, was moved to the individual port authorities. Recommendation M96-07 was closed in March 2016, with the Board’s final assessment of the response being Satisfactory in Part; the Board noted, however, that the safety deficiency remained in some ports. The Board also noted that the responsibility for firefighting now rested with individual port authorities, and that it would take into account the effectiveness of the ports’ responses to a ship-based fire in future investigations. During the investigation into the Tecumseh, similar issues arose to those highlighted in Recommendation M96-07, which again raises concerns about the current status of training for shore-based fire brigades. For example, the investigation confirmed that the Windsor Fire Service did not have staff specifically trained for fighting shipboard fires, and that the Windsor Fire Service would respond to a vessel fire at a dock in the port, but firefighters would not be allowed to board or enter the vessel. As well, the investigation identified that neither the Windsor Fire Service nor the Windsor Port Authority had an international shore connection. On 26 June 2020, the TSB sent Marine Safety Advisory Letter 01/20 to the Association of Canadian Port Authorities and the Port of Windsor about the need for local shore-based firefighting resources to be properly trained and equipped to support crews in fighting shipboard fires. In its response to this letter, the Port of Windsor indicated that, among other things, they were not required to have an international shore connection. The Board believes that shore-based resources must be trained and equipped to respond to major vessel fires in order to minimize the consequences of a fire in the close confines of a port or harbour. Therefore, the Board is concerned that some Canadian ports and harbours authorities may lack the proper equipment, training, and resources to respond effectively to shipboard fires occurring within their jurisdiction, which could result in fires that endanger crews, the general public, property, and the environment. The Board will continue to monitor this issue with a view to assessing the need for further safety action. |
|---|
INVESTIGATION REPORT M20A0160: Sinking and subsequent loss of life, Fishing vessel Sarah Anne, Placentia Bay, Newfoundland and Labrador, 25 May 2020
| SAFETY ACTIONS | Registration raises awareness of the vessel to TC, affording an opportunity for improved safety oversight by the regulator, including providing the owner access to safety initiatives and programs. In addition, accurate and up-to-date registration also provides search and rescue authorities critical information about the vessel and its owner in the event of emergency situations. In August 2021, the TSB issued Marine Safety Advisory Letter 02/21 to the Canadian Council of Professional Fish Harvesters regarding information on the council’s website stating that fishing vessels of less than 15 gross tons were below the size for mandatory Transport Canada registration. No response was received. On 25 May 2020 shortly after midnight, the fishing vessel Sarah Anne, with 4 people on board, departed St. Lawrence, Newfoundland and Labrador, to fish snow crab in Placentia Bay. The Marine Communications and Traffic Services Centre in Placentia, Newfoundland and Labrador, received an overdue report at 1945 that evening. A search was launched using several vessels and aircraft. The bodies of 3 crew members were recovered the following day. The body of the 4th crew member was recovered from the shore on 06 June 2020. The vessel was not found. There were a number of contributing factors involved in the loss of life: no distress call was received, no life raft was available to the crew, personal flotation devices (PFDs) were not worn, the vessel was not monitored by a third party, the vessel was not equipped with an emergency position indicating radio beacon (EPIRB), and the stability limits of the vessel were not known to the crew. The investigation also revealed that thousands more commercial fishing vessels were registered with Fisheries and Oceans Canada (DFO) in the Atlantic Region than were registered with TC. That is, DFO was issuing a license to harvest marine resources commercially without verification that the vessel was correctly registered with TC, the department responsible for surveillance of safety requirements. Commercial vessels must be registered with TC, even those that are not inspected for certification. Vessel registration with TC is not only a legislative requirement of the Canada Shipping Act, 2001, but also it gives TC the opportunity to provide safety oversight and guidance to vessel owners regarding their responsibility for compliance. In addition, up-to-date registration data mean accurate information is available to search and rescue authorities, and reliable data are available for safety regulators and other organizations in the marine safety system. Harvesters are more likely to comply with regulatory requirements related to harvesting resources, partly because DFO upholds its mandate robustly through licence conditions and enforcement measures for non-compliance. In contrast, TC’s less robust enforcement regime means that there are no such direct incentives to register with TC, nor to keep registration information up-to-date. In addition, the investigation identified that communication with fish harvesters in regard to the requirement for registration with TC is inconsistent and not always well understood. Internationally, the importance of current and accurate vessel registration with the safety regulator has also been recognized, and many countries link fishing vessel licenses to vessel registration and inspection. In Canada, the connection between safety considerations and the granting of fishing licenses has long been recognized, but has not been adequately addressed. Driven largely by initiatives created by regional staff, efforts are underway within both TC and DFO to address the issue. Nationally, TC and DFO report that they are each changing their database structures to include the other department’s unique registration number. However, without any enforceable requirements, these initiatives remain an informal arrangement and are not a permanent solution. DFO can continue to issue licenses to harvest marine resources on vessels that do not have a current and accurate TC registration. Since DFO is a part of the Government of Canada, issuing a licence may give fish harvesters the impression that they have satisfied all government requirements before conducting commercial operations. In many countries, including Canada, one solution to coordinating service delivery when an issue falls under the responsibility of one or more departments has been a “whole of government” or “horizontal government” approach. This approach was developed in response to situations where issues are interdependent, such as the safety of the fishing industry, and where the government’s objectives cannot be achieved unless 2 or more departments begin working together. For the Canadian fishing industry, this means TC and DFO must work together to ensure that fish harvesters meet all requirements before they can operate commercially. Given that fish harvesters have more frequent contact with the Government of Canada through DFO, a key step in advancing commercial fishing safety will be using this relationship to promote regulatory compliance with TC safety requirements. If fishing vessels are not registered in a TC register, and there are no mechanisms in place to ensure the accuracy of the register information, there is a risk that fish harvesters will not know about, understand, or adhere to regulations intended to increase fishing safety. Given that current and accurate TC registration is the first step in safety oversight of commercial fishing vessels, the Board therefore recommends that the Department of Fisheries and Oceans require that any Canadian vessel that is used to commercially harvest marine resources have a current and accurate Transport Canada registration. |
|---|
INVESTIGATION REPORT M20A0434: Sinking with loss of life, Fishing vessel Chief William Saulis, 12 nautical miles NNE of Digby, Nova Scotia, 15 December 2020
| SAFETY ACTIONS | Following the occurrence, Yarmouth Sea Products Limited required vessel masters to leave crew lists with the safety officer before departure. On 15 December 2020, the fishing vessel Chief William Saulis was returning from scallop fishing when the Joint Rescue Coordination Centre in Halifax, Nova Scotia, received a signal from its emergency position‑indicating radio beacon (EPIRB), 12 nautical miles NNE of Digby, Nova Scotia. Search and rescue efforts were initiated after the vessel could not be reached via very high frequency (VHF) radio or phone. The body of 1 crew member was recovered; as of December 2022, the other crew members remained missing. The investigation determined that the vessel departed the fishing grounds with unshucked scallops on deck, and the freeing ports were likely covered either mechanically or by scallops, so that water from the heavy beam sea also accumulated on deck. The resulting free surface effect from shifting scallops and water and the rolling motion from the heavy beam sea likely caused the vessel to capsize and sink. Both the Canada Shipping Act, 2001 and the Fishing Vessel Safety Regulations (FVSR) require a vessel’s authorized representative (AR) to provide written safety procedures that familiarize persons on board with various operational and emergency activities. Yarmouth Sea Products Limited (YSP), the AR for the Chief William Saulis, had provided the Chief William Saulis and the other 24 vessels in the YSP fleet with a manual for vessel operations. Most of the safety procedures in the manual were based on templates provided by TC. However, these templates do not cover all required procedures, and the manual did not include all procedures required by regulation. In particular, the manual did not have any written procedures to guide the use of the freeing ports, or for how scallops should be stowed on deck, 2 elements critical for the stability of the Chief William Saulis. The investigation determined that, if guidance provided by TC for written safety procedures required by the Fishing Vessel Safety Regulations, including templates, only partially covers regulatory requirements for effective safety procedures, there is a risk that organizations will not develop complete written safety procedures. For fishing vessels such as the Chief William Saulis, TC’s certification program is the primary oversight mechanism to ensure compliance with regulations. Although written safety procedures are required by regulation, TC does not require them to be approved, does not verify their content during inspections, and does not determine if the crew are knowledgeable about the procedures. TC inspection records indicate that from July 2017 to December 2020, 84 separate inspections were conducted on the 25 vessels operated by YSP. None of the records indicated any deficiencies relating to the vessels’ safety procedures. The investigation found that, if the vessel certification process does not identify gaps in safety procedures and provide education, there is a risk that masters, owners, and others filling the role of AR will allow vessels to operate without effective safe work practices. Concentrated Inspection Campaigns (CICs) are one form of TC oversight that is independent of the regular certification program. In these campaigns, TC focuses on a specific area of safety concern for Canadian vessels. In 2021/2022, TC conducted a CIC that focused on fishing vessels and especially on compliance with the FVSR, including regulatory requirements for effective safety procedures. The CIC found deficiencies that had not been identified through TC’s certification program and issued deficiency notices to 62% of the 101 vessels inspected. The largest number of deficiencies were related to ensuring the safety of vessel and crew: vessels had deficiencies related to drills and drill records (41%), the completeness and accessibility of safety procedures (30%), and the crews’ knowledge of safety procedures (28%). TC’s oversight is not always effective and so the issue of regulatory oversight remains on the TSB Watchlist 2022. Without TC oversight to validate that the written procedures required by regulation on board fishing vessels have been developed and that crew are knowledgeable of their content, there is a risk that fishing operations will continue without guidance critical to support the safety of the crew and the vessel. The Board therefore recommends that the Department of Transport ensure that each inspection of a commercial fishing vessel verifies that each required written safety procedure is available to the crew and that the crew are knowledgeable of these procedures. |
|---|
INVESTIGATION REPORT M20C0188: Collision, General cargo vessels Florence Spirit and Alanis, Welland Canal, Ontario, 11 July 2020
| SAFETY ACTIONS | On 01 February 2021, the TSB sent Marine Safety Advisory Letter MSA 01/21 to McKeil Marine regarding the effectiveness of the Florence Spirit’s rudder angle in relation to the vessel’s speed. On 15 July 2021, TC conducted a flag state inspection and identified deficiencies related to McKeil Marine’s quality safety management system. The deficiencies included:
Additionally, TC identified 2 deficiencies to McKeil Marine for violating its own company policies. The vessel’s speed in the Welland Canal violated McKeil Marine’s under-keel clearance policy. There was no record of this breach, although it was required by company policy to be reported. As a result of the inspection, TC issued administrative monetary penalties to McKeil Marine. Following the occurrence, McKeil Marine reviewed the incident and produced an internal investigation report that was shared with all masters. It also took the following actions:
Following the occurrence, the Great Lakes Pilotage Authority (GLPA) reviewed the incident with a focus on compliance with the Pilotage Act and its regulations. On 08 September 2020, the GLPA implemented a process requiring restrictions to be placed on newly issued pilotage certificates when a candidate
As of 12 April 2021, the GLPA had issued 3 pilotage certificates with restrictions. The restrictions related to vessel size, vessel type, company of operation, geographic area (such as a port), and capacity limitations on the candidate’s certificate of competency. On 08 March 2022, the GLPA emphasized to companies with Great Lakes Marine Pilotage Certificate Training Programs that their programs need to clearly define the roles and responsibilities of all bridge team members. On 21 March 2022, the GLPA amended its policy concerning the use of electronic devices to emphasize prohibiting the use of electronic devices while employees are engaged in pilotage duties on the bridge of a vessel. Following the occurrence, the St. Lawrence Seaway Management Corporation conducted a review of speed management. The following actions were taken:
|
|---|
INVESTIGATION REPORT M20C0145: Striking of berth, bulk carrier CSL Tadoussac, Port of Québec, Québec, Quebec, 10 June 2020
| SAFETY ACTIONS | The Laurentian Pilotage Authority (LPA) conducted a case study of this occurrence and sent letters to the pilot and the master informing them of the study’s conclusions. Before this occurrence, the LPA had prepared a detailed policy on the exchange of information between masters and pilots, entitled Policy on Master-Pilot Exchange, which came into effect on 23 June 2020. Following this occurrence, this policy was sent to the pilot and the master at the same time as the study’s conclusions. |
|---|
INVESTIGATION REPORT M20P0229: Sinking with loss of life, Fishing vessel Arctic Fox II, 77 nautical miles west-southwest of Bamfield, British Columbia, 11 August 2020
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
INVESTIGATION REPORT M20P0353: Accidental release of free-fall lifeboat, Bulk carrier Blue Bosporus, English Bay, British Columbia, 01 December 2020
| SAFETY ACTIONS | Apollonia Lines S.A. took the following steps after the occurrence:
The circular reminded crews to ensure that
In addition, Apollonia Lines S.A.
|
|---|
INVESTIGATION REPORT M21A0315: Sinking and loss of life, Unregistered fishing vessel known as Island Lady, Labrador Sea, Newfoundland and Labrador, 17 September 2021
| SAFETY ACTIONS | The Board is not aware of any safety action taken following this occurrence. |
|---|
INVESTIGATION REPORT M21P0030: Sinking and loss of life, Tug Ingenika and barge Miller 204, Gardner Canal, British Columbia, 10 February 2021
| SAFETY ACTIONS | Following the occurrence, Wainwright Marine Services carried out a review of all crew certification and worked with all existing and new crew to ensure that their certification was not restricted to other organizations or vessels. In addition, Wainwright Marine Services hired an individual to provide training to crew members on decision making, stability, and girding. Finally, Wainwright Marine Services digitized its safety management system to facilitate updates and to ensure that company employees can access it at any time. In January 2022, TC established the Pacific Coast Tow and Workboat Safety Advisory Group, which includes representatives from industry, labour, and the government of British Columbia. The group’s purpose is to raise issues, develop initiatives, and put forward practical solutions and industry best practices. It also presents findings and makes recommendations to federal marine safety regulators and provincial occupational health and safety regulators regarding potential changes to regulatory, enforcement, and health and safety regimes. TC has also increased its outreach efforts to enrol tugs of 15 GT or less in the Small Vessel Compliance Program for Tugs. The authorized representatives for all of these tugs were contacted directly by TC. In the Pacific region, a targeted monitoring inspection campaign was initiated in January 2022 to verify compliance of tugs of 15 GT or less. At September 2022, more than 50 compliance inspections had been conducted. Finally, the scope of the existing memorandum of understanding between TC and WorkSafeBC is being expanded to include all commercial vessels in British Columbia, including tugs. Previously, the memorandum of understanding was limited to sharing information on operational or occupational health and safety concerns about fishing vessels. On 10 February 2021, the tug Ingenika, with 3 crew members on board, was towing the loaded barge Miller 204 in the Gardner Canal when the tug sank approximately 16 nautical miles west‑southwest of Kemano Bay, British Columbia (BC). The barge subsequently drifted and went aground about 2.5 nautical miles southwest from where the tug sank. The search and rescue operation located 1 surviving crew member on land and recovered the bodies of the 2 other crew members from the water. The barge was recovered; the tug was not found. At the time of the occurrence, the tug had 3500 L of diesel fuel in tanks on board. At September 2022, there were approximately 1343 tugs of 15 GT or less registered in Canada, approximately 1035 of which were registered in BC. Since 2015, the TSB has investigated 6 occurrences involving tugs of 15 GT or less operating on the west coast of Canada that have raised issues around the adequacy of regulatory surveillance. TC does not certify tugs of 15 GT or less, nor are these vessels required to undergo regular inspections. By comparison, before being certified by TC under the Vessel Safety Certificates Regulations, tugs of greater than 15 GT but of less than 150 GT are required to be inspected every 4 years, and tugs of 150 GT and greater are required to be inspected annually. Although TC has set an annual target of inspecting 3% of tugs of 15 GT or less nationwide, most will go years between inspections and may never be inspected over the life of the vessel. For example, the Ingenika was built in 1968 and had been in operation for over 50 years before this occurrence; the investigation found that there were no records of TC performing an inspection at any point in the tug’s operational life. The TSB also recently investigated another occurrence involving a tug of 15 GT or less, the Risco Warrior which was built in 1961 and had never been inspected. That investigation found that, in the absence of comprehensive regulatory surveillance and enforcement, there is a risk that tugs of 15 GT or less will continue to be operated with unsafe equipment and operating practices. While vessel owners and operators have the primary responsibility to manage safety, it is vital that TC provide effective oversight and proactively intervene to ensure that vessel owners and operators comply with regulations and standards and can manage the safety of their operations effectively. From April to October 2022, TC conducted 30 risk-based monitoring inspections of tugs of 15 GT or less. Overall, 21 of these inspections resulted in a total of 62 deficiencies, including 13 related to lifesaving equipment, 12 related to structure or stability, 8 related to crew certificates, 6 related to fire safety, and 5 related to navigation safety. From April to October 2022, TC also conducted 120 statutory inspections of tugs of greater than 15 GT. Sixty-four of these inspections resulted in the identification of deficiencies. Statutory inspections are generally more comprehensive than risk-based monitoring inspections. In addition, TC conducted 30 risk-based monitoring inspections of tugs of greater than 15 GT on the basis of findings from the statutory inspections. Of these 30 risk-based monitoring inspections, 19 resulted in the identification of deficiencies. In 2018–19, TC conducted a concentrated inspection campaign on domestic vessels. According to the campaign report, 83 vessels were inspected nationwide, 49 of which were inspected under the annual inspection category and 34 through quadrennial inspections per the Hull Inspection Regulations. Nineteen of the vessels inspected were tugs, but none were of 15 GT or less. The data showed that vessels inspected every 4 years had more deficiencies than those inspected annually. TC also focused on tugs in a concentrated inspection campaign conducted in BC from January to March 2017. Thirty tugs of 15 GT or less and 30 tugs of greater than 15 GT were selected for inspection. TC concluded that tugs of 15 GT or less had significantly more instances of regulatory non-compliance than tugs of greater than 15 GT For tugs of 15 GT or less, the onus is on the authorized representative (AR) to ensure compliance with the regulations and the safe operation of the vessel. However, in its Watchlist 2022, the TSB highlighted that many ARs of small vessels, such as the Ingenika, have limited awareness of key sections of the Canada Shipping Act, 2001 and of the broader regulatory framework. Other ARs may not be motivated to comply with regulations, given that it is well known that TC is unlikely to inspect their vessels and so the probability of enforcement is low. Recognizing the level of risk present, in 2016, the Board issued a safety concern on the issue of regulatory surveillance for tugs of 15 GT or less. On 25 June 2022, TC pre-published the proposed Marine Safety Management System Regulations, which will require tugs of 15 GT or less to develop a safety management system and obtain a Canadian safety management certificate. TC also developed and implemented the Small Vessel Compliance Program for Tugs (SVCP-T), which provides a simplified description of regulatory requirements and useful information that companies and ARs can use to evaluate their regulatory compliance. Although these are encouraging initiatives, neither are a replacement for vessel inspections under a broader program of regulatory surveillance, which would provide an opportunity to examine a vessel and its equipment to verify that it is in compliance with the regulatory requirements and being operated safely. Without adequate surveillance by TC, shortcomings in the safety management and operations of tugs of 15 GT or less will continue to go unaddressed, leading to accidents. Therefore, the Board recommends that the Department of Transport expand its surveillance program to include regular inspections of tugs of 15 gross tonnage (GT) or less to verify that these vessels are complying with regulatory requirements. The TSB has noted that, in addition to the need for regulatory surveillance for tugs of 15 GT or less, there is currently no requirement for towing companies operating these tugs to assess any of the risks that might be present in their operations, even when it comes to something as essential as assessing the suitability of their tugs for the towing operations they are undertaking. Although the present investigation focused on tugs of 15 GT or less, it was noted that there are also no requirements for risk assessments for tugs of greater than 15 GT. Although the Canada Shipping Act, 2001 requires the AR of any vessel to develop safe operating procedures and requires the master to ensure the safety of the vessel and anyone on board, what constitutes safe operating procedures is open to interpretation, and these requirements have not resulted in the effective management of risk on tugs of 15 GT or less. Combined with the fact that tugs in this category go largely uninspected and have no restrictions on their operations, there is the potential for accidents like the one involving the Ingenika to occur. Requirements for risk assessment do exist for some towing vessels; TC requires a risk assessment to be performed when a vessel is towing a vessel carrying oil or dangerous chemicals in bulk. These types of risk assessments provide an opportunity to look at each aspect of the towing operation, such as the weather, hazards posed by the cargo, and suitability of the tug for the tow. TC’s recently developed SVCP-T also provides useful data that can be used in risk assessments to support safe towing operations. Since the occurrence involving the Ingenika, TC has taken some initiatives to improve tug safety through the development of the SVCP-T and the pre-publication of the proposed Marine Safety Management System Regulations in the Canada Gazette, Part I. The proposed regulations, in particular, give TC an opportunity to develop regulatory provisions to ensure that companies operating tugs of 15 GT or less incorporate risk assessments into their operations. However, although the SVCP-T and the proposed regulations are positive steps forward, in their present forms, they do not explicitly require tug operators to conduct risk assessments. This means that risks in towing operations will continue to go undetected and unmitigated, placing crews, tugs, tows, and the environment in danger. Therefore, the Board recommends that the Department of Transport require authorized representatives of tugs of 15 gross tonnage (GT) or less to assess the risks present in their operations, including the suitability of their tugs for the specific towing operations they are undertaking. At the time of the occurrence, the Ingenika was operating in a compulsory pilotage area that falls under the responsibility of the Pacific Pilotage Authority (PPA). The PPA is a Crown corporation that has a mandate to establish, operate, maintain, and administer safe and efficient pilotage services in British Columbia. Pilotage services are provided by licensed pilots, who are highly trained navigators that use their knowledge of local waters to direct a vessel and navigate it using the safest route. The PPA has a pilotage waiver system under which some vessels, mainly tugs, may obtain waivers that exempt them from having to take a licensed pilot on board in designated pilotage areas if the operators and tugs meet certain requirements. However, when a company requests a pilotage waiver, the PPA does not check the information submitted to ensure that it meets regulatory requirements, and the PPA relies on operators to ensure that they are complying with waiver conditions once a waiver is granted. In BC, there are currently 364 tugs, owned by 85 different companies, that operate under pilotage waivers. This investigation identified that, although the master of the Ingenika had been issued a pilotage waiver, he held a certificate of competency that was restricted to passenger vessels operated by a specific company and therefore should not have been eligible for a waiver on a towing vessel. As well, one of the deckhands had, on various occasions, been put in charge of a navigational watch on board the Ingenika, but he did not hold a certificate of competency or a pilotage waiver. Further, the tug was not fitted with a bridge navigational watch alarm system and did not have a Class A automatic identification system, both of which are requirements for a vessel operating under a waiver. This investigation is not the first to identify shortcomings around the PPA’s process for issuing waivers and its reliance on companies to ensure ongoing compliance with waiver conditions. The TSB found similar issues in occurrences involving the tug Ocean Monarch in 2017and the tug Nathan E. Stewart in 2016. Without an effective process to verify that crew members and vessels meet PPA waiver requirements, there is a risk that non-compliance with waiver requirements will go undetected and compromise safety in compulsory pilotage waters. Given the need to ensure that waivered vessels are operating at a level of safety comparable to that afforded by a licensed pilot, the Board recommends that the Pacific Pilotage Authority verify that eligibility requirements are met before issuing pilotage waivers to companies operating tugs in compulsory pilotage areas. the Pacific Pilotage Authority implement a process to verify ongoing compliance with waiver conditions by companies operating tugs in compulsory pilotage areas. |
|---|
INVESTIGATION REPORT M22P0029: Grounding, Water taxi C12997BC (Rocky Pass), Coomes Bank, British Columbia, 25 January 2022
| SAFETY ACTIONS | On 26 April 2022, TC reached out to the Nuu-chah-nulth Tribal Council regarding occurrences in and near Tofino harbour in 2021 and early 2022. TC offered a follow-up discussion to share information about the current regulatory regime and better understand the Council’s perspectives about transportation safety in the Tofino area. |
|---|
Pipeline transportation sector
INVESTIGATION REPORT P21H0143: Third-party damage to a natural gas pipeline, Manitoba Hydro, Minell Pipelines Ltd. (a wholly owned subsidiary of Manitoba Hydro), Minell 6-inch natural gas pipeline, Near McAuley, Manitoba, 05 October 2021
| SAFETY ACTIONS | The TSB issued Pipeline Safety Advisory Letter 01/22, “External risks to pipelines in agricultural areas,” to Manitoba Hydro on 15 March 2022. The letter indicated that pipeline operators need to be aware of the depth of cover (DOC) over their pipelines to ensure that they are sufficiently buried or otherwise protected against normal agricultural activities that do not require explicit authorization. Given the risk of damage to underground pipelines by activities conducted on agricultural land, the letter indicated that Manitoba Hydro may wish to review the management practices associated with its damage prevention program to ensure that the Minell Pipeline is adequately protected. Manitoba Hydro took or initiated the following actions:
On 09 October 2021, the Canada Energy Regulator (CER) issued order MEL-001-2021 to Manitoba Hydro with respect to the occurrence. Among other things, the order required Manitoba Hydro to
On 13 April 2022, the CER issued Safety Advisory SA 2022-01, “Depth of Cover in Agricultural Areas,” to all regulated companies, and provided specific guidance on how to interpret the regulatory requirements for the prevention of pipeline damage, including preventive actions that companies can incorporate into their damage prevention programs. On 12 August 2022, following a compliance verification activity, the CER issued 4 notices of non-compliance to Manitoba Hydro. In October 2022, following a field inspection, the CER identified additional requirements for DOC survey spacing and requirements for right-of way patrol and monitoring, which are being addressed with Manitoba Hydro. |
|---|
Rail transportation sector
INVESTIGATION REPORT R19T0147: Employee fatality, Canadian National Railway Company, Remote control locomotive system, Dual hump yard assignment YDHF60, Mile 0.0, Halton Subdivision, MacMillan Yard, Vaughan, Ontario, 15 August 2019
| SAFETY ACTIONS | TC undertook an investigation under the Canada Labour Code, Part II (CLC II), and as a result, 2 directions were issued to the Canadian National Railway Company (CN): one on 15 August 2019, and another one on 11 October 2019. TC reviewed the corrective measures implemented by CN and deemed them to be satisfactory. The CLC II investigation has been completed and the results shared with the employer and its workplace health and safety committee as per CLC II requirements. On 15 August 2019, CN issued Notice No. 1908-15 which contained revised instructions for S-Yard industrial released cars. The notice identified that effective immediately and until otherwise notified:
On 21 August 2019, CN issued Notice No. 1908-21 which contained revised instructions for pulling W100 and S-Yard industrial released cars. The notice identified that the instructions were effective immediately and until otherwise notified. Due to the high-degree curvature at the north end of W100, CN eliminated the need to stop and restart movements to detrain at the W100 switch in order to eliminate in-train forces and the potential for derailment in these curves. The new procedure requires that
Once movement has commenced and has been ramped up to the 8 mph speed selector position (the maximum allowed speed to pull cars from W100 onto the west pullback), except in case of emergency, the throttle selector lever should only be placed to the “Coast” position to bring the movement to a stop.
The instructions previously communicated in Notice No. 1908-15 for the S-Yard industrial released cars remained in effect. CN has also implemented the following corrective measures:
|
|---|
INVESTIGATION REPORT R19T0191: Crossing accident, Metrolinx, GO Transit commuter train 3919, Mile 62.08, Guelph Subdivision, Kitchener, Ontario, 13 November 2019
| SAFETY ACTIONS | On 18 January 2021, the TSB issued Rail Safety Advisory 01/21, which discussed second-train events at multi-track grade crossings. This advisory cited the risks posed by multi-track crossings situated near rail yards where slow-moving trains and switching assignments frequently occupy the crossing and delay pedestrians or cyclists, sometimes in excess of the regulatory limit (5 minutes). The advisory indicated that, when delays involve a slow-moving switching assignment, crossing users may incorrectly assess the risks as being low, enter the crossing before the grade crossing warning devices deactivate, and proceed into the path of an oncoming second train. The advisory suggested that it may be prudent for the parties involved to identify those multi-track crossings that experience frequent and extended crossing signal activations and that have a high level of pedestrian and cyclist traffic, assess the likelihood of a second-train event to occur, and consider additional safety measures to minimize the risks of an accident. On 02 March 2021, TC responded to the TSB Rail Safety Advisory indicating that the accident occurred at a grade crossing that falls under provincial jurisdiction and that the Grade Crossings Regulations apply only to grade crossings under federal jurisdiction. Notwithstanding, TC indicated that CN and Metrolinx had begun performing joint audits of the Lancaster Street West crossing, and that they had been working collaboratively to identify possible improvements and action plans. In an effort to raise the safety concerns associated with conducting switching operations in the vicinity of crossings with double tracks, TC asked the Railway Association of Canada to share Rail Safety Advisory 01/21 with its members and recommend that they assess their crossings to determine if additional measures are needed to reduce the risk of a similar accident occurring in the future. Since the accident, Metrolinx has made a number of safety improvements at the crossing. Metrolinx has installed
In addition, it has
Metrolinx has also introduced a number of business processes to improve its crossing oversight:
Metrolinx continues to monitor CN switching activities via closed-circuit television cameras and in-person observations at locations where CN trains interact with GO Transit trains, which includes the Lancaster Street West crossing. Results from the observations and analyses of the crossings have identified non-compliances, which have been shared with CN management. As of February 2023, Metrolinx continues to work with CN to manage and reduce any safety risk to railway operations and the public. Since the accident, the Ministry of Transportation of Ontario (MTO) has begun to receive TC inspection reports, starting with the 2019 reports. Both the agreement with TC and the agreement with Metrolinx were updated in January 2022, and each contains amendments and additions to the original agreement, such as
In making these updates to the agreements, the MTO worked closely with TC to strengthen the MTO’s accountability role in the agreement, with respect to Metrolinx, to verify that non-compliances and deficiencies that may arise are appropriately addressed. The MTO has identified a need to update the oversight framework for urban and regional rail transit in Ontario that would better support the province’s growing rail network and the diversity of operators. Early in 2021, the MTO began a review of the safety oversight framework for provincial railways; this review was ongoing as of February 2023. The review encompasses provincial shortline railways, the Ontario Northland Transportation Commission, and urban and regional transit systems with rail service (i.e., the Toronto Transit Commission, GO Transit and UP Express [Metrolinx], OC Transpo, and ION light rail [Grand River Transit]). Since the accident, bitKIDS Behaviour Consulting moved from its Victoria Street North location to a new location that has its own fenced play area. Street-safety skills are taught in the fenced play area. Once children have learned the skills, they practise these skills daily outside the fenced play area. In addition, the bitKIDS Behaviour Consulting handbook has been updated to include the following statement: “Obey all traffic laws when crossing streets, railway tracks, and crosswalks with or without traffic signals at all times.” Safety concern: Regulatory oversight of Ontario provincial railways Metrolinx was created in 2006 to improve the coordination and integration of public transit train and bus service for the Greater Toronto and Hamilton Area.Footnote 9 It oversees the operations of UP Express, the dedicated air–rail link between Union Station in downtown Toronto and Lester B. Pearson International Airport, as well as of the GO Transit regional public transit train and bus service. The GO Transit train service and UP Express operate over about 420 km of rail lines, 337 km of which are owned by Metrolinx. In 2019, they carried an average of about 229 000 riders each weekday, which represents the highest daily ridership in Canada. In April 2020, the provincially regulated rail network in the Province of Ontario comprised 12 railways (including Metrolinx) that are governed by 3 provincial acts:
The MTO is responsible for the oversight of the provincially regulated railway system but it has no overall provincial regulatory framework and has not issued any regulations pursuant to the SRA. The MTO also does not have employees with the technical knowledge, experience, and expertise required to oversee the safety of railway operations; rather, it relies on various agreements with other parties in an effort to provide oversight. Specifically:
Metrolinx falls under the Metrolinx Act, 2006 when operating on its own provincially regulated track. Because this Act does not include safety-related provisions or subsequent offence provisions for violating them, it does not provide the Province of Ontario with a framework for taking enforcement action for safety-related deficiencies, when appropriate, against Metrolinx or other provincial railways operating on Metrolinx-owned property. Furthermore, TC inspectors do not have the authority to compel Metrolinx or other provincial railways operating on Metrolinx-owned property, to take action to address identified safety hazards. With regard to enforcement, it is within the authority of the Ontario Minister of Transportation to require Metrolinx or the Ontario Northland Transportation Commission to implement any directives issued to either agency with respect to any matter arising under their respective legislation, including implementation of corrective action. For the provincial shortline railways that fall under the authority of the SRA, the Registrar of Shortline Railways can suspend or revoke a railway licence. In accordance with its agreement with TC, the MTO was to receive all TC inspection reports and resolve any disputes from the implementation of the TC inspection agreement with Metrolinx. However, the MTO had not been receiving TC inspection reports and does not have employees with the technical knowledge, experience, and expertise required to evaluate TC inspection reports. Given the current complex MTO regulatory framework that involves multiple agreements, there are gaps in the oversight processes that can lead to occasions when the MTO will not be able to provide effective safety oversight. The MTO has identified a need to update the oversight framework for urban and regional rail transit in Ontario that would better support the province’s growing rail network and the diversity of operators. Early in 2021, the MTO began a review of the safety oversight framework for provincial railways; this review was ongoing as of February 2023. The review encompasses provincial shortline railways, the Ontario Northland Transportation Commission, and urban and regional transit systems with rail service (i.e., the Toronto Transit Commission, GO Transit and UP Express [Metrolinx], OC Transpo, and ION light rail [Grand River Transit]). The Board is encouraged that the MTO has identified a need to update the oversight framework for urban and regional rail transit in Ontario. However, although such a framework may include updated legislation and the creation of a regulator to provide oversight and support safety practices across the provincial railway sector, no such framework has yet been established. Therefore, the Board is concerned that the Province of Ontario does not provide effective safety oversight of provincially regulated railways. |
|---|
INVESTIGATION REPORT R19W0002: Main-track train collision and derailment, Canadian National Railway Company, Freight trains M31851-01 and M31541-03, Mile 50.37, Rivers Subdivision, Portage la Prairie, Manitoba, 03 January 2019
| SAFETY ACTIONS | On 04 April 2019, following this occurrence, Canadian National Railway Company (CN) distributed System Notice No. 904 to all operating employees in Canada. The notice warned train crews that there had once again been a marked increase in Canadian Rail Operating Rules Rule 439 violations across the CN system. In these cases, train crews failed to stop at signal indications requiring them to do so, primarily due to a lack of focus on situational awareness. It also noted that “operating crews must not be influenced by other information such as train lineups, detector broadcasts or other crew’s [sic] broadcasts until they themselves positively identify the next signal.” Safety action required Eastbound CN train M31851-01 (train 318) was proceeding on the south main track of the Rivers Subdivision. Train 318 was a key train operating on a key route, as defined by the TC–approved Rules Respecting Key Trains and Key Routes. At 0906:54, train 318 was travelling at 42 mph, with Trip Optimizer (TO) engaged and the throttle in position 7, as it passed a Clear to Stop signal indication at Mile 52.2. The conductor had called out the signal in the locomotive cab and identified the Clear to Stop indication but did not hear the locomotive engineer (LE) verbally respond to acknowledge the signal. At Mile 51.13, while travelling at 46 mph, train 318 passed the head end of train M31541-03 (train 315), which was westbound on the north track. The train 318 conductor then reminded the LE that they were operating under a Clear to Stop signal indication. Once reminded, the LE disengaged TO and made a full service brake application at 0908:34; 24 seconds later, he inadvertently placed the brake handle into the suppression position, and then applied the locomotive independent brake. At 0909:08, train 318 was proceeding at 39 mph at Mile 50.57 when the LE recognized that a collision was inevitable and placed the train in emergency. By 0909:30, train 318 had slowed to 23 mph when it side-collided with the 95th car of train 315 at Mile 50.37, as train 318 negotiated the equilateral turnout. The investigation concluded that:
Enhanced train control for key routes The rail transportation system is complex. The defence-in-depth philosophy advocated by safety specialists for complex systems seeks multiple and diverse lines of defence to mitigate the risks of normal human errors. Wherever possible, a combination of rules-based (i.e., administrative) defences and physical defences should be implemented to address normal slips, lapses, and mistakes that characterize human behaviour. Although newer circuitry has been integrated over the years, the basic design of centralized traffic control (CTC) signalling systems in Canada is well established. Despite this newer circuitry, railway operations still rely predominantly on administrative defences, which are the least effective method for mitigating risk. Administrative defences, such as the Canadian Rail Operating Rules, railway general operating instructions, and bulletins, place an over-reliance on a train crew to follow the rules and do not consider the human factors that affect behaviour in everyday life. For example, the CTC train control system in this case had the administrative requirement for train crews to follow the signal indications displayed in the field. Safe train operations are contingent on train crews observing each signal indication, broadcasting it, and then taking the appropriate actions. A signalled CTC system does not provide any advance warning to either the train crew or the rail traffic controller if a train crew does not observe a signal indication or does not take the appropriate action. CTC also does not provide automatic enforcement to comply with speed restrictions in order to slow or stop a train before it passes a restrictive signal. In instances where a train crew misperceives, misinterprets or does not follow a signal indication, the administrative defences as a whole fail. As demonstrated in this and other occurrences, when an administrative defence fails and there is no secondary defence, it can result in an accident that otherwise could have been prevented. In contrast to the administrative defences for train control systems available in Canada, Class 1 railways that operate in the United States (U.S.) have implemented physical fail-safe train control systems known as positive train control (PTC). PTC is designed to prevent train-to-train collisions, overspeed derailments, incursions into work zones, and movement of a train through a switch left in the wrong position. In Canada, the term “enhanced train control” (ETC) has been adopted to describe such systems. A PTC/ETC system would address the risk of crews misinterpreting or not following signal indications by automatically intervening to slow or stop a train in the event that an operating crew does not respond appropriately to a signal displayed in the field. A fully functioning PTC/ETC system would also offer a physical fail-safe defence against operating crew errors that are influenced by fatigue, which played a role in this accident. In the U.S., over the last 50 years, the National Transportation Safety Board (NTSB) has investigated more than 150 PTC-preventable accidents that took the lives of more than 300 people. From these investigations, the NTSB made 51 PTC-related recommendations. In September 2008, a collision between a Metrolink commuter train and a Union Pacific freight train in Chatsworth, California, prompted the passage of the Rail Safety Improvement Act of 2008 (RSIA) in the U.S. The RSIA mandated that PTC be installed on main rail lines that had specific risks associated with the transportation of dangerous goods (DG) as well as intercity and commuter passenger rail service. As of 31 December 2020, PTC was fully implemented in the U.S. on all track required by the RSIA legislation, a total of 57 535.7 miles, which accounts for about 41% of the nearly 140 000 route-miles of the U.S. rail network. The total miles of track that have PTC installed includes the U.S. operations of both CN (3107 miles) and Canadian Pacific Railway Company (CP) (2118 miles). For comparison, the Canadian rail network comprises about 26 000 route-miles of track. Key routes account for a combined total of about 10 940 miles of main track, which represents about 42% of the Canadian rail network. When the key route criteria are compared to the high-hazard route criteria of the U.S. RSIA, it is reasonable to conclude that the hazards and percentages for route-miles of affected track are similar. Although U.S. legislation required that PTC be installed on high-hazard routes, there is no similar requirement to install PTC or ETC on comparable routes in Canada that carry DG. A review of all TSB rail investigation reports (excluding Class 5 occurrences and including this occurrence) produced since the inception of the TSB in 1990 determined that 80 occurrences may have been prevented had a train control system equivalent to PTC (i.e., ETC) been available. Furthermore, when TSB Class 5 occurrences are also considered, from 2004 to 2019, there was an annual average of 31 reported occurrences in which a train crew did not respond appropriately to a signal indication displayed in the field, and the yearly number of these occurrences is on the rise. In particular, 2018 (40) and 2019 (38) had the highest number of these occurrences. In 2000, the TSB issued its first recommendation (R00-04) for implementing additional train control defences following its investigation into the 1998 collision between 2 CP trains near Notch Hill, British Columbia.Footnote 10 After determining that backup safety defences for signal indications were inadequate, the Board recommended that the Department of Transport and the railway industry implement additional backup safety defences to help ensure that signal indications are consistently recognized and followed. In 2013, the TSB issued another recommendation (R13-01) for implementing additional train control defences following its investigation into the 2012 derailment and collision of VIA Rail Canada Inc. passenger train 92 (VIA 92) near Burlington, Ontario.Footnote 11 Following the investigation, the TSB indicated that TC and the industry should move forward with a strategy that would prevent these types of accidents by ensuring that signals, operating speeds, and operating limits are always followed. The Board recommended that the Department of Transport require major Canadian passenger and freight railways implement physical fail-safe train controls, beginning with Canada’s high-speed rail corridors. In 2014, in response to the 2 TSB recommendations, a joint TC–industry train control working group (TCWG) was established. The group was chaired by TC Rail Safety, and also included representatives from the railway industry and operating crew unions. After establishing the TCWG, there were a series of ongoing meetings, discussions, and studies related to the development and implementation of ETC systems in Canada with no implementation plan or other tangible results to date. While TC did publish a Notice of Intent in the Canada Gazette, Part I, in February 2022 signalling its intent to require the implementation of ETC in Canada, there is still no implementation plan. In the time it took TC and industry to strike the TCWG, study the issue, produce the TCWG Final Report, contract a follow-on report from the Canadian Rail Research Laboratory (CaRRL) and study the CaRRL results, PTC had been fully implemented in the U.S. on all of the high-hazard trackage required by the RSIA legislation. Despite significant investment in PTC technology for the CN and CP locomotive fleets and their U.S. infrastructure, and 2 TSB recommendations to TC related to ETC dating back over 20 years, little has been done to extend the use of PTC into Canada or develop a similar form of ETC in Canada. In this occurrence, with no backup physical fail-safe defence, such as a PTC/ETC system, there was no automatic intervention available to slow or stop the train. Consequently, the collision occurred after the train 318 LE, who was fatigued, did not respond appropriately to the Clear to Stop signal displayed in the field. By definition, the CN Rivers Subdivision is a key route and is also an integral part of one of the major rail traffic corridors in Canada. This also means that the cities, towns, and villages along this key route are continually exposed to the risks associated with key trains transporting DG. Any collision or derailment involving a key train presents a risk of a DG release. If a train accident occurs on a key route, a key train or trains may be involved, increasing the risk of a DG release and potential adverse consequences to people, property or the environment. It is clear that the current administrative defences for train operation, such as company procedural guidelines, notices and instructions, as well as the TC–approved Canadian Rail Operating Rules and Work/Rest Rules for Railway Operating Employees, are not always effective. Consequently, incidents and accidents continue to occur. The first TSB recommendation on this issue is over 20 years old. The 2013 recommendation called for the implementation of physical fail-safe train controls, beginning with Canada’s high-speed rail corridors. (Canada’s primary high-speed rail corridor extends from Québec, Quebec, to Windsor, Ontario.) While the high-speed corridors are generally comprised of key routes, more recent accident history demonstrates that there is also a need for the implementation of fail-safe train control systems on all key routes. The implementation of physical fail-safe train control technologies such as ETC would provide an extra layer of safety when operated in conjunction with existing administrative defences. However, the Canadian railway industry continues to rely solely on administrative defences, such as company procedural guidelines, the Canadian Rail Operating Rules, and the Work/Rest Rules for Railway Operating Employees, to protect against train crews not responding appropriately to signal indications displayed in the field. If TC and the railway industry do not take action to implement physical fail-safe defences to reduce the consequences of inevitable human errors, the risk of collisions and derailments will persist, with a commensurate increase in risk on key routes in Canada. Therefore, the Board recommends that the Department of Transport require major Canadian railways to expedite the implementation of physical fail-safe train controls on Canada’s high-speed rail corridors and on all key routes. Crew resource management training Railway operations are governed by rules and instructions that place equal responsibility for safe train operations on all crew members. Safe railway operations are predicated on all crew members following all of the rules, all of the time. In the rail industry, operating rules require that crew members verbally acknowledge signal indications displayed in the field to each other. When a train encounters a signal indication displayed in the field, one crew member must communicate the signal indication aloud within the locomotive cab to the other crew member. While the other crew member is required to repeat the message back, there is no requirement for the original sender to confirm that the message was received accurately or understood by the other crew member. As a result, this communication can fail. The railway rules do not specify a closed-loop communication method, meaning there is no requirement for the original sender of the message to acknowledge, and therefore confirm, that it was received accurately. Moreover, when there is a significant difference in level of experience between operating crew members, an authority gradient may develop in which the less experienced crew member may not always intervene to ensure compliance with all of the rules. In these situations, there is a danger that safety-compromising behaviour will be overlooked because a less experienced employee may be reluctant to question the actions of a more senior employee or intervene in the operation of the train even when it may be critical to do so. In this occurrence, the investigation determined that communications between the 2 crew members were not always closed-loop. The callouts of signal indications by the conductor were not always acknowledged or repeated back by the LE. The conductor did not confirm that the LE had understood the communication nor was he required to do so. The inexperience of the conductor on the subdivision, and with locomotive operations, also deterred him from trying to intervene and stop the train. Crew resource management (CRM) is a concept introduced in the aviation and marine industries to limit or eliminate human errors by recognizing the importance of cognitive and interpersonal skills, thereby improving safety. CRM targets a crew’s skills, abilities, attitudes, communication, situational awareness, problem solving, and teamwork. Crew members must successfully interact with each other, their equipment, and their environment to effectively manage threats, errors, and unexpected conditions that may be encountered. In order to perform in a coordinated, efficient, and safe manner, crew actions need to be based on a common understanding of the current state of the equipment, the intended route to be taken, and any other potential threats. When this understanding is consistent, crews are better able to effectively anticipate and coordinate their actions to achieve their common goal. This common understanding between crew members is referred to as team or shared situational awareness. Shared situational awareness is developed and maintained by a crew through a number of discrete and continuous behaviours. These behaviours include in-trip briefings, the identification of key points throughout the trip, threat and error management (TEM), callouts to any change in the state of the equipment, the instrument setting or mode, and the communication of any change in plans to ensure that all crew members have a common understanding of activities. TEM stresses the principles of anticipation, recognition, and recovery when addressing threats, errors, and undesirable equipment states, and is based on the proactive detection of threats that could reduce safety margins. Effective error management is associated with specific behaviours by the crew, the most common being vigilance, a propensity to ask questions or provide feedback, and assertiveness. A 2015 study entitled Human Factors Analysis of “Missed Signals” in Railway Operations,Footnote 12 when addressing team training, indicated that CRM training
The report went on to state that CRM training includes aspects of team situational awareness such as “perception” and “information sharing, coordination and crosschecking information” and instructed crews to “become vigilant for losses of [situational awareness]; both one’s own and by others.” CRM focuses on providing crews with the interpersonal skills required to carry out their tasks safely: “CRM training typically consists of an ongoing training and monitoring process through which personnel are trained to approach their activities from a team perspective rather than from an individual perspective.”Footnote 14 Significant safety benefits were experienced in the aviation and marine industries with the introduction of CRM. Given the prevalence of human factors issues in rail accident statistics, this type of training could yield significant safety benefits in the rail industry.Footnote 15 Since 2017, CN has delivered a course called “Looking out for each other” as part of its operating crew requalification programs delivered every 3 years. While the CN training is insightful, it is broadly focused and does not specifically deal with train crew interaction within a locomotive cab or the authority gradients that may exist in that environment. While CP provides CRM training to its new operating employees, it does not provide formal dedicated recurrent CRM training. The Railway Employee Qualification Standards Regulations have no requirement for operating crews to complete a separate module on CRM when they qualify or re-qualify. Consequently, the adoption of CRM training in the rail industry has been sporadic and the approach differs between railways. Although railway training touches on CRM principles, neither CP nor CN provide dedicated, recurrent CRM training that explores all aspects of CRM. Recurrent CRM training would seek to improve non-technical skills that deal with in-cab communication, job briefings, backing-up behaviour, mutual performance monitoring, team leadership, decision making, task-related assertiveness (e.g., a junior operator speaking up to a dominant colleague), team adaptability, as well as concepts of TEM and team situational awareness. The TSB has investigated 8 other rail occurrences, dating back as far as 1996, in which ineffective CRM practices were identified as a factor that contributed to the accidents.Footnote 16 If operating crew members do not receive enhanced initial and recurrent CRM training to develop skills in crew communication, the coordination of decision making and activities, and dealing with authority gradients that may exist within a locomotive cab environment, there is an increased risk that inadequate crew communication will lead to unsafe operations. Therefore, the Board recommends that the Department of Transport require, under the Railway Employee Qualification Standards Regulations, Canadian railways to develop and implement modern initial and recurrent crew resource management training as part of qualification training for railway operating employees. |
|---|
INVESTIGATION REPORT R19W0050: Main-track train derailment, Canadian National Railway Company, Freight train U73451-11, Mile 197.47, Rivers Subdivision, St. Lazare, Manitoba, 16 February 2019
| SAFETY ACTIONS | Following this accident and 2 additional serious Canadian Pacific Railway Company crude oil unit train derailments near Guernsey, Saskatchewan, on 09 December 2019 (TSB Occurrence R19W0320) and 06 February 2020 (TSB Occurrence R20W0025), on 04 March 2020 the TSB issued rail safety advisories (RSA) 02/20 and 03/20 to TC. The RSAs noted that, since 2015, including this accident, the TSB had deployed to 7 train derailments involving tank cars that were transporting crude oil, 6 of which resulted in a significant release of product. A review of the 7 accidents revealed the following:
In RSA 02/20, the TSB indicated that train speed is one of the primary factors that contributes to the severity of a derailment. However, other factors such as train length, train weight, the position of the first car(s) derailed, the position of the cars in the train, and tank car design also play a role. The RSA suggested that, to reduce the frequency of these accidents and the commensurate risk to the public, property and the environment, TC should further review and modify key train speeds, as appropriate, based on various train risk profiles while also considering other factors that influence the severity of a derailment. In RSA 03/20, the TSB noted that, as train operations have evolved, the TSR have not kept pace. The current TSR came into force on 25 May 2012, almost 4 years before the TC-approved Rules Respecting Key Trains and Key Routes came into force in February 2016. While the TSR establish minimum standards for track infrastructure, there are no provisions in the TSR to address the need for enhanced track standards for key routes despite sometimes significant increases in dangerous goods traffic volumes on these routes. To reduce the frequency and mitigate the risks associated with accidents involving key trains on key routes, it is imperative that the track infrastructure be adequately maintained. Considering that the underlying causes of the 7 accidents identified were all related to failures of track infrastructure, TC was advised that the current TSR do not address the increased risks associated with the operation of key trains. The TSB suggested that TC consider revising the Rules Respecting Track Safety to include enhanced track standards for key routes. On 01 April 2020, TC issued Ministerial Order (MO) 20-05 which indicated that, pursuant to the provisions of section 32.01 of the Railway Safety Act, federally regulated railway companies were ordered to implement additional safety measures for key trains. The MO identified that there were a number of recent derailments of trains transporting dangerous goods that resulted in the breach of tank cars and the release of dangerous goods, including the St-Lazare derailment in Manitoba in 2019, the Guernsey derailment in Saskatchewan in 2019 and the second Guernsey derailment in Saskatchewan in 2020. Federally regulated railways were ordered to implement an additional definition for a higher-risk key train, which was defined as an engine with cars that include loaded tank cars carrying crude oil or liquefied petroleum gases, as defined in the Transportation of Dangerous Goods Act, 1992, in a continuous block of 20 or more tank cars, or 35 or more tank cars dispersed through a train. The MO also included additional speed restrictions, requirements for continuous welded rail (CWR) joint management, and requirements for installing replacement (plug) rail. MO 20-05 was effective immediately, with the exception of the requirements for CWR joint management and installing replacement (plug) rails, which were planned to come into effect on 01 September 2020. This MO will remain in effect until the Minister approves revised Rules Respecting Key Trains and Key Routes that incorporate the above measures on a permanent basis. On 01 April 2020, TC issued Ministerial Order MO 20-06 pursuant to the provisions of paragraph 19(1)(a) of the Railway Safety Act. The MO ordered federally regulated railway companies to revise the Rules Respecting Key Trains and Key Routes. The MO required that revised rules be based on an assessment of safety risk and, at a minimum, incorporate new definitions, including of “higher-risk key trains,” which is to be defined as “an engine with cars that include loaded tank cars carrying crude oil or liquefied petroleum gases, as defined in the Transportation of Dangerous Goods Act, 1992, in a continuous block of 20 or more tank cars, or 35 or more tank cars dispersed through a train;” additional speed restrictions; requirements for CWR joint management; and requirements for installing replacement (plug) rail. The MO required that railways file the revised Rules Respecting Key Trains and Key Routes with the Minister of Transport for approval within 210 days of the date that the MO was issued. On 06 November 2020, TC issued Ministerial Order MO 20-10 pursuant to the provisions of section 32.01 of the Railway Safety Act. With the issuance of MO 20-10, MO 20-05 was repealed, and federally regulated railway companies were ordered to implement additional safety measures for key trains including the following:
This order was effective immediately and will remain in effect until the Minister approves revised Rules Respecting Key Trains and Key Routes that incorporate the above measures on a permanent basis. On 22 February 2021, TC approved the revised Rules Respecting Key Trains and Key Routes submitted by the industry. The revised rules came into effect on 22 August 2021.Footnote 17 The revised rules are as follows:
On 01 April 2020, TC issued Ministerial Order MO 20-07, which indicated that, pursuant to the provisions of paragraph 19(1)(a) of the Railway Safety Act, federally regulated railway companies were ordered to revise the TSR. The revised TSR should be based on an assessment of safety risks, track-related derailment causes, evolving technology, current railway internal standards and industry best practices, and shall, at a minimum, address the following elements in 3 phases: Phase 1 elements
Phase 2 elements
Phase 3 - Structures / Other elements
The dates for filing the revised TSR with the Minister are 01 April 2021 (Phase 1), 02 October 2021 (Phase 2) and 02 April 2022 (Phase 3). On 31 May 2021, TC approved the Phase 1 revisions to the TSR. The revised TSR Part I, Section 9, items b) through f) include quality assurance requirements for safety-critical maintenance and repair activities.Footnote 18 These quality assurance requirements are expected to decrease the likelihood of derailments resulting from repair and maintenance activities that are inconsistent with the railway company’s standards and procedures. Part II, Subpart D, Section IX of the revised TSR includes requirements for CWR Management Plans that include comprehensive installation, inspection, and maintenance requirements.Footnote 19 The revised TSR also include requirements for railway companies to prepare and adhere to Track Geometry Management Plans, Rail Surface Management Plans, and Rail Wear Management Plans. CN provided the following information with regards to safety action taken: CN now requires the outside surface of all compromise joint bars, which is the side of a joint bar that is exposed when installed in track, to be spray-painted royal blue by the supplier. This change allows for compromise joint bars to be more easily differentiated from standard joint bars. The occurrence joint bars and rail were returned to CN for use in its training program for Engineering personnel. For training purposes, CN is also developing multiple rail track and joint bar kits made of lightweight composite material. Because rail track and joint bar kits could weigh up to 400 pounds, light weight kits are better suited for transport and practical, hands-on training. The following items were part of CN’s ongoing track maintenance initiatives for the Rivers Subdivision between 01 March 2019 and 31 December 2019:
|
|---|
INVESTIGATION REPORT R20H0130: Collision between train and track unit, Canadian National Railway Company, Freight train G87441-25 and Track unit, Mile 3.2, Caramat Subdivision, Jackfish, Ontario, 28 November 2020
| SAFETY ACTIONS | Following the occurrence, TC’s Regional Enforcement Unit conducted a regulatory investigation. The TC investigation determined that the Canadian National Railway Company (CN) employee’s actions were not in accordance with the Canadian Rail Operating Rules (CROR) Rule 803, which governs track unit and track work authorization. Subsequently, TC issued an Administrative Monetary Penalty to CN for the CROR Rule 803 contravention. Since the occurrence, CN has developed a software application (Electronic Track Authority Verification [ETAV]) for maintenance-of-way (MOW) employees that uses the track unit’s GPS location to provide audible alerts within the cab of the track unit as it approaches its limits of authority. The ETAV application obtains the limits of authority either by interacting with the electronic track occupancy permit program or by having the MOW employees manually input them. As of May 2022, CN has equipped 68% of a total of 1896 track units with the hardware necessary to support ETAV. The GPS locations that are used to delineate limits of authority have been mapped for ETAV use on 100% of CN’s main east-west corridor subdivisions, including the Caramat Subdivision, and on 44% of CN’s secondary corridor subdivisions. |
|---|
INVESTIGATION REPORT R20W0102: Main-track train derailment, Canadian Pacific Railway Company, Freight train 320-227, Mile 12.8, Ignace Subdivision, Near Ignace, Ontario, 25 May 2020
| SAFETY ACTIONS | Canadian Pacific Railway Company (CP) constructed a toe berm on the north side of the track to balance the existing former track embankment on the south side, and completed rehabilitation and stabilization work on the south side of the track after the derailment. The toe berm helps to evenly distribute loading of the subgrade and to counter differential settlement through the derailment area. CP conducted simulations and modified the distributed power configuration for grain trains of 224 cars. Such trains are now operated with a tail-end remote locomotive (distributed power train configuration 2-1-1) instead of a sense and braking unit (distributed power train configuration 2-1-0, the configuration of the occurrence train). Trains with 112 or 168 cars are still permitted to operate with a sense and braking unit instead of a tail-end remote locomotive. |
|---|
INVESTIGATION REPORT R21C0070: Fire on right-of-way, Canadian National Railway Company, Yard assignment YCYS61-16, Mile 124.95, Three Hills Subdivision, Calgary, Alberta, 17 July 2021
| SAFETY ACTIONS | In response to this occurrence and other recent occurrences involving fires on a railway right-of-way, TC approved the new Railway Extreme Heat and Fire Risk Mitigation Rules, which came into effect on 15 June 2022. The new rules stipulate requirements to address track integrity during periods of extreme heat, for inspection of the exhaust system, and for a fire risk mitigation plan for the prevention of fires on railway rights-of-way. |
|---|
INVESTIGATION REPORT R21H0087: VIA Rail Canada Inc., Passenger train No. 53, Mile 11.75, Smiths Falls Subdivision, Richmond, Ontario, 30 June 2021
| SAFETY ACTIONS | Following the occurrence, TC conducted a regulatory inspection of the crossing. The crossing met regulatory requirements with regard to visibility, sightlines, and crossing warning time. |
|---|
INVESTIGATION REPORT R21M0027: Main-track train derailment, Canadian National Railway Company, Train B73041-15, Mile 18.9, Napadogan Subdivision, Pangburn Station, New Brunswick, 21 August 2021
| SAFETY ACTIONS | Following the derailment, Canadian National Railway Company issued Operating Bulletin No. 618. This bulletin instructed train crews to avoid excessive braking and limit the dynamic brakes to position 5 or less from Mile 17.0 to Mile 21.2 of the Napadogan Subdivision. |
|---|