Loss of Control - Collision with Building
Piper PA-34-200 Seneca C-GHFD
Richmond, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
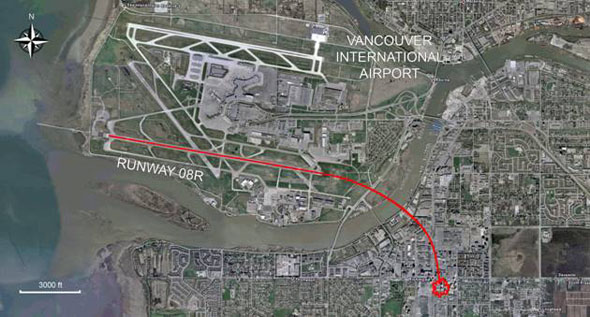
At 1602 Pacific daylight time, the privately registered Piper PA-34-200 Seneca (registration C GHFD, serial number 34-7350210) was cleared for takeoff from Runway 08 Right at the Vancouver International Airport destined for Pitt Meadows Regional Airport. The flight was operating under visual flight rules with only the pilot on board. Shortly after takeoff, communications and radar contact were lost. The aircraft collided with a 15-storey residential building in Richmond, about 1.5 nautical miles east-southeast of the departure end of Runway 08 Right. The pilot was fatally injured. There was no post-impact fire. The aircraft entered a suite occupied by two people; one received serious non-life-threatening injuries, the other received minor injuries. Structural damage to the building was minimal, but there was extensive water damage from the fire suppression system. As a result, hundreds of people were displaced from their homes for extended periods. There were no other reported injuries.
Factual information
History of the Flight
Pitt Meadows Regional Airport is about 19 nautical miles (nm) east-northeast of the Vancouver International Airport, but the pilot requested a southbound departure in order to check some maintenance work that had recently been done on the aircraft. The flight was approved for the published Vancouver VOR Footnote 1 departure from Runway 08 Right (R08R), which requires a right turn, at pilot's discretion, to a heading of 160° magnetic toward the Vancouver VOR (7 nm south) and to climb to 2000 feet above sea level (asl). When climbing through 1000 feet asl, the pilot is required to change from the inner to the outer south tower frequency.
The takeoff roll commenced near the runway threshold shortly after 1602 Footnote 2. The aircraft lifted off and then flew the full length of the runway (10 600 feet) before commencing the right turn. A transponder reply (secondary surveillance radar return) was never received from the aircraft, though Transponder ON was listed among four tasks to be completed under the final item on the before-takeoff checklist Footnote 3. The primary radar returns, which do not provide aircraft identification or altitude information to the controller, were intermittent and first appeared abeam the departure end of the runway. The returns displayed a track consistent with the planned departure procedure.
Communications were normal throughout the pre-taxi, taxi, and takeoff phases of the flight. When the aircraft was in the right turn, the tower controller directed the pilot to change frequencies and to turn his transponder on. The pilot did not acknowledge these instructions and a secondary surveillance radar target never appeared. The last primary radar return occurred 5 seconds later at about 1 nm southeast of the departure end of the runway and 0.5 nm northwest of the accident site.
During the turn, the altitude profile of the flight changed from a climb to a descent. The airspeed was calculated to be about 141 mph passing the departure end of the runway (above the manufacturer's recommended climb speed of 120 mph) and the aircraft accelerated continuously to 174 mph at the last radar return before the collision.
The aircraft was at a low altitude the entire time it was airborne. The aircraft's altitude was estimated at about 400 feet above ground level (agl) shortly beyond the departure end of R08R, and at about 200 feet agl by the time it crossed a location about 0.25 nm northwest of the accident site. The aircraft was travelling at high speed, with the landing gear retracted. The sound of the engines was normal to very loud. The aircraft was in a right bank and in a steady, shallow descent (See Figure 1).
Weather
The weather at the Vancouver International and the Pitt Meadows Regional Airports was suitable for flight under visual flight rules (VFR) at the time of departure. Weather is not considered to be a factor in this accident.
Aircraft Damage
The aircraft entered the residential building in a right bank (see Photo 1). The left engine entered the apartment building with the fuselage through a large window. The right engine directly impacted the building's 9th floor exterior concrete wall, separated from the aircraft, and fell to the 4th floor parking lot. Damage signatures from the right engine showed the last one half of a revolution during the impact before stopping. The right engine was severely damaged and could not be disassembled. An examination was conducted on the left engine and did not reveal any evidence of pre-impact damage that would have prevented normal operation.

The damage to both propellers was indicative of rotation with power at the time of impact. Engine power output could not be ascertained. There were no discrepancies noted that would preclude normal operation. All damage was consistent with impact damage.
Examination of the wreckage did not reveal any aircraft structural deficiencies, engine or system failure. There was no indication of external interference, such as a bird strike or other emergency situation, before the collision with the building.
Fuel
One hundred and twenty litres of 100LL Avgas had been added six days before the accident. This is the correct type of fuel for the aircraft and no difficulties were reported with the aircraft or others regarding the quality of the fuel. The pilot drained the fuel sumps and used a dipstick to check the fuel quantity during the pre-flight walk-around before departing Vancouver.
Both fuel selector valves, which incorporate cross-feed capability, were examined and no issues were identified. Fuel lines from the main tanks through to the engines were damaged and/or severed in numerous places at impact. The aircraft had spent about 15 minutes running on the ground prior to takeoff. An examination of the engine instruments determined that the right hand fuel flow indicator registered a reading of 14.5 to 15 United States (U.S.) gallons per hour at the time of impact. This figure corresponds with a power setting of full throttle and 2500 rpm (2700 rpm maximum). The left-hand fuel flow indicator did not provide any meaningful information.
Airframe
All flight control surfaces were recovered. Continuity of the primary pitch, roll, and yaw control cables was established and no defects were identified that would have prevented normal operation.
The stabilator incorporates an anti-servo tab that provides longitudinal trim. The anti-servo tab manual control system was examined and no pre-existing defects were identified. The anti servo tab jack screw was free and easy to operate in both directions; extension was measured to be about halfway between the neutral and full nose-down positions, which is consistent with the flight profile. When the autopilot is not engaged, a pitch trim servo provides manually activated electric trim via the manual electric trim operation/autopilot disconnect toggle switch mounted on the left grip of the pilot's control wheel. The electric trim switch was tested to the extent possible and no anomalies were identified. The roll control system does not incorporate an adjustable trim system.
The vertical stabilizer was separated from the fuselage upon impact with the building's 10th floor slab. The rudder remained partially attached to the stabilizer. The rudder trim jack screw extension was measured to be at full right tab deflection, which equates to a left rudder input. The rudder trim jack screw assembly was damaged and could not be operated in either direction. The rudder tab deflection is not consistent with other data collected regarding the aircraft flight profile.
Weight and Balance
The aircraft weight at the time of takeoff was estimated to be approximately 3600 pounds (maximum allowable is 4200 pounds) and the centre of gravity was within the prescribed limits.
Avionics
The aircraft was equipped with two navigation/communication (NAV/COM Footnote 4) units. The #1 NAV/COM unit incorporated global navigation system (GNS) capability. The NAV/COM unit has four selectable frequencies–one active and one stand-by for NAV, one active and one standby for COM. Of all four selected VHF frequencies recovered from the #1 unit, only one navigation frequency was applicable to the Vancouver area and was selected to the Vancouver International Airport's VOT Footnote 5 frequency.
The #2 NAV/COM unit was selected to the Vancouver south (inner) tower frequency of 118.7 MHz; the navigation frequency could not be determined due to damage. The pilot could have selected the Vancouver VOR on the #1 NAV through the GNS function, which would not have required the selection of a frequency, or he may have intended to navigate to the Vancouver VOR by visual reference. A second panel-mounted GNS unit was destroyed and no data was recovered. Neither of the two GNS units installed in the aircraft were capable of storing recorded route data.
Aircraft Accident and Maintenance History
The pilot had three previous accidents with this same aircraft in 1979, 1998, and 2006, each resulting in substantial damage. Extensive repairs had recently been completed following the 2006 accident. Although not all maintenance records were provided, examination of the wreckage did not reveal any evidence of pre-impact failures or signs of substandard workmanship or materials.
One week prior to the occurrence, the aircraft was flown to a Transport Canada (TC) approved maintenance organization (AMO) in Vancouver for maintenance on three avionics items:
- the completion of a planned upgrade of the #1 NAV/COM unit;
- the verification of the altitude reporting function Footnote 6 of the transponder; and
- the pitch command function of the autopilot system.
The records for this maintenance were complete.
The altitude reporting function of the transponder was repaired, the unit was reinstalled, and it tested satisfactorily. The transponder was extensively damaged after the accident; it could not be determined whether it was turned on or not by the pilot before flight. The non-operation of the transponder did not have any bearing on the accident, but did limit the recorded flight data available to investigators.
The aircraft was equipped with an Altimatic IIIB-1 autopilot that provides pitch and roll control but not direct yaw control through the rudder or the rudder trim tab. Aileron/rudder interconnect cables provided some indirect rudder control through roll command inputs. This aircraft was equipped with a toggle-style trim switch and, in combination with the autopilot, incorporated an autopilot trim sensor. This sensor automatically controls pitch trim servo operation when the pitch command function of the autopilot is engaged.
During the pilot's recent recurrent training, while enroute, it was reported that the autopilot caused a nose-down pitch when the pitch command function was engaged. This resulted in the pilot having to disengage the autopilot. Maintenance action did not find any anomalies with the autopilot pitch system, but determined that the altitude hold calibration was out of adjustment, which could have led to the symptoms that the pilot observed. The altitude hold function was recalibrated and the pitch system was re-checked and found to be serviceable. The position of the stabilator trim and whether the electrical power switch for the pitch trim was left ON or OFF after the aircraft was released from maintenance could not be determined. A maintenance release was signed subject to a satisfactory test flight.
Because the accident flight was the test flight, it is not known whether the repair to the autopilot corrected the symptom reported by the pilot. The recovered autopilot and electric trim components were examined at the TSB Engineering Laboratory. The autopilot control system was substantially damaged. Of all parts and components that could be examined, no evidence of improper functioning was identified.
The autopilot is engaged at the pilot's discretion. The autopilot is not used for takeoff and it could not be determined whether it had been engaged at any time during the flight. It would be unusual for a pilot to turn the system on immediately after lift-off on the first test of the system after maintenance. If the autopilot is engaged and a pitch problem is experienced, there are a number of ways to disengage the autopilot, including manually overriding the autopilot. During recurrent training the pilot demonstrated the ability to overcome the problem reported with the autopilot.
Flight Operations
The PA-34-200 pilot operating manual (POM) describes the pre-flight procedure to verify the correct operation of the electric pitch trim system. The procedure for an electric pitch trim malfunction is to disengage it by operating the push-button pitch trim electrical power switch on the instrument panel. In an emergency, the electric pitch trim may also be overpowered using the manual pitch trim wheel. While a pre-takeoff checklist recovered from the accident site did not include an item to remind the pilot to turn on the electric power switch for the pitch trim, it is completely functional in manual mode.
The POM recommends a lift-off speed of 85 mph and a cruise climb speed of 120 mph. The pitch trim setting for takeoff should be set within the takeoff range on the pitch trim position indicator. The pre-takeoff checklist included the item of "TRIM (STABILATOR AND RUDDER) – SET." When the pitch trim is set in the takeoff range, only light back pressure on the control wheel is required to lift the aircraft off the ground, after which the aircraft should maintain a speed slightly above 85 mph. Without any additional pilot input, an aircraft will attempt to achieve and maintain the airspeed for which the pitch trim is set, for a given power setting. Setting the pitch trim in any phase of flight is a process of adjustment to find the setting that will maintain the desired airspeed. The pilot can modify the pitch attitude by physically pushing or pulling on the control wheel to change airspeed, but setting the pitch trim relieves the pilot of this constant effort. After takeoff, the pitch trim would then be selected to a more nose-down position for the desired climb speed.
A demonstration was conducted using the same model of aircraft in a similar weight and balance configuration as the subject aircraft to determine the behaviour and flight control forces in similar manoeuvres and speeds as the accident flight. It was determined that push forces of 40 pounds are needed on the yoke to accelerate from a trimmed speed of 120 mph to 174 mph at climb power. The pilot could not exert this level of force on the control wheel with his torso by leaning forward, even with the seat belt and shoulder belt fully loosened. This observation, combined with the seat position in the Seneca being similar to that of a sports car (low to the floor with legs extended ahead), makes it extremely unlikely for an incapacitated pilot to have fallen forward on the control wheel and exerted the required 40 pounds of force. A nose-down trim setting, as found, is consistent with the acceleration (174 mph +). It could not be determined if the trim setting was made before or after takeoff.
A pilot can normally overcome control forces caused by trim settings. The effect of a nose-down pitch trim following takeoff, when a climb is desired, would be a requirement for the pilot to physically hold a pitch-up input until the trim can be reset manually or via the electric pitch trim, to achieve a hands-off condition at the desired airspeed. Regardless of what the trim position was, the pilot did rotate the aircraft for lift-off and initiate a climb.
Pilot
TC records indicated that the pilot was 82 years of age and held a Canadian Private Pilot Licence–Aeroplane validated by medical certificate until 01 October 2008. The pilot had held an instrument rating that expired on 01 March 2007. The validity period of a medical certificate for a private pilot changes from 60 months to 24 months at a pilot's 40th birthday. Canadian Aviation Regulation (CAR) 401.05 and Commercial Air Service Standard (CASS) 421.05 deal with pilot recency requirements. However, there is no regulatory requirement for a specific evaluation of cognitive and motor skills through recurrent flight testing or medical examination for private pilots.
The pilot's last aviation medical examination and electrocardiogram test was completed on 11 September 2006. The medical certificate was valid with one limitation–glasses must be worn. The pilot also held a U.S. private pilot licence. The last U.S. aviation medical examination was completed on 15 September 2006 and validated the licence, with the same limitation, until 01 October 2008.
The pilot's personal flight log recorded total flight time as 5800 hours, of which nearly 5300 were recorded on the Piper PA-34-200 model. The aircraft was damaged in an accident in February 2006 and the pilot had not flown again until 31 August 2007. Log book entries recorded 8 hours of multi-engine re-currency training since 31 August 2007.
Anecdotal descriptions of the pilot's demeanour indicated that he was feeling good and was repeatedly described as being very sharp and having a good memory. He was enjoying life with many plans in progress and was anxious to start flying again after repairs were completed.
A post-mortem examination of the pilot was carried out, but was limited due to the extensive physical trauma. No evidence was found of a heart attack. Evidence associated with hypertension was identified. Toxicology tests were negative except for a small amount of carboxyhemoglobin, possibly from the earlier ride to the airport (exhaust smell in vehicle was reported), but was within normal limits. No evidence of the medication used to control blood sugar levels was detected. It is not possible for a post-mortem examination to determine a person's level of consciousness prior to death or to identify all causes of death. The pathology report attributed the pilot's death to multiple blunt force injuries, but also stated that the possibility of the pilot's death just prior to the collision could not be excluded.
Pilot's Medical History
Risk factors that may have increased the likelihood of sudden incapacitation were considered. The pilot's personal medical records identified evidence of a previous heart attack (10 or more years ago) and two chronic conditions, Type II diabetes and hypertension, that existed for at least 4 and 20 years, respectively. In addition to the pilot's age and obesity, both of these conditions are risk factors associated with the development of coronary heart disease Footnote 7 and were being controlled with oral medication. Medications can mask the symptoms of existing conditions and, therefore, make their identification unlikely in a routine examination.
The civil aviation medical examiner (CAME) who carried out the pilot's aviation fitness assessment for the years 1995 to 2006 became the pilot's personal physician in 2004. The pilot never disclosed his diabetes and hypertension to the physician until new concerns were identified in the 2006 aviation medical examination. The pilot continued to fly solo in accordance with his valid medical certificate. The pilot's CAME prior to 1995 had not recorded the hypertension condition or medication either and it is unknown if he was aware of this condition.
The TC Civil Aviation Medicine (CAM) Handbook for Civil Aviation Medical Examiners (TP13312) provides guidance for cardiovascular (CV) risk factors to be identified on the examination form. TP13312 stipulates that this is a shared responsibility with the onus on the applicant to report any symptoms and on the physician to conduct a careful and thorough examination.
None of the U.S. aviation medical examination reports identified any new issues, and the hypertension, diabetes, and the medications taken were not reported in the section completed by the pilot. The pilot's medical records since year 2000 recorded two electrocardiogram tests (ECGs), in 2002 and 2006 respectively.
For pilots diagnosed with diabetes, TP13312 states:
A cardiovascular assessment to include an exercise electrocardiogram is required at the age of 40 and then 5 yearly to age 50. After the age of 50 it should be completed every two years. A resting ECG will be required yearly.
Had the pilot declared his conditions, he would have been required to complete an exercise electrocardiogram every two years and a resting electrocardiogram yearly.
In the 2006 CAME report, a new cardiac abnormality was identified from the ECG and the conditions of diabetes and hypertension were both recorded on the form for the first time (after being disclosed to the physician) along with a recommendation for follow-up testing. The TC Regional Aviation Medical Officer (RAMO) took prompt action to ensure the issue was investigated further by specialists. Further testing confirmed deterioration in the cardiac conduction system (sporadic notes of this condition were recorded as early as 1991) and reasons for testing in 2006 included dizziness and palpitations. One of the tests was a stress nuclear perfusion imaging study (in lieu of an exercise stress test), which is considered to be more sensitive and specific than routine exercise stress testing. When all of the test results were reviewed in accordance with the TC screening process, it was concluded that the pilot's conditions met the TC requirements and, therefore, the medical certificate was validated.
The combination of hypertension, diabetes, obesity, and age, along with the deterioration in the cardiac conduction system means that a medical event resulting in incapacitation can not be ruled out. The nature of incapacitation can involve a partial loss of consciousness, which may or may not precipitate a total loss of consciousness. As one transitions from a state of consciousness to unconsciousness, the ability to control voluntary muscles may be affected.
Medical Requirements for Pilots
Currently, pilots are exercising licence privileges with medical conditions that would have been disqualifying one or two decades ago because there are now more explicit processes for managing the safety risks associated with these conditions. Frequently, the CAME is not the candidate's personal physician and must rely, to a large extent, on information disclosed by the candidate. TP13312 acknowledges this:
Aviation personnel, although not basically dishonest, may not volunteer information which may affect their medical certification.
On occasion, the CAME or the TC RAMO may wish to review previous medical records regarding some concern, but can only obtain complete medical documentation with the candidates' written permission, Footnote 8 which may be refused. CAR 404.04(3) provides TC with the authority to request any additional medical information necessary to determine whether the holder continues to meet the medical fitness requirements specified in the personnel licensing standards and to suspend, or refuse to renew, the holder's medical certificate if the holder fails to comply with the request. However, this requires that the CAME advise TC that further review is required.
For the period 01 January 1976 to 31 October 2008, the TSB database has 272 occurrences that had a medical condition or incapacitating event identified as a contributing factor. Of these, at least 25% (68 occurrences) involved pilots with a private pilot licence and 40% (109 occurrences)involved fatalities. Cardiovascular issues accounted for 13% (35 occurrences), of which 80% (28 occurrences) involved fatalities. Of the 35 cardiovascular occurrences, pilot age was recorded for about half and averaged 55 years. Statistics provided by Transport Canada indicate that in 1998 there were 2290 persons over 65 years of age with a valid Canadian private pilot licence for fixed wing or rotary wing aircraft. By 2008, while the total number of private pilots had decreased by 3%, the number of private pilots aged 65 and over had increased by 48% to 3380. Of these, 88 were over the age of 75.
The TC Civil Aviation Medical Examination Report form contains a table (See Figure 2) that can be used by the examiner to indicate six cardiovascular risk factors. However, use of the table is voluntary and no explicit instructions regarding the meaning of check marks or the absence thereof are provided. In 2006, the pilot met the criteria for three of these factors. None was indicated in the table; two appeared for the first time in other parts of the form. This table does not include age as a cardiovascular risk factor, nor is age mentioned anywhere on the form except for the date of birth entered by the candidate. The guidance material does not contain a requirement to carry out testing for serum lipids, although the table provides a space to record any information available.
Age is a dominant concern in assessing cardiovascular risk as indicated by the many references in TC guide TP13312. TP13312 provides guidance to CAMEs and RAMOs and is written and applied to support medical judgement that TC regards as an essential aspect of the pilot medical fitness assessment process. The guide has a table that contains risk factors related to age (up to 74 years), but only in a section related to cholesterol levels. TP13312 does not provide guidance concerning age across the range of medical factors relevant to pilot fitness for duty.
TP13312 states:
Since the prevalence of ischemic heart disease increases with age, the utility of routine electrocardiography improves after age 50 and with the presence of major risk factors for ischemic heart disease. The current recommendations for routine electrocardiographic testing which stratify the frequency of testing by age are considered adequate. Compared with a resting electrocardiogram, exercise electrocardiography increases the likelihood of detection of coronary artery disease. The number of true-positive results is increased significantly if such testing is applied only to those who are more likely to have coronary artery disease, such as those with symptoms of angina, those for whom major risk factors are present, and those in older age groups.
Advanced age is one of the risk factors associated with medical incapacitation. Given the debate in recent years about raising the retirement age of commercial pilots in the U.S. from 60 to 65, Footnote 9 the majority of scientific studies on pilot incapacitation have focused on commercial multi-crew pilots below the age of 70.
The significance of cardiovascular incapacitation as a factor in flight safety for commercial pilots over age 70 is less clear. Current guidance to TC medical examiners regarding age-related medical risks is limited to pilots below 74 years of age and focuses on cardiovascular events only, rather than additional safety critical factors such as acute neurological events and degradation of cognitive performance.
As cognitive processes degrade with age, older adults become less able to divide attention among sub-tasks and to smoothly overlap information processing stages. Specific age-related cognitive deficits have been found on complex tasks, divided attention, and multiple tasks. Research has demonstrated substantial deterioration of frontal lobe functioning with age, resulting in decreased executive control and impaired attention control strategies and coordination of multiple tasks. Footnote 10,Footnote 11
Analysis
The identification of the factors that contributed to this accident was hampered by significant destruction of the aircraft and minimal recorded information. Three possible accident scenarios were considered: an intentional act, an equipment problem and pilot response, and pilot incapacitation. These scenarios are analyzed below.
First Scenario – an Intentional Act
The first scenario is that the pilot intentionally flew the aircraft into the building. The pilot's demeanour, his making of ongoing plans, his concern about the correct operation of the aircraft systems, and the care taken to prepare the aircraft for this flight are inconsistent with such a scenario. The TSB investigation did not reveal any indication to conclude that an intentional effort was made to place the aircraft, or anyone, in jeopardy.
Second Scenario – Equipment Problem and Pilot Response
The second scenario involves a problem with the aircraft or its configuration that the pilot was unable to resolve during the short flight. Several aircraft systems with the potential to affect aircraft performance during the flight were examined and all but two potential system problems were eliminated. This left the possibility of an autopilot electrical malfunction or an electric pitch trim malfunction.
Because this was the first flight following maintenance on the pitch command function of the autopilot system, it would be unusual for the autopilot to have been engaged at such a low altitude, especially in view of the nature of the original complaint. Component damage prevented complete testing of these systems after the accident, but to the extent these systems could be examined, no anomalies were identified.
Following the accident, the anti-servo trim tab on the stabilator was found to be in a moderate nose-down position and the rudder trim was at full right deflection (left rudder input). It could not be determined if either trim setting was made before or after takeoff. It is possible that the pilot inadvertently omitted the checklist item to check and set either or both trims prior to takeoff. A nose-down trim would require the pilot to exert more back pressure to rotate the aircraft during the takeoff roll and could account for the much higher than normal speed over the departure end of the runway. It could not be determined if the electric power switch for the pitch trim was ON or OFF. There was no pre-takeoff checklist item reminding the pilot to turn the electric trim ON. If OFF, the pilot would have had to either turn it on to regain electric pitch trim functionality, or use the manual trim wheel to adjust the pitch trim. If an electric pitch trim runaway occurred during flight, it could be expected that it would have travelled to its limit (full nose-down position) unless pilot intervention limited the travel.
The pilot's experience and skill level should have been sufficient to overcome such events and he had previously demonstrated his proficiency at altitude to deal with a faulty pitch command function of the autopilot during recurrent training. It was considered a possibility that degraded cognitive performance may have affected the pilot's ability to identify, diagnose, and correct an unexpected pitch or rudder trim anomaly while controlling the aircraft's attitude in the brief time after takeoff and before the collision with the building. However, no evidence of symptoms of reduced cognitive functioning was identified during the investigation.
Therefore, the investigation concluded that it is unlikely there was any system malfunction that could not have been readily overcome by the pilot.
Third Scenario – Pilot Incapacitation
The third accident scenario involves the possibility of an acute medical event resulting in pilot incapacitation. The pilot was diagnosed with several cardiovascular risk factors, making an acute cardiovascular decompensation a possibility. An equally plausible possibility is an acute neurological event (such as a seizure or stroke). The routine medical examination did not detect impairment of cognitive processes or other neurological functions; therefore, further testing was not conducted.
The normal and loud engine operating sounds provided an indication of normal engine and propeller operation, which was confirmed by post-accident examination. High-engine power available from both engines would have contributed to reducing the angle of descent. A conscious pilot would have likely made some effort to correct the descent, to manoeuvre away from the building, or to communicate with air traffic services.
Demonstration showed that it is extremely unlikely for an unconscious pilot to have collapsed onto the control wheel and to have caused the loss of control resulting in the unchecked descent. Therefore, the change from a climb to a descent due to unconsciousness could be the result of two possibilities: the pilot being unable to maintain overriding control input in response to an anomalous pitch trim condition, or a less likely scenario of the pilot making an autonomic electric pitch trim command during the transition toward unconsciousness. In either case, it follows that the aircraft was accelerating in a descent because it had not achieved the airspeed corresponding to the pitch trim position. The erroneous pitch trim setting was not successfully addressed, and before the aircraft could achieve the corresponding speed and level off or resume a climb, it descended below the height of the building and collided with it.
The pilot had pre-existing health risk factors, making it possible that he suffered an acute medical event resulting in incapacitation and a loss of control of the aircraft. The investigation concluded that this is the most plausible scenario.
Medical Examinations
Prior to 2006, none of the pilot's cardiovascular risk factors, or the medication taken, was recorded on the Canadian Aviation Medical Examination (CAME) reports because the pilot had not disclosed these conditions and the symptoms were masked by medication. These conditions were also not reported by the pilot on any of his U.S. aviation medical examination report forms. However, once these conditions were disclosed, further medical testing was conducted and there were no medical findings at the time to preclude unrestricted TC medical certification.
Non-disclosure of medical symptoms or chronic conditions to CAMEs bypasses some of the safety benefit of examinations and may pose a risk of incapacitation while flying. Present legislation provides TC (CAM) with the authority and the means to obtain any additional medical information necessary to investigate suspicious conditions when relevant evidence indicates a need to do so. However, where there is no basis to do so because a pilot has not disclosed a condition to their CAME, the risk to public safety is increased.
A comparison of the information that was known to the CAME with the information formally documented using the cardiovascular risk factors table on the TC Civil Aviation Medical Examination Report form demonstrates two potential problems. First, the cardiovascular risk factors table was not used and, second, the guidance material concerning this table in TP13312 is inadequate to ensure its utility as a risk management tool. Because completion of the cardiovascular risk factors table on the TC Civil Aviation Medical Examination Report form is voluntary and the meaning of a check mark, or no mark, in a box is not defined, there is a risk that this information will not be recorded or used effectively in the medical examination.
Furthermore, the current guidance material in TP13312 concerning the assessment of cardiovascular risk factors was last updated in 2003, based on information exchanged at a workshop Footnote 12 held in 2001. While the guidelines may provide sufficient guidance to examiners to assess cardiovascular risk, there has been a significant evolution of the understanding of coronary atherosclerosis since 2001. In addition, the guidelines in TP13312 do not address the complete range of conditions that may be affected by age, such as changes in neurology and in cognitive performance. Although medical practitioners use various means to remain current and revise their practice accordingly, improving the guidelines in TP13312 could reduce the risk associated with varying individual judgement decisions.
Data Collection
The opportunity to gather valuable data regarding the flight path of the aircraft was lost because neither of the two GNS units installed in the aircraft were capable of storing recorded route data. The Board remains concerned Footnote 13 that manufacturers and designers of equipment containing memory devices may not consider their potential for accident investigation purposes.
The following TSB Engineering Laboratory Reports were completed:
- LP 009/2008 – Autopilot, electric pitch trim components, engine
- LP 129/2008 – Engine exhaust component analysis
Findings
Findings as to causes and contributing factors
- The pilot had pre-existing health risk factors, making it possible that he suffered an acute medical event resulting in incapacitation and a loss of control of the aircraft.
- With the pitch trim at an inappropriate setting, the aircraft accelerated in a descent below the height of the building and collided with it.
Findings as to risk
- Non-disclosure of medical symptoms or chronic conditions to civil aviation medical examiners (CAMEs) bypasses some of the safety benefit of examinations and may pose a risk of incapacitation while flying and, as such, a risk to public safety.
- TP13312 does not address the complete range of conditions that may be affected by age, does not include significant advances since 2001, and does not cover the age range above 74. The guidelines, therefore, are of limited value in assisting CAMEs to detect all pilots with age-related medical risk factors.
Other findings
There is no evidence to suggest that the pilot intentionally flew the aircraft into the building.
The manufacturers and designers of equipment containing memory devices may not consider their potential use for accident investigation purposes.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .