Collision with terrain
Privately registered
Cavalier SA102.5 (amateur-built aircraft), C-FBWF
Lacombe Aerodrome, Alberta, 14 NM E
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 09 October 2021, the privately registered, amateur-built Cavalier SA102.5 aircraft (registration C-FBWF, serial number 6958) was conducting a local recreational flight from Lacombe Aerodrome, Alberta, with 1 pilot and 1 passenger on board. When the aircraft was 14 nautical miles east of the aerodrome, it entered an aerodynamic stall, resulting in a left-hand spin and collision with terrain. The pilot, who was seated in the left seat, was fatally injured; the passenger received serious injuries. The aircraft was substantially damaged; there was no post-impact fire. The 406 MHz emergency locator transmitter activated. A satellite tracking device also helped locate the aircraft.
1.0 Factual information
1.1 History of the flight
At approximately 1516Footnote 1 on 09 October 2021, the privately registered, amateur-built Cavalier SA102.5 aircraft (registration C-FBWF, serial number 6958) departed Lacombe Aerodrome (CEG3), Alberta, for a local recreational flight with the owner/pilot and 1 passenger on board.
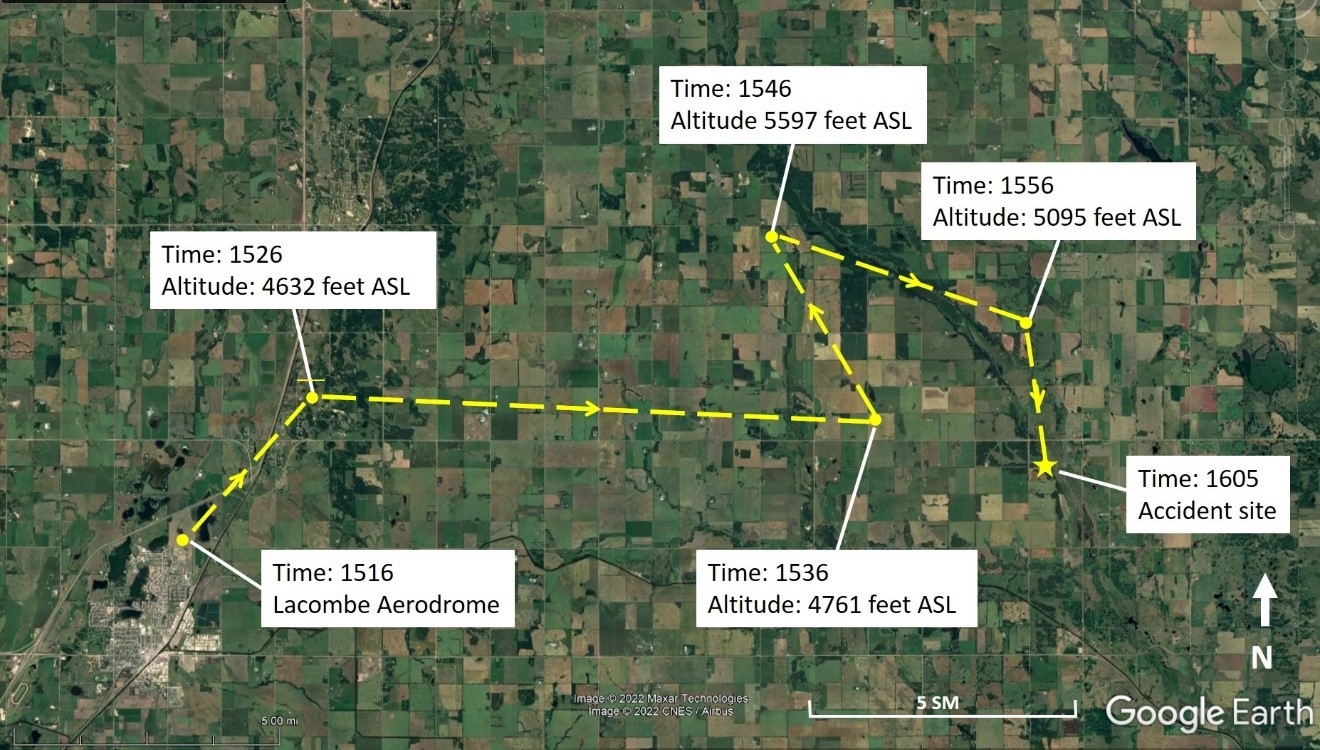
After departing CEG3, the aircraft flew generally eastward. Details of the flight path (Figure 1) were captured every 10 minutes by a SPOT satellite tracking deviceFootnote 2 on board. The last recorded position of the aircraft while it was airborne was at 1556, at an approximate altitude of 5095 feet above sea level (ASL). Following this, the aircraft changed direction to a south-southeast heading and at some point between this position and the accident site, the aircraft entered an aerodynamic stall, resulting in a spin and collision with terrain. The accident site was approximately 14 nautical miles east of Lacombe Aerodrome, Alberta, at an elevation of 2644 feet ASL.
At 1605, the 406 MHz emergency locator transmitter Footnote 3 (ELT) activated and a signal was detected by the Canadian Mission Control Centre, which relayed the information to the Joint Rescue Coordination Centre in Trenton, Ontario. The Joint Rescue Coordination Centre contacted first responders within 2 minutes.
First responders arrived at the site approximately 1 hour and 46 minutes after the accident. The pilot was fatally injured, and the passenger was seriously injured.
1.2 Injuries to persons
The pilot and 1 passenger were on board. Table 1 outlines the degree of injuries received.
| Degree of injury | Crew | Passengers | Persons not on board the aircraft | Total by injury |
|---|---|---|---|---|
| Fatal | 1 | 0 | - | 1 |
| Serious | 0 | 1 | - | 1 |
| Minor | 0 | 0 | - | 0 |
| Total injured | 1 | 1 | - | 2 |
1.3 Damage to aircraft
The aircraft was destroyed by the impact forces. There was no post-impact fire.
1.4 Other damage
There was no property damage in the area surrounding the accident site other than ground scars and some small fuel and oil spills.
1.5 Personnel information
The owner/pilot held an airline transport pilot licence – aeroplane, which had originally been issued on 18 December 1996, and was endorsed for single- and multi-engine landplanes. He held a Category 1 medical certificate that was valid until 01 February 2022. The pilot’s personal log recorded 18 472.3 total flight hours, of which 2382.7 hours were on single-engine aircraft.
A review of the aircraft’s journey log revealed that the pilot had flown 90.2 hours in the Cavalier SA102.5 in the time he had owned the aircraft (since July 2017). The pilot’s personal log showed that he had performed basic aerobatic manoeuvres, including spins, during solo flights in the occurrence aircraft.
At the time of the occurrence, the pilot was employed by an airline as a captain and training captain.
| Pilot licence | Airline transport pilot licence (ATPL) |
|---|---|
| Medical expiry date | 01 February 2022 |
| Total flying hours | 18 472.3 |
| Flight hours on type (air time from journey log) | 90.2 |
| Flight hours in the 7 days before the occurrence | 11.6 |
| Flight hours in the 30 days before the occurrence | 47.7 |
| Flight hours in the 90 days before the occurrence | 98.5 |
| Flight hours on type in the 90 days before the occurrence | 12.6 |
1.6 Aircraft information
The occurrence Cavalier SA102.5 was an amateur-built aircraft that had been constructed in 1969, primarily of wood and fabric (Figure 2). It was fitted with a non-certified Aero Sport Power Ltd. O-320-B2B piston engine, a Sensenich 74DM6-0-64 fixed-pitch propeller, and fixed, tricycle landing gear. The airframe had a total of 913.2 hours. The aircraft was equipped with dual flight controls. It was not equipped with a stall warning device or an angle-of-attack indicator system, nor was it required to be by regulation.

| Manufacturer | Amateur-built |
|---|---|
| Type, model and registration | Cavalier, SA102.5, C-FBWF |
| Year of manufacture | 1969 |
| Serial number | 6958 |
| Certificate of airworthiness/flight permit issue date | 25 May 2005 - Special Certificate of Airworthiness - Amateur-built |
| Total airframe time | 913.2 hours |
| Engine type (number of engines) | Aero Sport Power Ltd. O-320-B2B (1) |
| Propeller type (number of propellers) | Sensenich 74DM6-0-64 (1) |
| Maximum allowable take-off weight | 793.8 kg |
| Recommended fuel type(s) | Avgas 100LL |
| Fuel type used | Avgas 100LL |
The aircraft was inspected annually as required by the Canadian Aviation Regulations (CARs). The most recent annual inspection was dated 23 June 2021. There were no records of any outstanding defects. The Cavalier is a stable aircraft design with no significant adverse flight characteristics and typical stall and spin behaviour. The pilot operating handbook has no information related to spins.
1.6.1 Spin characteristics of the Cavalier SA102.5
The occurrence pilot had spun the aircraft and successfully recovered on several occasions. His personal log included a number of entries on solo flights with notes about aerobatic manoeuvres that had been conducted, including spins. Owners of this aircraft model have said that the stall and spin characteristics are docile and that the aircraft can be recovered from this flight profile using basic techniques. In an article published in the December 2017 issue of the Experimental Aircraft Association’s Bits and Pieces Newsletter, the designer of the airplane is said to have had no problems recovering the aircraft from a spin, including when the aircraft is inverted.Footnote 4
On board the aircraft during the occurrence flight were the pilot and 1 passenger, very little baggage, and a maximum of 23 U.S. gallons of fuel at takeoff. The aircraft’s gross weight on the occurrence flight was calculated to be within the maximum allowable take-off weight. The centre of gravity (C of G) could not be calculated because the investigation did not have access to the necessary documentation. However, it is unlikely that the aircraft was loaded in a such a way that would have negatively affected the C of G and made the recovery from a spin difficult.
1.7 Meteorological information
The hourly aerodrome routine meteorological report issued at 1600 for Red Deer Regional Airport (CYQF), Alberta, the closest airport to the accident site, indicated the following:
- Winds variable at 2 knots
- Visibility 9 statute miles
- Sky clear
- Temperature 15 °C, dew point −6 °C
- Altimeter 29.73 inches of mercury
- Density altitude 4000 feet
Weather was not considered a factor in this occurrence.
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
Not applicable.
1.11 Flight recorders
The aircraft was not equipped with a flight data recorder or a cockpit voice recorder, nor was either required by regulation. The aircraft was, however, equipped with a SPOT satellite tracking device, which captured flight path data.
1.12 Wreckage and impact information
The aircraft struck the ground in a shallow, nose-down, nearly wings-level attitude. Ground scars and the position of the wreckage indicate that the aircraft was rotating to the left, but had very little forward movement. This is consistent with the aircraft being in a left-hand spin at the time of impact.
During impact, the main landing gear collapsed directly under the wings and the nose gear collapsed under the engine cowl. The tail of the aircraft partially broke just aft of the cabin (Figure 3). The fuel tanks, located at the wing tips, ruptured and spilled their contents.

The wings had partially sheared from the fuselage, but cables and rods controlling the ailerons and flaps were still attached to the cabin. The primary flight controls were examined, and flight control continuity was confirmed.
The engine mixture control was found in the full rich/forward position, the throttle control was found at mid travel, the fuel tank selector was on the left fuel tank, and the fuel boost pump switch was in the OFF position. During the investigation, the engine was placed on a test stand and run up to full throttle with no issues noted.
1.13 Medical and pathological information
1.13.1 Cause of death
The Office of the Chief Medical Examiner in Alberta reported that the cause of death was attributed to blunt force trauma with cardiovascular disease as a significant contributing factor. The report also noted that the pilot had evidence of a heart attack, although it was not possible to determine the exact time of this event.
1.13.2 Transport Canada aviation medical certification
The primary activity of Transport Canada’s (TC’s) Civil Aviation Medicine Branch is performing medical assessments required for the certification of licensed aviation personnel. As stated in CARs Standard 424.04(1)(b),
[…] Medical Certificates are issued by the Minister of Transport through the office of the Regional Director, Aviation Licensing following receipt of:
(i) a medical examination report, provided the candidate meets the pertinent medical standards and has been assessed medically fit or fit subject to any restriction or limitation recommended by Civil Aviation Medicine Division [sic] Medical Staff; […]Footnote 5
The pilot held a Category 1 medical certificate that was valid until 01 February 2022. However, because the occurrence flight was a recreational flight, the pilot was only required to hold a Category 3 medical certificate. The pilot’s medical certificate did not document any known medical conditions, nor were there any restrictions on his licence.
1.13.2.1 Medical examination
The purpose of the medical examination is to determine whether an applicant meets the standards for the issuance of a medical certificate, which is needed to validate a pilot’s licence. TC is mainly concerned with managing the risks to aviation, such as incapacitation, for the period of the licence. If necessary, further medical examination may be requested.
In accordance with CARs Standard 424.04(2)(a), “[e]very applicant for a medical certificate or revalidation thereof shall undergo a medical examination by a CAME [Civil Aviation Medical Examiner].”Footnote 6 CARs Standard 424.17 requires that the CAME examine the pilot carefully and that the examination be “sufficiently thorough so as to determine whether the applicant meets the requirements in respect of the category of medical certificate that is applied for or in respect of which a validation is sought.”Footnote 7
TC’s Handbook for Civil Aviation Medical ExaminersFootnote 8 provides guidance to CAMEs on how to perform medical examinations and assess medical fitness. During a medical examination, CAMEs are required to complete Medical Examination Report 26-0010, which must then be sent to the appropriate regional office for review by the regional aviation medical officer.Footnote 9
Holders of a commercial pilot licence, a multi-crew pilot licence – aeroplane, or an airline transport pilot licence require a valid Category 1 medical certificate. The medical certificate is valid for 12 months unless the holder of the licence is 40 years of age or older and is conducting single-pilot operations with passengers on board, or is 60 years of age or older. In those cases, the medical certificate’s validity period is reduced to 6 months.Footnote 10
The occurrence pilot, who was older than 40, regularly attended a TC medical examination every 12 months as required for his airline transport pilot licence. For each visit, a medical examination report was completed as required. However, for his most recent medical certificate, issued in 2021, the pilot did not undergo a medical examination. Instead, he completed and signed an attestation that he did not have any limitations or restrictions or other conditions that could impair his ability to exercise the privileges of the licence. This attestation was allowed in accordance with an exemption issued by TCFootnote 11 due to the global COVID-19 pandemic.
1.13.2.2 Management of cardiac-related illness in commercial aviation in Canada
The Handbook for Civil Aviation Medical Examiners advises CAMEs that the risk of a fatal accident occurring as a result of medical incapacitation of a pilot is dependent on a number of factors, such as the amount and type of flying or the presence of other qualified pilots, all of which must be taken into consideration in addition to the known risks of a particular medical condition.Footnote 12 For a Category 1 medical certificate, the pilot is required to “not suffer from any disease or disability which may render the applicant liable to become unable to operate an aircraft safely.”Footnote 13
Heart disease places an applicant in a potentially high-risk category for an incapacitating event. CARs Standard 424 stipulates that “[t]he applicant shall not possess any abnormality of the heart, congenital or acquired, which is likely to interfere with the safe operation of an aircraft.”Footnote 14
Heart disease is any condition that affects the structure or function of the heart. There are 4 main types of heart disease:
- Heart rhythm disorders (arrhythmias)
- Structural abnormalities
- Heart failure
- Coronary heart diseaseFootnote 15,Footnote 16
In accordance with the Handbook for Civil Aviation Medical Examiners, it is essential for the CAME to identify and document the presence of any heart disease or associated diseases during a civil aviation medical exam.
1.13.2.3 Identifying heart disease during the aviation medical examination
When examined by a CAME, some applicants may present with obvious symptoms and/or documentation indicating past or present heart disease. However, others may not present with any single obvious indicator or have any history of cardiac illness. For example:
[m]any [individuals] may have ischemic episodes without knowing it. […] People with angina also may have undiagnosed episodes of such silent ischemia. In addition, people who have had previous heart attacks or those with diabetes, are especially at risk for developing silent ischemia.Footnote 17
Ischemic heart disease is a term given to heart problems caused by narrowed heart arteries. This may also be called atherosclerosis, which involves the arteries becoming narrowed as a result of fatty deposits.Footnote 18
It is difficult for CAMEs to suspect heart disease or estimate an applicant’s risk of a cardiac-related incapacitation event when the applicant presents with no confirmed and documented heart disease. Guidance for assessing the risk factors associated with heart disease to help CAMEs ascertain the risk profile of each applicant is available in the CARs Standards,Footnote 19 Figure 2 in the Handbook for Civil Aviation Medical Examiners,Footnote 20 and the Handbook for Civil Aviation Medical Examiners’ link to the cardiovascular fitness assessment guide.Footnote 21 This guidance material reflects recommendations made during a TC Civil Aviation Medicine Branch aviation cardiology workshop in 2010 and replaces the former TC cardiovascular guidance from 2002.
The Handbook for Civil Aviation Medical Examiners outlines the various risk factors for heart disease, which include age, gender, obesity, blood pressure, smoking, family history of heart disease, results from cardiac tests, and symptoms of heart disease, such as chest pain and shortness of breath. CAMEs are also provided with information on the Framingham risk scoring tool. This tool takes into account information on 6 key risk factors: age, blood lipids, blood pressure, history of diabetes, smoking status, and possibly family medical history. Once this information is collected, the CAME will assign scores to each risk factor to estimate the overall risk profile of the individual, i.e. their risk of having a cardiac-related incapacitating event.
To assess an applicant’s risk factors, CAMEs are provided with guidance on 4 techniques:
- Medical interview: during the interview, the CAME requests information on the applicant’s cardiac-related health and any other associated health issues, such as diabetes. The CAME relies on the applicant declaring cardiac-related information, such as chest pain, any known results of medical exams or treatments, and health behaviours, such as smoking and alcohol consumption.
- Physical exam: during the physical exam, the CAME examines the applicant’s peripheral circulation and heart function, takes the applicant’s blood pressure, and uses height and weight to calculate the applicant’s body mass index (BMI).
- Review of electrocardiograms: the CAME assesses the applicant’s most recent electrocardiogram, which, for a pilot over the age of 40, must be conducted within the 12 months preceding the medical exam. Footnote 22
- Examination of other test results: CAMEs may, at their discretion, request further medical screening if they believe there are indications of a disease that must be further examined to establish medical fitness.
In this occurrence, the pilot had a medical interview, medical examination, and an electrocardiogram for each annual visit, during which medical data on cardiac risk factors were documented. The CAME did not identify or document any significant cardiac risk factors.
The CAME did not calculate the pilot’s BMI for most of the pilot’s examinations because this information was not required on the CAME’s examination form. Only newer versions of the examination form require the BMI to be calculated. When calculated by the TSB from the available information on the examination forms, the pilot’s BMI had been at or above the obese threshold Footnote 23 since at least 2014. The pilot therefore had some risk factors such as age, gender, and obesity. However, the independent cardiology review performed for this investigation confirmed that none of the pilot’s results would have raised a suspicion of increased cardiovascular risk.
1.13.2.4 Assessing laboratory data as a risk factor
An independent cardiology review performed for another TSB investigation Footnote 24 highlighted that, based on the consensus of a multinational consortium of aviation cardiologists published in 2019, Footnote 25 cardiovascular risk screening should be required for all pilots over the age of 40, and for those pilots identified to be at an increased risk (based on risk calculation). Such screening should always include an assessment of blood lipids.
The occurrence pilot did not have any laboratory data assessed as part of his civil aviation medical examinations. However, the investigation determined that he did have blood tests performed in 2019 at the request of his family physician. These tests included blood lipids. The independent cardiology review performed for this investigation confirmed that even if the CAME had had access to these results, the pilot’s blood lipids would not have raised a suspicion of increased cardiovascular risk.
The pilot’s family physician requested further routine blood testing in July 2021, but the pilot did not fulfill this request. However, the independent cardiology review confirmed that unless there were significant changes in lifestyle, dietary patterns, or weight, blood lipids tend to remain fairly stable over time. Therefore, even if the blood testing had been done in 2021, the results may still not have indicated an increased cardiovascular risk.
The independent cardiology review performed for this investigation highlighted that, although most cardiovascular disease is indicative via blood lipids, some 10–20% of heart attack victims do not present with these traditional risk factors. Therefore, cardiologists advise that other mechanisms may also be required to screen for coronary atherosclerosis. For example, elevated lipoprotein Lp(a) has been identified as a significant additional hereditary risk factor in some individuals. Lipoprotein Lp(a) measurement has been incorporated into the recommended periodic screening for cardiovascular risk. Footnote 26
Current TC CAME guidelines, which were published in 2012, only recommend—they do not mandate—enhanced screening using laboratory data, such as screening for blood lipids. Given that it is not policy to screen using laboratory data, CAMEs are not required to use such screening for periodic certification examinations, even for those applicants over the age of 40.
The cardiology reviews conducted by the same cardiologist for both this occurrence and for TSB Air Transportation Safety Investigation A19P0142 indicate that the TC Civil Aviation Medicine Cardiovascular Guidelines from 2012 have not been updated to include the significant advances in the recommended approach to screening for coronary atherosclerosis. The cardiology review for this occurrence also stated that options for screening could include blood lipids and potentially enhanced laboratory testing for Lp(a), as well as CT (computed tomography) cardiac imaging where possible.
In this occurrence, the cardiologist concluded that if such screening methods were followed, risk factors contributing to the pilot’s heart attack may have been identified.
1.13.2.5 Calculating an applicant’s risk profile
The Handbook for Civil Aviation Medical Examiners stipulates that an estimated risk, calculated using any of the recommended risk estimators (e.g. the Framingham risk scoring tool), of 2% per yearFootnote 27 for a sudden incapacitating cardiovascular event should be the threshold for performing enhanced screening before medical certification:
The cumulative risk conferred by the presence of more than one risk factor, even at levels only moderately above normal, can exceed that conferred by the presence of one major risk factor alone. […] If abnormalities are found, resulting in an average annual mortality risk of 1% or more, assuming an additional 1% risk of an incapacitating nonfatal event, then a license holder is considered medically unfit for an unrestricted licence.Footnote 28
The Handbook also specifies that
[c]oncern about these [major modifiable] risk factors is greater in applicants with known ischemic heart disease where the absolute risk is greater.Footnote 29
This investigation reviewed the information TC provides to CAMEs for medical examinations and determined that the guidance does not mandate the use of the Framingham risk scoring tool and in no way is the tool linked with the use of the TC medical examination report. In addition, nothing on the medical examination report specifically prompts the CAME to use the Framingham risk scoring tool or to consolidate key risk factors to determine the applicant’s overall risk profile.
There was no cardiovascular risk profiling performed as part of any of the pilot’s medical examinations. However, using data from the CAME medical examinations, the blood lipids from the family physician’s records, and various risk-profiling methods, including the Framingham risk scoring tool, the independent cardiology review confirmed that the pilot’s calculated annual risk for a cardiovascular event was approximately 1% per year. This is considered a low-to-average risk for his age, and acceptable for commercial pilot operations. Even if the CAME had performed risk profiling, these results would not have triggered secondary screening testing for underlying coronary disease.
1.13.3 Oversight of cardiovascular factors
The oversight and management of medical risk factors involving cardiovascular and hypertensive issues in pilots have been addressed in previous TSB reports. As of October 2022, there were 32 900 pilots in Canada with Category 1 medical certificates. Of these, 16 607 (approximately 50%) were over the age of 40. Since 2000, there have been 8 accidents, including this one, involving commercial pilots in which cardiovascular disease was identified as a finding as to risk Footnote 30 or finding as to cause. Footnote 31
1.13.4 Reportable health issues
The Aeronautics Act states,
[w]here a physician […] believes on reasonable grounds that a patient is a flight crew member […] or other holder of a Canadian aviation document that imposes standards of medical […] fitness, the physician […] shall, if in his opinion the patient has a medical […] condition that is likely to constitute a hazard to aviation safety, inform a medical adviser designated by the Minister forthwith of that opinion and the reasons therefor. Footnote 32
As part of provincial licensing, physicians are informed about their provincial and federal mandatory reporting responsibilities. Physicians can access this information through the web-based Canadian Medical Association’s document CMA Driver’s Guide: Determining medical fitness to operate motor vehicles, Footnote 33 which contains a section on Aviation. This section includes details of the Aeronautics Act’s reporting requirements, as well as an alert that states:
Physicians are required by law to report to regional aviation medical officers of Transport Canada any pilots, air traffic controllers or flight engineers with a medical condition that could affect flight safety. Common conditions requiring mandatory reporting are listed in this section. Footnote 34
It should be noted that the Aeronautics Act’s requirement to report issues that are a hazard to flight safety applies specifically to physicians and optometrists; it does not apply to psychologists, social workers, or counsellors.
The Guide also states:
When pilots are informed that they have a condition (or are prescribed treatment) that might make it unsafe for them to perform their duties, they must “ground” themselves temporarily.
A physician diagnosing a condition that might affect flight safety must report the condition to the medical advisors of Transport Canada. Footnote 35
The Aviation section provides guidance on medical conditions, a link to the Handbook for Civil Aviation Medical Examiners and guidance on prescription medications. More specifically, the Guide states:
Medications with side effects of postural hypotension, arrhythmias or effects on the central nervous system are unacceptable. Footnote 36
It further states:
Prescription drugs: Discuss in detail the side effects of any medication that is prescribed or recommended to pilots. For example, minor side effects on visual accommodation, muscular coordination, the gastrointestinal tract or tolerance to acceleration (increased gravity) may be more serious when they occur in flight. If in doubt, the physician should discuss the medication with the RAMO [Regional Aviation Medical Officer]. Footnote 37
Physicians are informed that if they suspect that a condition might affect flight safety, they should inform the pilot and contact the RAMO at a Civil Aviation Medicine regional office. The section provides contact details for the Civil Aviation Medicine headquarters, as well as the Civil Aviation Medicine regional offices. Once a physician contacts the RAMO, they can either informally discuss a medical condition or medication, or formally complete a Civil Aviation Medicine Medical Condition Reporting Form.
It could not be determined how often family physicians are informed of their provincial and federal reporting responsibilities, or how often they access or read the CMA Driver’s Guide: Determining medical fitness to operate motor vehicles.
The Handbook for Civil Aviation Medical Examiners and CARs Standard 424 also require the applicant for a medical certificate to provide complete and accurate information regarding their health. Although these requirements refer to disclosure during the medical examination, by signing the declaration, applicants are also committing to disclosure for the duration of the medical certification period.
The occurrence pilot’s family physician’s notes did not contain any medical information to indicate there had been any cardiovascular-related discussion or identified risk factors.
However, from September 2019 to July 2021, the pilot had visited the family physician on 5 different occasions with an acute medical condition unrelated to cardiovascular health. In May 2021, the pilot was prescribed 3 medications to treat this condition, but reportedly none were taken. The pilot was not scheduled for work in May. One of these medications, as confirmed by the cardiology review for this occurrence, has significant central nervous system side effects, including drowsiness and dizziness, and should not be used within several days of flying or performing safety-sensitive duties. In overdose, it can cause cardiac arrhythmias (irregularities of heart rhythm).
Another one of the medications can predispose a person to cardiovascular thrombotic events (clots), but does not directly increase the risk for a coronary event (heart attack). This medication is generally used only for the temporary relief of significant symptoms. The cardiology review confirmed that pilots with symptoms that require this medication should be grounded because such symptoms would be incompatible with the safe operation of an aircraft.
One of these medications also contained a warning on the label not to take it if the patient has congestive heart failure, high blood pressure, and heart issues.
It should be noted that, although these medications were prescribed in the months preceding the occurrence, they were not listed in the toxicology results of the autopsy.
The occurrence pilot’s family physician was aware of his profession; there was a note on his file that he was a commercial airline pilot. However, the investigation determined that the physician was not aware of any aviation-related reporting responsibilities.
There was no indication in either the TC medical records or the family physician’s medical records that the family physician or the pilot had informed TC of the acute condition or of the medications prescribed.
In 2011, following the TSB investigation into a loss of control and collision with terrain that took place in Miramichi, New Brunswick, on 23 April 2010, Footnote 38 the Board issued the following Safety Concern:
The Board is concerned that medical practitioners may not always be aware of the need or importance of transmitting reportable medical conditions and, further, that deficiencies exist in the guidelines designed to screen for cardiovascular risks. As a consequence, there continues to be a risk that cardiovascular risk factors will go undetected in aviation personnel.
1.14 Fire
There was no post-impact fire.
1.15 Survival aspects
1.15.1 Emergency locator transmitter
As a result of a TSB recommendationFootnote 39 issued in 2016, the CARs were amended to require the installation of 406 MHz ELTs, replacing the older 121.5 MHz standard. The new regulations have an implementation date of 25 November 2025.
Although an upgrade was not yet required by the CARs, the owner of the occurrence aircraft replaced the 121.5 MHz ELT with a 406 MHz ELT in August 2021. The 406 MHz ELT helped first responders find the accident site quickly and provide emergency medical services.
Not all 406 MHz ELTs are manufactured the same. Some ELTs, such as the one installed in the occurrence aircraft, can only send a radio signal, with no location data, to the satellite. Others can input information from a GPS on the aircraft into the ELT. Still others have an internal GPS and do not require any outside data input to provide detailed location information when the ELT is activated.
ELTs that transmit on frequency 121.5 MHz not only have an expected search area of 1260 km2, but the frequency is no longer monitored by Cospas-Sarsat. ELTs that transmit on frequency 406 MHz with no location data have an expected search area of 13 km2. ELTs that transmit on frequency 406 MHz and either have a built-in GPS or receive data from an external GPS, can provide a precise location of the crash site.Footnote 40
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP142/2021 – NVM Data Recovery – AvMap
- LP153/2021 – Instruments Analysis
1.17 Organizational and management information
Not applicable.
1.18 Additional information
1.18.1 Aerodynamic stall and incipient spin
A stall is a loss of lift and an increase in drag that occurs when an aircraft is flying at an angle of attack greater than the angle that provides maximum lift. Regardless of airspeed, an aircraft always stalls when its wings reach this critical angle of attack.Footnote 41 Stall speed varies depending on factors such as the aircraft’s weight, power setting, flap position, and angle of bank.
An incipient spin occurs when an aircraft stalls and one wing produces more lift than the other. Because the descending wing is at a greater angle of attack, it stalls even further and produces more drag, which triggers an autorotation. During this phase of the incipient spin, the flight path changes from horizontal to vertical.Footnote 42
Generally, even if the pilot takes the necessary measures to stop the rotation as soon as it begins, the aircraft is in a vertical position while accelerating rapidly, and sufficient altitude is necessary to regain a horizontal flight path. If the rotation continues, the aircraft could stabilize in a spin and follow a helical path downward (Figure 4).
![Illustration of an incipient spin (Source: TSB, based on Transport Canada, TP 1102, Flight Training Manual, 4th Edition [revised 2004], Figure 2-31)](/sites/default/files/eng/rapports-reports/aviation/2021/a21w0089/images/a21w0089-figure-04.jpg)
2.0 Analysis
The investigation did not identify any issues related to the airframe and engine that could have contributed to the aerodynamic stall and subsequent spin. The analysis will discuss possible scenarios for an aerodynamic stall and spin. Next, it will examine the approach taken by Transport Canada (TC) for managing cardiovascular health and hypertension in pilots. Finally, the analysis will discuss the emergency response to the occurrence.
2.1 Departure from controlled flight and spin
The accident site was consistent with the aircraft being in a spin at impact. Given that there was no wreckage trail, the aircraft had low forward velocity and was in a nearly horizontal attitude at impact.
The investigation did not have data available to determine a detailed flight path because the aircraft was not equipped with devices capable of recording flight data. However, 10-minute plots from a SPOT satellite tracking device were available, which gave basic track information such as time, average speed, and altitude. Without detailed flight path information, the investigation was unable to determine the precise circumstance in which the aircraft collided with terrain.
The investigation determined that the aircraft was within its weight limitations; however, there was not enough documentation to determine the balance of the aircraft. It is likely that the aircraft was within the balance envelope given that the aircraft has 2 seats, the moment arm for the fuel is on a similar moment arm as the seats, and there was little baggage on board. The weight and balance condition likely did not cause the aircraft to enter a stall and spin and would not have prevented a recovery from the spin.
It could not be determined whether the entry into the stall was intentional or unintentional. The pilot had previously conducted solo stall and spin manoeuvres on numerous occasions, and he likely would have recognized the signs of an unintentional impending stall. The aircraft was equipped with dual flight controls; however, the investigation could not determine whether the passenger attempted to fly the aircraft at any time during the flight.
Finding as to causes and contributing factors
For undetermined reasons, the aircraft entered an aerodynamic stall and spin, and remained in the spin until it collided with the ground.
2.2 Cardiovascular health
Autopsy results indicated that cardiovascular disease with narrowing of the coronary arteries was a significant contributing factor to the pilot’s death. The autopsy also identified that the pilot had experienced a heart attack, although the timing was not specified. The independent cardiologist confirmed that the significant coronary disease and evidence of a heart attack provide a very plausible, even if remote, scenario for an in-flight acute medical incapacitation—for example, due to a cardiac arrhythmia. However, it is not possible to ascertain if this event was causal to the occurrence, or as a result of the occurrence.
Finding as to causes and contributing factors
Cardiovascular disease was a contributing factor to the pilot’s death; however, it could not be determined whether this resulted in an in-flight incapacitation, or in his death before or after the collision with terrain.
The pilot’s civil aviation and family physician medical records were reviewed by the investigation and by an independent cardiologist to ascertain the risk of this pilot having an incapacitating event. No obvious risk factors were noted that would have placed the pilot at an increased risk of cardiovascular disease or an associated incapacitating event. Therefore, neither the Civil Aviation Medical Examiner (CAME) nor the family physician had any reason to conduct any further cardiac screening.
However, it was noted by the investigation and confirmed by the independent cardiologist that because 10–20% of heart attack victims do not present with any traditional risk factors, including abnormal blood lipids, cardiologists advise that other mechanisms may also be required to screen for coronary atherosclerosis, such as more advanced blood screening and heart CT (computed tomography) scans where possible. Two cardiology reviews—one for this investigation and one for another TSB investigation—indicated that the TC Civil Aviation Medicine Cardiovascular Guidelines from 2012 have not been updated to include the significant advances in the recommended approach to screening for coronary atherosclerosis. The cardiologist concluded that, in this occurrence, if such screening methods were followed, risk factors contributing to the pilot’s heart attack may have been identified.
Finding as to risk
If TC guidance material and the civil aviation medical examination report do not include up-to-date cardiovascular screening methods to perform a global cardiovascular assessment when appropriate, there is an increased risk that cardiovascular disease will remain unidentified and pilots may become incapacitated while operating an aircraft.
The investigation revealed that the pilot had been prescribed medications that could have affected his cardiovascular health and, therefore, flight safety; however, the pilot reportedly did not take any of these medications. Even though the medications were not taken, the pilot’s family physician was not aware of the requirement to provide such information to TC.
Findings as to risk
If CAMEs are not informed by physicians and pilots about medical conditions and/or medications that could affect the safe operation of an aircraft, then there is an increased risk that pilots will be certified without appropriate safety mitigations in place.
If physicians are not regularly informed and updated on their federal responsibilities to report medical conditions and/or medications that may affect flight safety, TC may not have the information required to accurately determine a pilot’s fitness for flight.
2.3 Emergency response
The occurrence aircraft was equipped with an emergency locator transmitter (ELT) capable of transmitting on frequency 406 MHz. The ELT activated following impact and the signal was received by the Canadian Mission Control Centre. Within 2 minutes, the Joint Rescue Coordination Centre in Trenton, Ontario, had contacted first responders to initiate the search.
In addition, a SPOT satellite tracking device was on board the aircraft. This device also helped search and rescue personnel find the aircraft quickly.
Finding: Other
The aircraft was equipped with a 406 MHz ELT and a SPOT satellite tracking device, which contributed to a timely response by first responders. As a result, the passenger received first aid treatment quickly, which contributed to his survival.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- For undetermined reasons, the aircraft entered an aerodynamic stall and spin, and remained in the spin until it collided with the ground.
- Cardiovascular disease was a contributing factor to the pilot’s death; however, it could not be determined whether this resulted in an in-flight incapacitation, or in his death before or after the collision with terrain.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If Transport Canada guidance material and the civil aviation medical examination report do not include up-to-date cardiovascular screening methods to perform a global cardiovascular assessment when appropriate, there is an increased risk that cardiovascular disease will remain unidentified and pilots may become incapacitated while operating an aircraft.
- If Civil Aviation Medical Examiners are not informed by physicians and pilots about medical conditions and/or medications that could affect the safe operation of an aircraft, then there is an increased risk that pilots will be certified without appropriate safety mitigations in place.
- If physicians are not regularly informed and updated on their federal responsibilities to report medical conditions and/or medications that may affect flight safety, Transport Canada may not have the information required to accurately determine a pilot’s fitness for flight.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- The aircraft was equipped with a 406 MHz emergency locator transmitter and a SPOT satellite tracking device, which contributed to a timely response by first responders. As a result, the passenger received first aid treatment quickly, which contributed to his survival.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transportation Safety Board of Canada
On 11 January 2023, the Transportation Safety Board of Canada issued Air Transportation Safety Advisory Letter A21W0089-D2-A1 to Transport Canada (TC). The letter informs TC that not all physicians are aware of the requirement to report medical issues for their patients that hold a pilot licence. It also encourages TC to work with the Canadian Medical Association to develop communication strategies to increase the awareness of the reporting requirements for physicians under the Aeronautics Act.
On 19 January 2023, TC responded to the TSB’s Safety Advisory Letter A21W0089-D2-A1. It its response, TC stated that Transport Canada Civil Aviation Medicine had coordinated with the Canadian Medical Association to increase awareness of the reporting requirements for physicians.
4.2 Safety action required
4.2.1 Screening tools for pilot medical exams
On 09 October 2021, the privately registered, amateur-built Cavalier SA102.5 aircraft (registration C-FBWF, serial number 6958) was conducting a local recreational flight from Lacombe Aerodrome, Alberta, with 1 pilot and 1 passenger on board. When the aircraft was 14 nautical miles east of the aerodrome, it entered an aerodynamic stall, resulting in a left-hand spin and collision with terrain. The pilot, who was seated in the left seat, was fatally injured; the passenger received serious injuries. The aircraft was substantially damaged; there was no post-impact fire.
The Office of the Chief Medical Examiner in Alberta reported that the cause of death was attributed to blunt force trauma with cardiovascular disease as a significant contributing factor. The report also noted that the pilot had evidence of a heart attack, although it was not possible to determine the exact time of this event.
The pilot’s Category 1 medical certificate, which was valid until 01 February 2022, did not list any limitations.
The occurrence pilot, who was older than 40, regularly attended a TC medical examination every 12 months as required for his airline transport pilot licence. For each visit, a medical examination report was completed as required. However, for his most recent medical certificate, issued in 2021, the pilot did not undergo a medical examination. Instead, he completed and signed an attestation that he did not have any limitations or restrictions or other conditions that could impair his ability to exercise the privileges of the licence. This attestation was allowed in accordance with an exemption issued by TC Footnote 43 due to the global COVID-19 pandemic.
There was no cardiovascular risk profiling performed as part of any of the pilot’s medical examinations. However, using data from the Civil Aviation Medical Examiner (CAME) medical examinations, the blood lipids from the family physician’s records, and various risk-profiling methods, including the Framingham risk scoring tool, an independent cardiology review performed for this investigation confirmed that the pilot’s calculated annual risk for a cardiovascular event was approximately 1% per year. This is considered a low-to-average risk for his age, and acceptable for commercial pilot operations. Even if the CAME had performed risk profiling, these results would not have triggered secondary screening testing for underlying coronary disease.
The independent cardiology review highlighted that, although most cardiovascular disease is indicative via blood lipids, some 10–20% of heart attack victims do not present with these traditional risk factors. Therefore, cardiologists advise that other mechanisms may also be required to screen for coronary atherosclerosis. For example, elevated lipoprotein Lp(a) has been identified as a significant additional hereditary risk factor in some individuals. Lipoprotein Lp(a) measurement has been incorporated into the recommended periodic screening for cardiovascular risk. Footnote 44
An independent cardiology review performed for another TSB investigation Footnote 45 highlighted that, based on the consensus of a multinational consortium of aviation cardiologists published in 2019, Footnote 46 cardiovascular risk screening should be required for all pilots over the age of 40, and for those pilots identified to be at an increased risk (based on risk calculation). Such screening should always include an assessment of blood lipids and, in some cases, other methods might be needed for the 10–20% of heart attack victims that do not present with traditional risk factors.
Current TC CAME guidelines, which were published in 2012, only recommend—they do not mandate—enhanced screening using laboratory data, such as screening for blood lipids. Given that it is not policy to screen using laboratory data, CAMEs are not required to use such screening for periodic certification examinations, even for those applicants over the age of 40.
The cardiology reviews conducted for both this occurrence and for TSB Air Transportation Safety Investigation A19P0142 indicate that the TC Civil Aviation Medicine Cardiovascular Guidelines from 2012 have not been updated to include the significant advances in the recommended approach to screening for coronary atherosclerosis. The cardiology review for this occurrence also stated that options for screening could include blood lipids and potentially enhanced laboratory testing for Lp(a), as well as CT (computed tomography) cardiac imaging where possible.
In this occurrence, the cardiologist concluded that if such screening methods were followed, risk factors contributing to the pilot’s heart attack may have been identified.
In 2011, following the TSB investigation into a loss of control and collision with terrain that took place in Miramichi, New Brunswick, on 23 April 2010, Footnote 47 the Board issued the following Safety Concern:
The Board is concerned that medical practitioners may not always be aware of the need or importance of transmitting reportable medical conditions and, further, that deficiencies exist in the guidelines designed to screen for cardiovascular risks. As a consequence, there continues to be a risk that cardiovascular risk factors will go undetected in aviation personnel.
In 2012, the TC Civil Aviation Medicine Cardiovascular Guidelines were updated.
As of October 2022, there were 32 900 pilots in Canada with Category 1 medical certificates. Of these, 16 607 (approximately 50%) were over the age of 40. Since 2000, there have been 8 accidents, including this one, involving commercial pilots in which cardiovascular disease was identified as a finding as to risk Footnote 48 or finding as to cause. Footnote 49
If TC guidance material and the civil aviation medical examination report do not include up-to-date cardiovascular screening methods to perform a global cardiovascular assessment when appropriate, there is an increased risk that cardiovascular disease will remain unidentified and pilots may become incapacitated while operating an aircraft. Therefore, the Board recommends that
the Department of Transport establish a framework for routine review and improvement to the Handbook for Civil Aviation Medical Examiners to ensure it contains the most effective screening tools for assessing medical conditions such as cardiovascular health issues.
TSB Recommendation A23-01
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .