Controlled Flight into Terrain
Canadian Helicopters Limited
Sikorsky S-76A (Helicopter), C-GIMR
Temagami, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Sikorsky S-76A medivac helicopter (registration C-GIMR, serial number 760079), operated by Canadian Helicopters Limited, departed Sudbury for Temagami, Ontario, to meet a land ambulance. At approximately 2202 eastern standard time, while on final approach to the Temagami Snake Lake Helipad in night visual meteorological conditions, the helicopter crashed in the forested area at the edge of the lake. The helicopter came to rest on its left side and was substantially damaged. Three of the four occupants received serious injuries and were transported to hospital.
Factual information
The closest reporting weather station was in North Bay, Ontario, approximately 50 nautical miles (nm) south of Temagami. The 2200Footnote 1 Aviation Routine Weather Report (METAR) for North Bay was as follows: wind 140° True (T) at 3 knots, visibility 12 statute miles (sm), light snow, scattered layer of cloud at 1600 feet above ground level (agl), broken layer at 3000 feet agl, temperature 6°C, dew point −7°C, altimeter 29.85 inches of mercury. The entire region was experiencing localized light to moderate snowfall on the evening of the occurrence and it was uncertain as to whether the flight would be able to land in Temagami.
The crew consisted of the captain, the first officer, and two paramedics.
The captain was the pilot flying (PF) and held a valid airline transport pilot license-helicopter. The captain was certified and qualified for the flight in accordance with existing regulations. He had approximately 3107 hours total flying time and 2267 hours on the Sikorsky S-76A. Records indicate that he had received all of the company required training, including night visual flight rules (VFR)/instrument flight rules (IFR) and controlled flight into terrain with specific training for black hole approaches (visual spatial disorientation). The captain had been to this location once in the past, on a day VFR flight.
The first officer was the pilot not flying (PNF) and held a valid commercial pilot license-helicopter. He had approximately 1967 hours total flying time and 147 hours on the Sikorsky S-76A. He was certified and qualified for the flight in accordance with existing regulations. The first officer was hired in July 2007 and had all the required training. He was fairly new to emergency medical services (EMS) operations and had never been to this location.
On the night of the occurrence, the helicopter departed Sudbury at approximately 2140 on a short flight to the Snake Lake Helipad in the town of Temagami located approximately 60 nm to the northeast. The helicopter climbed to 2500 feet and proceeded to Temagami. Throughout the initial portion of the flight, the visibility was found to be no less than four to five sm and improved as the flight progressed. The flight was uneventful and both pilots spent most of the time discussing procedures and coordinating the patient pick-up with dispatch. During the last 1.5 minutes of the approach, the PF was explaining to the PNF what he was doing, step by step, and what to watch out for during night approaches, including black hole illusions.
The Snake Lake Helipad is located on the northeast edge of town. According to the Canadian Helicopters Landing Site Directory for the Sudbury/Moosonee district, the Snake Lake Helipad is at a field elevation of 997 feet above sea level (asl) and has a 100 by 100-foot asphalt-surfaced pad with retro-reflective cones around the perimeter and with lead-in cones at 220° magnetic (M) from the pad. Four of the perimeter cones can be equipped with e-flaresFootnote 2 to aid in visibility.
These must be requested by the flight crew and are placed and activated by ground EMS personnel. They were not requested on the night of the occurrence. Approaches to and departures from the helipad are to be conducted in the southwest quadrant (210° M - 260° M).
The directory cautions of the following hazards:
- Wires under, along east and north sides of the approach/departure sector.
- Large hills south, east, and north of the site.
- Tower west and fire tower south of the site.
- Ball park east of helipad.
Additionally, there is a single house located beside the ball park, which has typical outside door entrance lights.
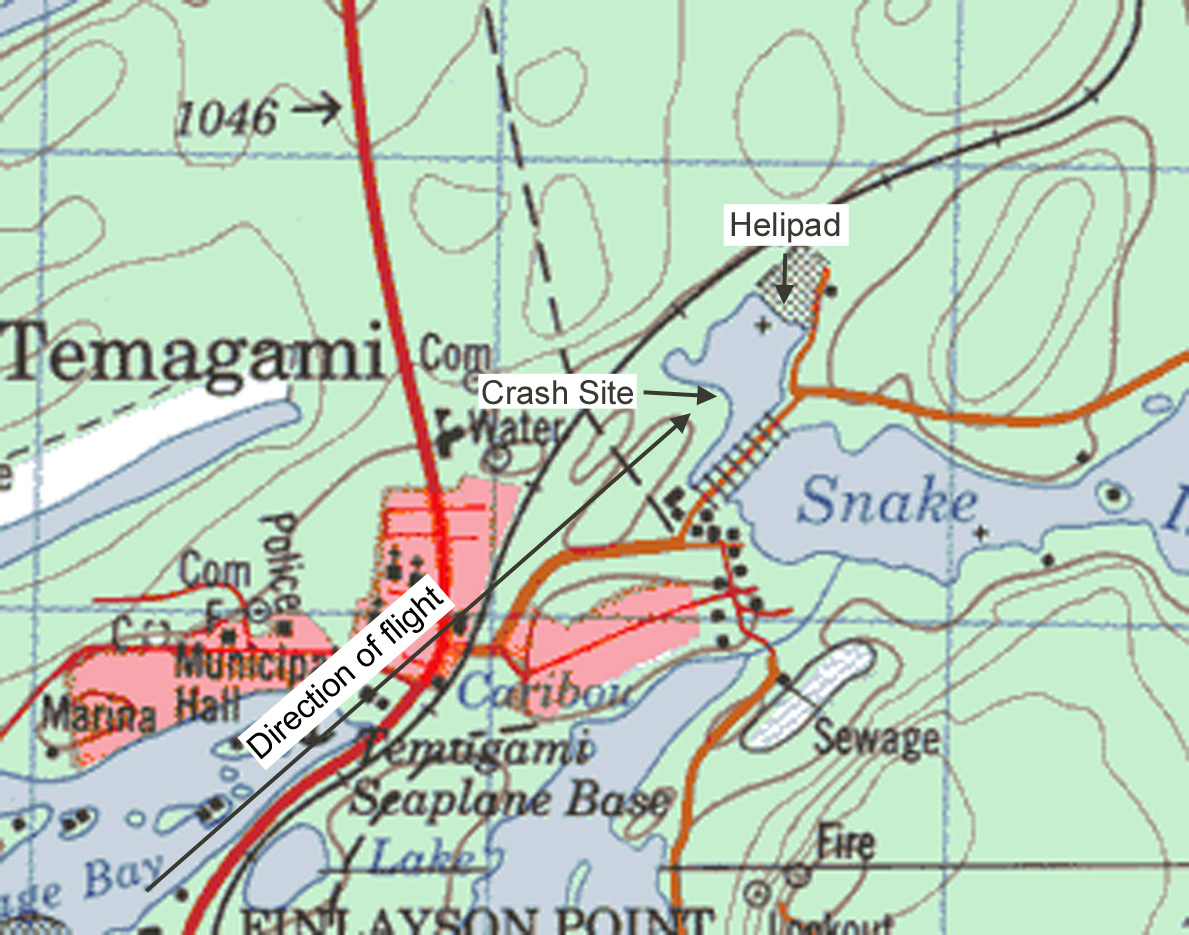
The approach to the helipad requires flying over the town and a small hill. The hill begins at approximately 2430 feet horizontally from the helipad and rises to a maximum height of approximately 1017 feet asl, approximately 20 feet above the elevation of the helipad. It then gently slopes down to meet the lake shore 723 feet horizontally from the helipad, which is located on the opposite shore of the lake (see Appendix A — Temagami Topographic Map).
The helicopter approached the helipad from the southwest on a heading of approximately 048°M and entered the trees near the edge of the lake approximately 814 feet horizontally from the helipad (see Appendix B — Snake Lake Helipad).
The trees on the approach averaged 40 feet in height. The helicopter impacted trees that were located on the downward slope of the hill, at approximately 70 feet horizontally from the shore where the height of the hill is approximately 10 feet higher than the helipad. As such, the average tree tops were approximately 50 feet higher than the helipad. The descent into the trees was near vertical with very little horizontal momentum and the nose of the helicopter came to rest approximately 15 feet from the shore. The helicopter's rotor diameter was 44 feet and the damage to the trees was mostly within this diameter. The rotor blades were completely destroyed. During the descent, a tree passed through the left landing gear bay, the main battery, and continued through the engine deck and exhaust collector of the right engine. There was evidence of heat and scorching on the tree consistent with the heat of a running engine, but no post crash fire.
There were no obvious signs of external engine damage on the left engine and the compressors of both engines appeared to be undamaged. All switches in the cockpit were consistent with an in-flight condition and the helicopter search and landing light switches were in the ON position. The power levers were in flight mode; fire handles were in the normal mode. The fuel system is a two-tank system comprised of a left tank and a right tank; the normal in-flight position for the fuel levers is the direct position, with the left tank supplying the left engine and the right tank supplying the right engine. The left fuel lever was in the cross-feed position, while the right fuel lever was in the direct position. The left fuel being in cross-feed would not affect the operation of the engine and was most likely bumped into this position after the accident.
The lap belt seat attachments for the paramedic seated in the starboard aft-facing seat failed in overload. Although the paramedic seats were equipped with four-point seat restraints, neither paramedic was wearing the shoulder harnesses.
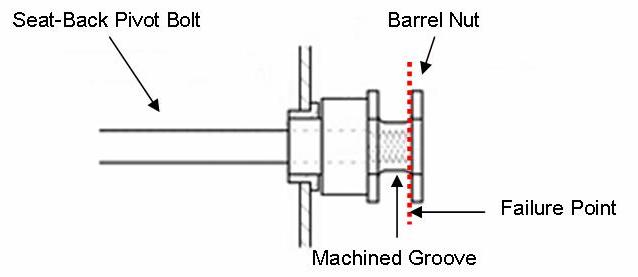
The lap belt incorporates a standard clip-on style steel hook with a spring closure that clips on to an aluminum barrel nut, which is threaded onto the seat-back pivot bolts. The seat-back pivot bolt is designed to pass through the barrel nut to the end of the machined groove. The barrel nut failed where the bolt ended (see Figure 1). There was thinning of the material in the groove of the barrel nut due to wear from the stainless steel lap belt attachment.
A detailed examination of the helicopter revealed no discrepancies that would have affected its flying characteristics. Both engines were sent to Rolls Royce for examination. The left engine was successfully started and run in a test cell and was found to be within serviceable limitations. The right engine could not be run due to damage from the impact with the tree that passed through the helicopter. No other damage was found that would have prevented the engine from running.
The helicopter was equipped with an enhanced ground proximity warning system (EGPWS), dual Garmin GNS 530 global positioning system (GPS)/Navigation/Communication units, a Latitude Technologies SkyNode satellite tracking system, and a cockpit voice recorder (CVR). These components were removed and analyzed.
The EGPWS and Garmin units contained no valuable information. The Latitude Technologies SkyNode device is a combination GPS and satellite transmitter. The device operates by periodically sending a position fix (approximately every two minutes for this occurrence) to a satellite, which relays the information to a ground station, which, in turn, sends the data to a computer server operated by Latitude Technologies, where the data is stored. An operator can contact the server and review past flights or monitor active flights. It was noted that the SkyNode device had a non-volatile memory that would retain any un-transmitted data. The examination of this showed that there was no unsent data. Therefore, there were no unsent coordinates. The transmitted data was retrieved, but the last recorded position was two miles from the helipad.
In addition to the voice and area microphone recordings, the CVR also recorded rotor rpm data. There were no operating abnormalities with the helicopter or engines prior to impact, and the helicopter was on the proper descent profile until it reached 500 feet agl and 0.5 nm from the helipad, 21.5 seconds before impact. The PF perceived that the helicopter was too high and corrected accordingly. Simultaneously, the cockpit area microphone picked up the sound of the rotor rpm increasing slightly, then decreasing just prior to impact. The rotor rpm recording also confirmed an increase and decrease in rotor rpm just prior to impact. The PNF did not question the PF's deviation from the proper descent profile, nor did he make any further speed or altitude calls after the deviation.
According to a study by the United States Air Force entitled "Running Head: BLACK HOLE ILLUSION"Footnote 3, spatial disorientation (SD) is defined by Gillingham as: "an erroneous sense of one's position and motion relative to the plane of the earth's surfaceFootnote 4." The study also states:
Visual spatial disorientation (SD) is often cited as a contributor to aviation accidents. The black hole illusion (BHI), a specific type of featureless terrain illusion, is a leading type of visual SD experienced by pilots. A BHI environment refers not to the landing runway but the environment surrounding the runway and the lack of ecological cues for a pilot to proceed visually. The problem is that pilots, despite the lack of visual cues, confidently proceed with a visual approach. The featureless landing environment may induce a pilot into feeling steep (above the correct glide path) and over-estimate their perceived angle of descent (PAD) to the runway. Consequently, a pilot may initiate an unnecessary and aggressive descent resulting in an approach angle far too shallow (below the correct glide path to landing) to guarantee obstacle clearance.
Training at Canadian Helicopters includes one hour in the simulator conducting night VFR operations. The flights are conducted to both runways and heliports where the heliports are all black holes, so black hole approach and departure techniques are required. The flights usually start with clear starry nights and then progress to overcast and reduced visibility conditions. The ceiling and visibility are increasingly reduced so that flight inadvertently goes IFR and the flight crews have to set-up and complete an IFR approach to a local airport. The exercise is usually terminated after the IFR approach.
Canadian Helicopters' Operations Manual, Part III - IFR/Night VFR, dictates the equipment requirements and procedures for performing a black hole approach. Section 1.16, Night Landing Site/Black Hole – Approach states:
1) Due to the wide variety of heliports and their locations, night landings are perhaps the most challenging of all approaches. Low (or no) illumination of the surrounding area makes reference to visual clues difficult. A structured procedure for the Night/Black Hole approach, with a heavy reliance on the aircraft instruments, is required. Preparation is needed long before commencing the final approach.
The section goes on to state the following:
4) At heliports with only one ingress/egress, care must be taken not to readily accept a downwind approach. First, look for alternate landing sites. Failing that, limit downwind approaches to a tailwind component of 15 knots.
- The PNF's radar altimeter shall be set to 500 ft and PF's radar altimeter shall be set to 150 ft.
- Establish a descent from cruise altitude to arrive at a circuit height of 100 ft agl and 80% of normal cruise indicated airspeed (IAS).
- Helipads with only retro-reflective cones must be identified and illuminated before continuing the approach.
- Structure the circuit to allow turning from base to final 1 nm back. Plan your descent to arrive at a point 0.5 nm back at 500 agl at 50 knots indicated airspeed (KIAS).
- The use of GPS is essential during the approach to determine the distance to the pad as well as determining the headwind/tailwind component.
- Every possible searchlight / landing light combination should be used to illuminate the approach path and landing zone.
- The PNF should monitor airspeed, vertical speed indicator (VSI), and radar altimeter.
- Continue with a steady rate descent from 500 ft with a gradual airspeed reduction towards landing decision point (LDP).
- Both pilots should confirm that they have good visual reference before further descent below 200 feet.
- At LDP (100 feet and VtossFootnote 5), increase collective and decrease airspeed to arrive in a stabilized hover over the landing area.
The PF's radar altimeter was not set to 150 feet during the approach and there were no altitude or speed calls after 0.5 nm and 500 feet.
Canadian Helicopters' standard operating procedures (SOPs), section 2.6.2, go on in greater detail to discuss the full procedures for the black hole hover landing. The landing profile section of this SOP calls for the following:
- Establish an approach speed of 50 KIAS at 500 feet agl. A stabilized final approach should commence with "wings level" at no less than one-half (1/2) nm back and at 500 ft. This will allow for a moderately steep approach angle of approximately 8° (16%).
- Once through 500 ft agl, adjust attitude with cyclic to slowly decelerate to a minimum of 35 KIAS. During this portion of the descent, the aircraft will be approx. 5° nose up. Torque should remain at +/-40% and should not exceed 55% (one engine inoperative limits). 750 feet per minute maximum rate of descent.
- Do not aim for the helipad. Adjust the sight picture to aim for a point beyond the intended touchdown spot. This will allow for settling as the aircraft slows below translation.
- In practice, the LDP is a variable depending on aircraft weight, wind, obstructions and helipad height. A normal LDP of 100 ft and 35 knots. However this will not apply to situations where obstructions are in the intended overshoot path. Increase height of the LDP proportional to obstructions higher than the surface of the helipad. As an example, a 30 foot obstruction along an overshoot path will require a LDP of 130 feet. Adjust the LDP accordingly. Call "committed" when no longer able to overshoot.
- After passing LDP, increase collective slightly and adjust attitude to slowly decelerate further. Torque should increase through 55% as the aircraft passes over the forward portion of the helipad. Adjust the flare to arrive over the touchdown zone at approximately 25-30 ft. agl while simultaneously increasing power to control rate of descent.
- Continue to raise collective to terminate in a hover.
Analysis
There were no anomalies found with the helicopter that would have contributed to the accident. Therefore, this analysis focuses on the operation of the helicopter.
The Snake Lake Helipad is a classic black hole approach helipad. Temagami itself is a small community and the location of the helipad is on the northeast edge of town. The approach is flown over the town and past all the lights with a relatively featureless landscape forward. The only visible lights are those of the house beside the ball park. On the terrain along the approach path, a small hill begins to rise approximately 2430 horizontally feet from the helipad. The maximum rise is approximately 20 feet, which then gently slopes back down to the lake surface 723 feet horizontally from the helipad. The mature trees along the flight path would further increase the obstacle height another 40 feet. However, the steep approach angle of 8° into the landing site would have provided for adequate clearance above the trees to land safely.
The black hole approach requires diligent monitoring of the helicopter's instruments. The flight crew followed most of the SOPs during the approach and appropriate calls were made. In this case, the PNF was monitoring the air speed, altitude and distance to the helipad. He relayed this information to the PF regularly. The PF, flying a visual approach, utilized the information from the PNF in addition to the visual cues for reference. However, the PF's radar altimeter was not set to 150 feet as called for by the operations manual. This would have provided an additional cue to the flight crew that the helicopter was approaching the ground too soon during the descent into the helipad. Meanwhile, the helicopter was on a stabilized approach with the proper 8° descent profile, as required by the operations manual and the SOP.
During the 1.5 minutes of the approach, the PF's attention was split between flying the approach and explaining why things were happening and what to watch for during a black hole approach. This likely distracted the pilots to the task at hand. In this case, the PF acknowledged a 0.5 nm and 500 foot call, an on-profile condition, but visually perceived that the helicopter was too high and, therefore, increased the rate of descent. This coincides with the increase in the rotor rpm; an indication that the collective is being lowered, decreasing the load on the rotor blades and increasing the descent rate. This was followed by a decrease in rotor rpm, as the collective was raised, increasing the load on the rotor blades and decreasing the descent rate just prior to impact. At no time did the PNF question the PF's deviation from the proper descent profile nor did he make any further speed or altitude calls after the deviation.
Based on the available information, a descent from 500 feet to impact in less then 21.5 seconds equates to a descent rate of more than 1400 feet per minute – well in excess of the recommended maximum descent rate of 750 feet per minute. The increased descent rate caused the helicopter to descend into the trees before either crew member realized what was happening.
The lap belt barrel nut attachment failed due to several factors. First, the barrel nut was weakened due to wear from the stainless steel lap belt attachment. Second, the seat-back attachment bolt did not pass completely through the barrel nut, but instead passed only part of the way through to the end of the machined groove. This created a weak point on the assembly at the outside edge of the barrel nut. Under normal loads, such as forward and aft g-forces, this would not be an issue because the main load would be over the machined groove and seat-back attachment bolts. However, with a side impact, the main loads are in a sideways direction on the end barrel nut. This placed an abnormal load on the end of the barrel nut, which caused it to fail at the weakest point.
The following TSB Engineering Laboratory report was completed:
- LP 034/2008 – Analysis of Aircraft Data
This report is available from the Transportation Safety Board of Canada upon request.
Findings
Findings as to causes and contributing factors
- The pilot flying (PF) was likely affected by visual spatial disorientation and perceived the approach height of the helicopter to be too high. While correcting for this misconception, the helicopter descended into trees 814 feet short of the helipad.
- The pilots were likely distracted during the critical phase of the approach and did not identify that the helicopter had deviated from the intended approach profile and recommended descent rates.
Findings as to risk
- The right rear aft-facing paramedic seat lap belt attachment barrel nut was worn in the groove where the seat belt attaches, weakening the barrel nut's structural integrity, thereby increasing the risk of failure.
- The helicopter crashed on its side, placing an abnormal side load on the right rear aft facing paramedic seat lap belt attachment barrel nut, thereby causing it to fail.
Safety action
Following the occurrence, JCM Aerodesign Limited, the supplemental type certificate (STC) holder for the emergency medical services (EMS) interior utilized in the S-76, issued Service Bulletin No. SB-EMS76-1. This service bulletin identified the affected helicopters and called for the replacement of the existing barrel nut lap belt attachment with a steel shackle. All affected helicopters have complied with the service bulletin.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on