Loss of Control - Collision with Water
Elbow River Helicopters Limited
Bell 212 (Helicopter), C-GTKE
Lillooet, British Columbia 20 nm S
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Elbow River Helicopters Limited Bell 212 helicopter (registration C-GTKE, serial number 30704) was engaged in firefighting operations about 20 nautical miles south of Lillooet, British Columbia. At approximately 1602 Pacific daylight time, the accident helicopter approached the Fraser River to pick up water. Shortly before reaching the pickup location, the helicopter descended unexpectedly and its water bucket, on a 150-foot longline, touched down in a fast flowing section of the river. As the helicopter continued forward, it was dragging the water bucket. Moments later, the helicopter pitched nose-down, yawed to the left, struck the river surface, broke up, and sank. The pilot escaped the wreckage and was swimming in the fast flowing water. Repeated attempts to rescue the pilot by other helicopters in the area proved unsuccessful. The pilot's body was found downstream five days later. Some pieces of the wreckage, including the longline and water bucket, were retrieved, but the majority of the wreckage was not recovered.
Other Factual Information
Aircraft
The Bell 212 is a twin-engine, single main-rotor helicopter that can carry up to 14 passengers with 1 pilot. It has hydraulically boosted controls and a characteristic of the anti-torque control pedals is that there is little or no resistance to the pilot's input. With both feet on the pedals, resistance is introduced by the pilot's opposing leg. Records indicate that the helicopter was certified, equipped, and maintained in accordance with existing regulations and approved procedures, and that the weight and centre of gravity were within prescribed limits.
The helicopter was configured to be flown by one pilot from the left front seat. This configuration allowed the pilot to look down the left side of the helicopter to monitor the external load.
The helicopter was also configured to carry external loads on a hook attached to a lift beam at the bottom of the main transmission. This hook is commonly referred to as the belly hook and it was rated for a maximum load of 5000 pounds. Attached to the belly hook via a 150-foot longline was a 300-gallon water bucket. The bucket was electrically opened by a button near the pilot's left hand on the collective. The belly hook could either be electrically released by a button on the cyclic control stick or manually by a pedal located between the anti-torque control pedals. The electrical release on the cyclic control stick is the primary release. The manual release was designed as a backup emergency release. To activate the manual release, the pilot would have to take one foot off the anti-torque control pedals and use it to push the release pedal. To enable the electrical release, the pilot must select the hook release switch (arm switch) to the armed position. With the hook disarmed, the pilot is unable to electrically release the load using the button on the cyclic control stick.
The Bell 212 Flight Manual Supplement (BHT-212-FMS-3) for the belly hook directs pilots to arm the hook for take-off, disarm it for in-flight operations (i.e., cruise), and arm it before final approach. Disarming the hook during cruise reduces the risk of an inadvertent release. Arming the hook during take-off and on final allows the pilot to quickly release the load should a problem arise during a critical phase of flight. Some operators prefer that company pilots operate with the belly hook disarmed; this is because of a history of dropped loads. Sometimes the dropped loads were due to electrical malfunctions, but most times happened as a result of pilots accidently triggering the electrical release. The accident pilot was known to have flown with the belly hook disarmed.
Pilot Information
The pilot held a Commercial Helicopter Pilot's Licence validated by a flight medical on 20 March 2009. He had approximately 10 000 flight hours total time on helicopters, of which about 1200 hours were on the Bell 212 type. He had accumulated approximately 3300 hours carrying-out forest fire water bucketing. A review of his records indicated that he was trained and certificated appropriately for the flight.
A post-mortem examination revealed that the pilot was not likely injured during the crash, but had drowned. The pilot was wearing a helmet. He was a good swimmer but was not wearing a personal flotation device (PFD).
There was no regulatory requirement to have flotation devices for the helicopter or its occupants, as long as the helicopter was within reach of shore with one engine inoperative.Footnote 1
Weather
Recorded weather on the day of the accident shows no precipitation in the area. The wind direction at Lillooet, approximately 20 nautical miles (nm) north of the accident site, changed from north to south between 1600 and 1700.Footnote 2 At Lytton (12 nm south) the wind was from the south all day and reached 32 knots around the time of the accident.
Operations
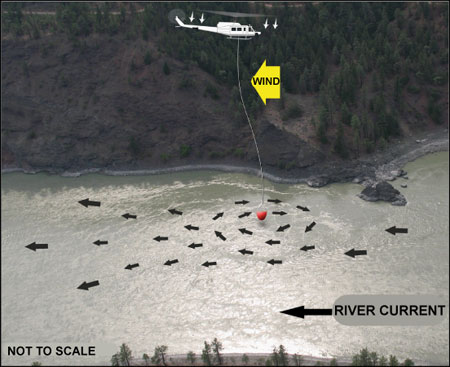
At the time of the occurrence, four helicopters were engaged in forest fire water bucketing operations approximately 20 nm south of Lillooet. They were using the Fraser River to fill their water buckets. At the accident location, the Fraser River is in a canyon and was flowing south at about 9 knots. The pilots had chosen a spot in the river where there was a whirlpool. The backside of the whirlpool is characterized by back-flowing current in the opposite direction to the river current. The pilots were dipping their buckets in this back-flowing water, which prevented the current from dragging them downstream (see Figure 1).
The helicopters were less than one minute apart in a circuit from the river to the fire and back to the river. On the approach to pick up water, the accident helicopter made a tight right-hand circuit before its final approach. The helicopter ahead was still picking up water. On the water pickup just prior to the accident pilot's approach, the winds were from the north. During the rescue attempts immediately following the accident, the winds were from the south. The canyon had little vegetation and provided little indication of the wind direction. The pilot attempting the rescue had not noticed the change in the wind until he was trying to rescue the accident pilot and his helicopter weather-cocked to the south.
Canyon Effect
Mountainous regions are characterized by rapidly changing and unpredictable winds. Winds will usually conform to the topography, following the contours of a canyon wall. As wind velocity increases in areas of steep, rough, broken topography, turbulent airflow can occur and winds may flip from one direction to the opposite direction in a canyon.Footnote 3
Vortex Ring State
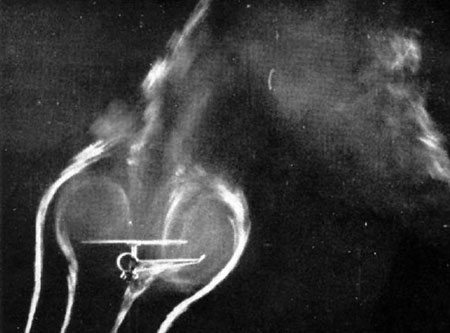
Helicopters are susceptible to an aerodynamic phenomenon known as the vortex ring state (VRS). VRS occurs when a helicopter's flight path, airspeed, and rate of descent coincide with the helicopter's downwash.Footnote 4 The risk of VRS increases when a helicopter slows in a downwind condition. In normal flight, airflow from the main rotors is directed downward. In VRS, the tip vortices generated by the main rotors re-circulate through the rotor, adversely affecting lift (see Photo 1). A helicopter in VRS quickly begins losing altitude, despite having power available to sustain flight. A helicopter in VRS may also experience vibrations, excessive flapping, and a reduction in cyclic authority. Applying more power (increasing collective pitch) serves to further accelerate the downwash through the main-rotor, exacerbating the condition.
The Transport Canada (TC) Helicopter Flight Training Manual highlightsFootnote 6 that VRS is likely to occur when the following three conditions are present:
- Powered flight;
- High rate of descent, in excess of 500 feet per minute; and
- Low airspeed, less than 20 miles per hour indicated.
To reduce the risk of entering VRS, helicopter pilots are trained to avoid entering their helicopter's own downwash. Should pilots of single main-rotor helicopters find themselves in VRS, there are two widely recognized recovery methods. They are as follows:
- Dive Out - Apply forward cyclic while reducing the collective in an attempt to gain airspeed. As airspeed increases, the helicopter will move out of its downwash and normal flight can be resumed.
- Enter Autorotation - This results in changing the airflow from disturbed airflow due to VRS to upward autorotational airflow. The pilot may then ease the cyclic forward, gain airspeed, and increase power to resume normal flight.
Regardless of the recovery technique, a helicopter in VRS will lose considerable altitude before it is able to resume normal flight. If insufficient altitude is available, the helicopter may impact the ground before it is able to recover from VRS.
Rescue Efforts
The accident pilot successfully egressed the wreckage. He was wearing his helmet and trying to swim. One of the other helicopter pilots put his water bucket close to the accident pilot in the water, but he disappeared below the water's surface. The wreckage floated for a very short time and drifted north in the back eddy before it sank. The water's depth in the back eddy was about 50 feet.
Analysis
The helicopter was not recovered; however, it is believed that mechanical malfunctions were not a factor in this accident. Therefore, the analysis focuses on the canyon winds, helicopter aerodynamics, operational factors, and post-crash survival.
Because of the local topography, the wind direction changed 180° in a short time. This may have happened without a decrease in wind speed and, because of the barren land and rough water, the wind direction would have been hard to identify.
The tight circuit just before final approach—likely for spacing—put the helicopter in a position that would have necessitated a steep approach, requiring careful power management. It is likely that the accident pilot's approach was unknowingly conducted with a tailwind, due to the sudden change in wind direction. This would have caused the helicopter to lose translational lift early on the approach, likely producing a sudden increase in the rate of descent. To counter this descent, the pilot would have to add power. The combination of a steep approach, unknowingly conducted downwind at slow speed with power applied, likely caused the helicopter to descend into its own downwash. This would have caused the helicopter to enter VRS and produced a rapid descent. The VRS condition and/or the attempt to recover by gaining airspeed or lowering the collective caused the water bucket to drop into the river before reaching the back eddy (See Figure 2, position A).

In an attempt to recover from VRS, the pilot would have pushed the cyclic forward to gain airspeed. However, the water bucket would have been full and drifting downstream, opposite to the direction of flight. This would have produced an anchor-like effect on the helicopter, causing it to pitch nose-down (see Figure 2, position B). The pilot would have quickly run out of aft cyclic travel while trying to raise the nose, causing a loss of control and the helicopter to fly in a descending arc until it collided with the water.
If the pilot had released the longline before he ran out of aft cyclic travel, he would likely have been able to fly away without losing control.
It is impossible to ascertain whether or not the pilot attempted to release the water bucket before the crash. Because he was known to disarm the release switch, the pilot would not have been able to electrically release the water bucket. The left yaw that occurred just prior to impact could be attributed to a last second attempt to jettison the longline and water bucket. In doing so, the pilot probably took his right foot off the right anti-torque control pedal to activate the manual belly hook release. This would make it very easy to induce a left pedal input that caused the helicopter to yaw left.
Findings as to Causes and Contributing Factors
Findings as to causes and contributing factors
- The combination of a steep approach, unknowingly conducted downwind at slow speed with power applied, likely caused the helicopter to enter a vortex ring state (VRS).
- During the pilot's attempt to recover, the water bucket dropped into the flowing river and acted as an anchor, causing the helicopter to pitch nose-down and collide with the water.
- The helicopter was likely being operated with the belly hook electrically disarmed, limiting the pilot's ability to jettison the water bucket before losing control.
- Although the pilot was able to escape the helicopter wreckage in the water without injury, he was not wearing a personal flotation device (PFD) and drowned.
- The helicopter's manual emergency release for an external load requires the pilot to remove one foot from the anti-torque control pedals. As a result, there is an increased risk of loss of anti-torque control at a critical time of flight.
- Operations in deep canyons may be subject to turbulent airflow and winds that rapidly flip from one direction to the opposite. Without adequate warning, helicopter pilots may be placed at risk.
Safety Action Taken
Elbow River Helicopters Limited
Immediately following the accident, the helicopter operator instituted policies requiring pilots to fly with the belly hook armed and to wear personal flotation devices (PFDs) when water bucketing.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .