Sinking and loss of life
Tug Ingenika and barge Miller 204
Gardner Canal, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 10 February 2021, the tug Ingenika, with 3 crew members on board, was towing the loaded barge Miller 204 in the Gardner Canal when the tug sank approximately 16 nautical miles west‑southwest of Kemano Bay, British Columbia. The barge subsequently drifted and went aground about 2.5 nautical miles southwest from where the tug sank. The search and rescue operation located 1 surviving crew member on land and recovered the bodies of the 2 other crew members from the water. The barge was recovered; the tug was not found. At the time of the occurrence, the tug had 3500 L of diesel fuel in tanks on board.
1.0 Factual information
1.1 Particulars of the vessels
| Name of vessel | Ingenika | Miller 204 |
|---|---|---|
| Official number | 329577 | 802725 |
| Port of registry | Vancouver, BC | New Westminster, BC |
| Flag | Canada | Canada |
| Type | Tug | Barge |
| Gross tonnage | 14.63 | 849.46 |
| Length | 11.06 m | 60.96 m |
| Breadth | 4.72 m | 15.24 m |
| Depth | 1.65 m | 2.80 m |
| Built | 1968 | 1982 |
| Propulsion | 2 diesel engines of 526 kW (in total) driving twin-screw fixed-pitch propellers in Kort nozzles | Non-propelled |
| Crew | 3 | n/a |
| Registered owner and authorized representative | Bates Properties Ltd. | Bates Properties Ltd. |
| Managing / operating company | Wainwright Marine Services | Wainwright Marine Services |
1.2 Description of the vessels
1.2.1 Ingenika
The Ingenika (Figure 1) was a twin-screw tug with a steel hull. It had a single flush deck, a raked stem, a round stern, and a hard chine. The hull was subdivided by 2 transverse watertight bulkheads. The bulkheads separated the accommodation, the engine room, and the lazarette.
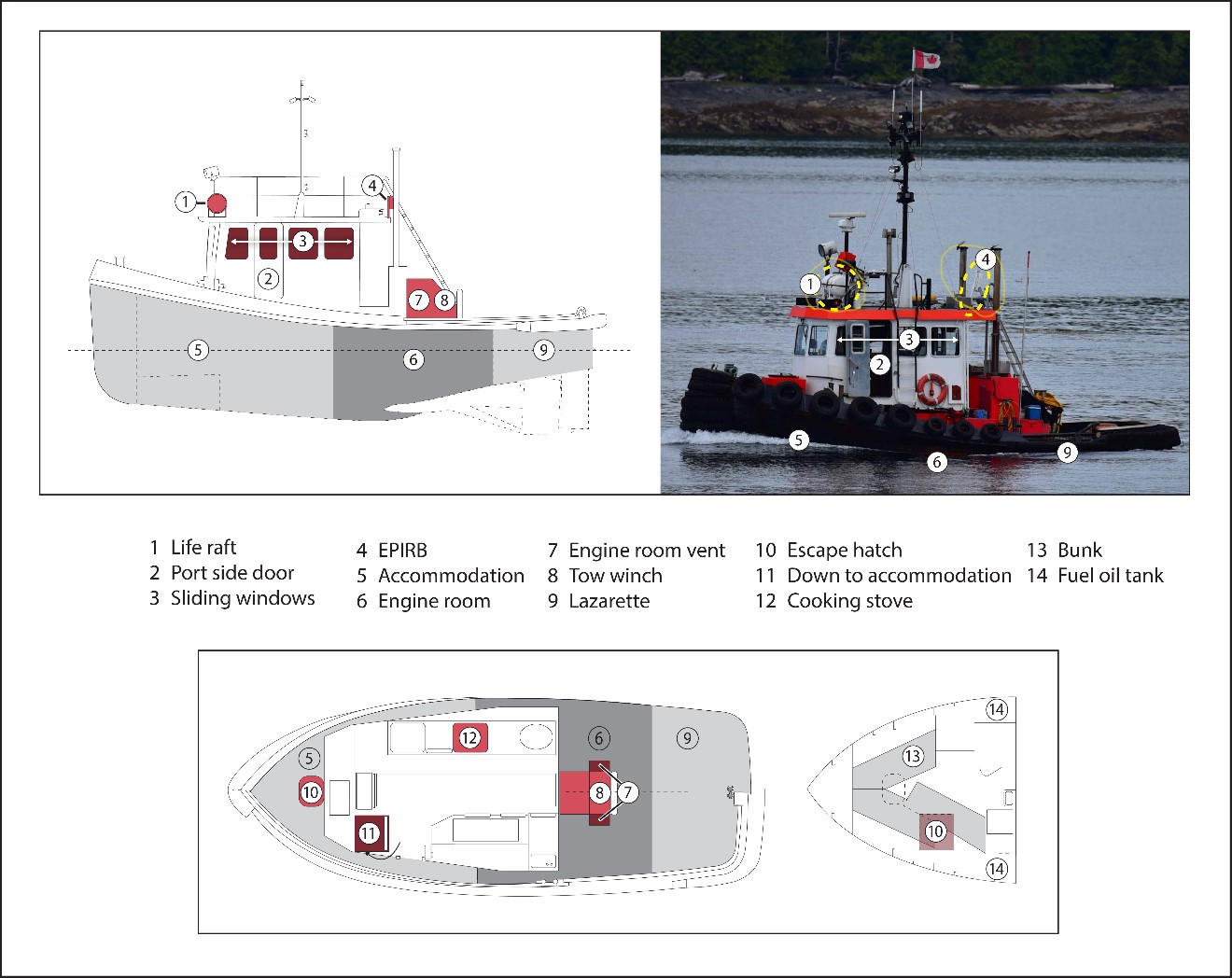
The wheelhouse was housed in an aluminum superstructureFootnote 1 and was flush with the deck. The wheelhouse had 2 weathertight exterior doors: 1 on the port side and 1 aft. There were sliding windows on the sides of the wheelhouse and 1 in the aft door. One of the starboard windows was normally left partly open to provide ventilation for a cooking stove located in the wheelhouse.
The wheelhouse was equipped with main engine and propulsion controls, an autopilot, a radar, a global positioning system, a very high frequency radiotelephone with digital selective calling (VHF-DSC), 2 electronic chart display units, and a Class BFootnote 2 automatic identification system (AIS). The wheelhouse also contained an engine room alarm panel.
There was another conning position on top of the wheelhouse. A 4-person life raft and a Category 1 emergency position-indicating radio beacon (EPIRB) were stored on top of the wheelhouse, with the life raft forward and the EPIRB aft on the port side. Both the EPIRB and the life raft had hydrostatic release units (HRU). HRUs are designed to automatically activate by water pressure when submerged and release the lifesaving equipment so that it floats free.
The accommodation, located in the forecastle, could be accessed via a ladder that led down from a watertight hatch in the wheelhouse. The accommodation also had an escape hatch with a coaming that exited onto the deck forward of the wheelhouse. There were 3 bunks inside the accommodation: 2 on the starboard side and 1 on the port side.
The engine room was accessed from the deck through a rectangular hatch with a coaming. The hatch cover had 2 slots cut in it, and plexiglass had been bolted over the slots to serve as a skylight. The engine room had a forced ventilation system as well as exhaust vents located on the aft side of the wheelhouse (Figure 2). The dampers for the exhaust vents were located beside their respective vents. To close the exhaust vents, the dampers had to be manually placed over the vents and secured.Footnote 3 The lower edge of the exhaust vents were about 1 m from the deck. When deck openings were secured, the open exhaust vents were the lowest downflooding point on the tug.

The Ingenika had a single-drum electro-hydraulic towing winch aft of the wheelhouse. The winch was fitted with a 350 m steel cable towline that was approximately 22 mm in diameter. There were 3 locations on the tug from which the winch brake could be released to abort the tow or pay out the towline: locally at the winch, from inside the wheelhouse, or from the top of the wheelhouse. The tug had manual towing pins that could be fitted to the transom. These were not in use at the time of the occurrence.
The vessel had undergone a midlife upgrade between July 2019 and May 2020, at which time both main engines were replaced.Footnote 4 The new main engines were connected to existing gearboxes. The batteries were also replaced and the electrical system was upgraded. The batteries were located in the engine room in covered and vented boxes. They provided power for the vessel’s floodlight, the AIS, and the VHF radiotelephone.
1.2.2 Miller 204
The Miller 204 (Figure 3) is a deck cargo barge of welded steel construction. It has a raked bow and stern, round bilges leading to a flat bottom, and 2 skegs located aft. The barge has a hinged stern ramp and double bitts located forward and aft on the port and starboard sides of the deck, allowing the barge to be towed from either end.

1.3 History of the voyage
On 10 February 2021, the Ingenika was scheduled to tow the Miller 204 from Kitimat, British Columbia (BC), to Kemano, BC. The Miller 204 was chartered to a contractor in Kemano who was using the barge to transport construction equipment and supplies.
Around 0800Footnote 5 on 10 February, the master and deckhand 1 (DH1) met in Prince Rupert, BC, and made the approximately 2-hour trip by car to Kitimat, where the Ingenika was docked. Deckhand 2 (DH2) joined them in Kitimat, having travelled from Terrace, BC, a trip of approximately 1 hour by car.
The crew boarded the Ingenika around noon. DH2, who was making his first trip on the Ingenika, accompanied DH1 as DH1 performed pre-departure checks. DH1 completed the tasks listed on the pre-departure checklist, which included disconnecting the electrical shore connection and visually checking the engine room and lazarette, including the bilges. Finding no issues, he started the main engines.
At 1504, the Ingenika proceeded to the loading grounds. The Ingenika’s towline was connected to the bitts on the Miller 204’s stern using synthetic rope bridles, and loading began. While the barge was being loaded, the master of the Ingenika discussed the inclement weather with the owner/master of another tug company. The master of the Ingenika also checked the weather forecast on his cellphone using the weather app Windy.Footnote 6 The Ingenika’s VHF radiotelephone was set to the channel that broadcasts the Environment Canada marine weather forecast.
At 1505, the master called the Wainwright Marine Services office from his cellphone, but there was no answer. At 1510, the owner of Wainwright Marine Services called the master’s cellphone and had a conversation with the master that lasted 2 minutes. During the conversation, weather was discussed, as well as a previous trip when another company tug, the Cadal,Footnote 7 had been used to tow the Miller 204 in adverse weather conditions. At 1513, the master also called home.
By 1537, loading of the barge was completed. The barge was carrying several trailers containing heavy equipment and cement powder in bulk, vehicles with an estimated 1100 L of diesel fuel, 6.5 tonnes of sulfuric acid in 3 tank trailers, and 3 semi-trailers with food for Kemano. The barge’s mean draft was estimated to be 0.9 m, and its displacement was estimated to be 2300 tonnes.Footnote 8
Soon after, the Ingenika departed Kitimat with the Miller 204 in tow. The master advised Marine Communication and Traffic Services (MCTS) in Prince Rupert accordingly. About 305 m of towline was paid out upon departure.
After departure, the master and the 2 deckhands remained in the wheelhouse. The tug was on autopilotFootnote 9 on a south-southwesterly course, and the master gradually increased the speed to 8.9 knots. The master then handed over the navigational watch to DH2 while DH1 supervised DH2. While DH2 had the watch, DH1 familiarized him with the navigation, communication, and safety equipment that was in the wheelhouse.
At approximately 1620, when the tug was adjacent to Coste Island (Figure 4), cellphone coverage was lost.Footnote 10 At this time, the waves were approximately 1 m and moving southerly, in the same direction as the tug. The master used the VHF radiotelephone to inform MCTS that the vessel was expected to be at Staniforth Point (Figure 4) around 1930. Soon after the call, the master retired to his bunk in the accommodation.

Around 1900, the master returned to the wheelhouse and had dinner. After dinner, the master and DH2 took over the watch while DH1 had dinner. The tug’s speed at this time was 7.3 knots, and the sea conditions remained unchanged from those observed earlier in the voyage.
At 1915, the master notified MCTS that the Ingenika had reached Staniforth Point and was checking out.Footnote 11 The tug was on a south-southeasterly course at a speed of 5.8 knots. At 1919, the master called the Wainwright Marine Services office using a satellite phone. The office number was routed to dispatch for the evening, which was being covered by the owner. The master informed the owner that the tug and barge were on track to reach Kemano as scheduled and that the weather conditions were acceptable. The tug was on a south-southeasterly course at a speed of 6 knots. After dinner, DH1 retired to the accommodation and lay down on the starboard bunk to rest. At this time, the tug had started bucking in the waves.
As the tug proceeded past Rix Island, its speed began to fluctuate and decrease. At 2152, as the tug and barge were rounding Europa Point, the tug’s speed dropped to below 1 knot (Figure 4, 1st drop in speed). The tug regained some speed, but at 2213, it dropped below 1 knot again (Figure 4, 2nd drop in speed). The tug then proceeded on an east-northeasterly course with the speed continuing to fluctuate between 0.6 and 3.1 knots.
At some point, there was a loud bang and DH1, who was resting in the bunk, was suddenly thrown against the starboard side of the hull. When he stood up, he had to balance himself because the tug was heeled over to starboard by approximately 30°. Soon after, DH2 opened up the hatch cover leading to the accommodation (Figure 5) and asked DH1 to pass him the immersion suits.

DH1 retrieved 3 immersion suits from a locker in the accommodation and passed them up to DH2 one at a time due to their bulkiness. DH1, attired in pyjama pants and a long-sleeve shirt, left the accommodation and climbed up the ladder to the wheelhouse. The ladder was at an angle because of the vessel’s starboard heel. As DH1 was climbing up the ladder, the master was making a Mayday call using the VHF radiotelephone and donning an immersion suit. DH2 was also donning an immersion suit. The tug’s engines were no longer running.Footnote 12 The last AIS transmission from the tug was logged at 2311:27. At this time, the Ingenika was in Europa Reach at position 53°25.89′ N, 128°29.4′ W, approximately 16 nautical miles (NM) from Kemano (Figure 4).
When DH1 reached the wheelhouse, the stern and the starboard side of the deck were awash. Shortly after, water began to enter the wheelhouse. As water entered the wheelhouse, the bag containing DH1’s immersion suit floated to the starboard side of the wheelhouse.
DH1 retrieved his immersion suit, at which point water had reached the level of the port-side door sill. Soon after, the master ordered the crew to abandon ship. Without time to don his immersion suit, DH1 opened the port-side door, stepped into the water, and swam away from the vessel. The master and DH2 followed DH1 and swam a short distance to where DH1 was, not far from the tug. At this time, the barge was not visible anywhere near the crew on the port side of the tug.
The master and DH2 floated on their backs in their immersion suits. DH1 briefly held on to DH2 and told him that he was holding on because he was not wearing a flotation device. DH2 acknowledged him.
As the tug continued to sink by the stern, the top of the wheelhouse became flush with the water. DH1 let go of DH2 and swam 5 to 10 m toward the life raft, which was still attached to the vessel. He tried to undo the straps securing the life raft to its cradle, but the straps were frozen and had ice built up on them. DH1 swam back to the master and DH2. He hung on to the master and explained that he did not have a flotation device. The master acknowledged him. DH2 began to drift away from the master and DH1.
Soon after the tug sank, the HRU on the life raft activated. The life raft deployed and inflated about 20 seconds later. It floated about 20 m from DH1 and the master. DH1 swam toward the life raft and reached it after a few minutes. The master yelled out to DH1 as DH1 boarded the life raft. DH1 called the master and DH2 to join him, but they did not respond. DH1 periodically activated the life raft’s flares to signal for help. After drifting for approximately 30 to 40 minutes, the life raft reached the shoreline. DH1 went ashore to seek shelter in the forest.
1.3.1 Search and rescue
On 10 February at 2343, the Joint Rescue Coordination Centre (JRCC) in Victoria received an EPIRB activation signal from 53°25.8′ N, 128°29.5′ W, approximately 0.1 NM south-southwest from the Ingenika’s last AIS signal. JRCC identified the EPIRB signal as coming from the Ingenika and relayed this information to MCTS. MCTS then made multiple attempts to contact the vessel, but did not receive a response. JRCC tasked search and rescue (SAR) resources to proceed to Europa Reach.
At 0250, SAR resources arrived in Europa Reach and began searching the area. At 0327, they located the Miller 204. It was aground about 4 NM west-southwest of Europa Reach. The towline was still attached to the barge but was trailing loose into the water and was no longer attached to the tug. Most of the cargo on the barge had shifted to the starboard side.
By 0858, SAR resources had found the bodies of DH2 and the master. DH2’s body was found approximately 3 NM west of Europa Reach, and the master’s body was found on the east side of Rix Island. Near Rix Island, SAR resources also found a life buoy, 2 standard lifejackets, and an inflatable lifejacket. The tug’s EPIRB was located near the barge’s grounded position.
At 0904, SAR resources located DH1 and the life raft on land, about 1 NM west of the tug’s last AIS position. DH1 was transported to emergency health services in Kitimat, where he was hospitalized and treated for hypothermia and frostbite.
On 15 February, the barge floated free on a high tide. The towline was cut and the barge was towed to Prince Rupert. Subsequent examination of the towline by the TSB determined that it had slight damage and kinks but showed no signs of having parted under tension.
The water at the area of the occurrence was approximately 200 m deep. Despite efforts by various federal agencies following the occurrence, the Ingenika was not located.
1.4 Previous voyages
The occurrence voyage was the 4th trip in February as part of the same charter, with the Ingenika and Miller 204 having already made voyages on 01, 03, and 05 February (Table 2). The occurrence master was also the master for these 3 prior voyages. The Ingenika’s average transit time from Kitimat to Kemano on these prior voyages towing the Miller 204 had been approximately 10 hours. The tug was usually on autopilot for the duration of the voyage. Loading of the barge was done at the discretion of the contractor based on operational requirements. The weights loaded on the barge on previous voyages had varied.
| Date | Transit speed at Staniforth Point (knots) | Transit speed at Shearwater Hot Spring Conservancy (knots) | Transit speed at location of 1st speed reduction on 10 Feb (knots) | Transit speed at location of 2nd speed reduction on 10 Feb (knots) | Transit speed at location at which AIS signal was lost on 10 Feb (knots) | Forecast wind speed (knots) and direction |
|---|---|---|---|---|---|---|
| 2021-02-01 | 6.3 | 5.3 | 4.9 | 4.3 | 5.1 | 15-25 NE |
| 2021-02-03 | 4.8 | 5.3 | 5.8 | 5.2 | 5.3 | 10-20 NE |
| 2021-02-05 | 6.3 | 7 | 6.6 | 6.7 | 6.5 | 15 NW |
| 2021-02-10 (occurrence voyage) | 5.83 | 1.75 | 0.97 | 0.39 | 1.55 | 35-45 NE |
The route followed on the occurrence voyage was similar to the route followed on previous voyages (Figure 6).

On previous occasions, especially in rough weather, the barge had slowed down the speed of the Ingenika. At these times, the towline had sometimes deviated from the centreline of the tug, especially when the tug and barge were making a turn. When this happened, the crew usually manoeuvred the tug so that the barge was behind it. There had also been times when the crew had taken the vessel out of autopilot and put it on hand steering to reduce yawing of the tug. Occasionally, the towline was also paid out to maintain control of the barge.
1.5 Injuries and fatalities
The cause of death for the master and DH2 was drowning. DH1 was treated in hospital for hypothermia and frostbite.
1.6 Damage to the vessels
The Ingenika sank and could not be located. The Miller 204 sustained damage to its hull sections as a result of pounding against the shoreline in the high winds.
1.7 Environmental conditions
Weather data for the specific area of the occurrence in Europa Reach is limited. Europa Reach is a natural fjord where there can be significant and rapid changes in conditions. The forecasts and conditions provided below are based on weather data collected from the nearest available locations.
On 10 February, the weather forecast for the Douglas Channel, issued at 0400 and continuing through to 2128, indicated gale force winds and freezing spray with northeasterly outflow winds of 35 to 45 knots. Periods of snow and temperatures falling to −7 °C were also forecast. The winds at Kemano Bay were forecast as northerly at 30 knots with gusts of up to 40 knots.
Between 0001 and 0250 on 11 February, the air temperature around Europa Point was −9° C with a windchill of −24. The winds were between 40 and 50 knots. There was freezing spray and 1 to 2 m waves that were approximately 3 m apart. The water temperature was approximately 5 °C. There was no ambient light, and the sky was clear with good visibility.
Low tide at Kemano Bay was 0.7 m at 1954 on 10 February, and high tide was 5.5 m at 0107 on 11 February. To estimate the current at the time and location of the occurrence, the TSB requested a simulation of oceanographic conditions from the Institute of Ocean Sciences at Fisheries and Oceans Canada. The simulation indicated that the magnitude of the current on the surface was 1 to 1.2 m/s and the magnitude of the current at a depth of 5 m was 0.9 to 1 m/s.
1.8 Vessel certification and inspection
The Ingenika, as a commercially operated vessel of 15 gross tonnage (GT) or less, was required to be registered with Transport Canada (TC) but was not required to have a certificate of inspection to operate, nor was it required to undergo periodic inspections by TC.
Under section 106 of the Canada Shipping Act, 2001 (CSA 2001), a vessel’s authorized representative (AR) is responsible for ensuring that the vessel complies with all applicable regulations. TC has the authority to randomly inspect any vessel for compliance with the CSA 2001 and its regulations.Footnote 13
The Ingenika was registered with TC. There were no records to indicate that TC had inspected the vessel in its over 50 years in operation. The Ingenika had not been formally assessed for stability or bollard pull. TC can request a stability assessment if TC is of the opinion that modifications made to a ship adversely affect its stability; however, TC had never required the Ingenika to undergo a stability assessment. A bollard pull assessment is not required by regulation (see Section 1.11.1 for information on bollard pull).
1.9 Company operations
The Ingenika and the Miller 204 were managed and operated by Wainwright Marine Services. Wainwright Marine Services is wholly owned by Bates Properties Ltd., which purchased Wainwright Marine Services from its former owner in July 2020. The Wainwright Marine Services office is located in Prince Rupert, and Bates Properties Ltd. operates out of Vancouver, BC.
At the time of the occurrence, Wainwright Marine Services was providing tug and barge charter services in northern BC and managed 6 tugs, including the Ingenika. Four of these 6 tugs were of 15 GT or less. Wainwright Marine Services was also managing 9 barges and 1 workboat. The tugs were typically operated 24 hours a day, 7 days a week, with a 3-person crew on a loose 2-week shift schedule. The same tugs were used for both coastal towing and river towing assignments. The management of safety and operations on the tugs was left to individual masters.
1.10 Personnel certification and experience
The master held a Master, Limited for a Vessel of Less than 60 GT certificate of competency issued in 2007 and had started working for Wainwright Marine Services as a deckhand in September 2017. After receiving on-the-job training, he was familiarized as master on the Ingenika in April 2019. From July 2019 to May 2020, when the Ingenika was undergoing a midlife upgrade, he worked as a deckhand on another company tug, the Cadal. On 09 June 2020, the master was given command of the Ingenika, and since that time, he had made approximately 22 trips as master on the Ingenika towing the Miller 204 between Kitimat and Kemano. The occurrence voyage was his 4th trip in February 2021.
The master had started working in the maritime industry in 1998 and the majority of his experience was on fishing vessels and passenger ferries. The master held a Restricted Operator Certificate – Maritime Commercial. He also had completed 3 Marine Emergency Duties (MED) courses. One of the MED courses was completed in 2006 (MED A2), and the other 2 were completed in 2010 (MED with respect to STCWFootnote 14 basic safety and MED proficiency in survival craft and rescue boats other than fast rescue boats).
DH1 had started his maritime career with Wainwright Marine Services on 08 January 2020. His 1st trip on the Ingenika was on 21 July 2020. In addition to working on the Ingenika, DH1 had also worked on other tugs and barges operated by Wainwright Marine Services. He held an MED A3 certificate and a Restricted Operator Certificate – Maritime. DH1 did not hold a certificate of competency.
DH2 had joined Wainwright Marine Services on 10 February 2021, and the occurrence voyage was his 1st trip with the company and 1st time on a tug. He had started working in the maritime industry in 2015, obtaining experience in the fishing industry from 2017 to 2019 and operating a Hurricane 753 rigid-hull inflatable boat for Fisheries and Oceans Canada in 2020. He held a Small Vessel Operator Proficiency certificate, an MED A3 certificate, and a Restricted Operator Certificate – Maritime. DH2 did not hold a certificate of competency.
1.11 Assessment of towing operations
There are a number of safety-related considerations that need to be assessed before undertaking a towing operation. Many of these considerations are outlined in the Small Vessel Compliance Program for Tugs (SVCP-T), a TC program introduced in January 2022 that is intended to assist owners of tugs of 15 GT or less to operate safely.Footnote 15 Enrollment in the SVCP-T is voluntary. The program covers many regulatory requirements that owners must meet. It also provides guidance to support safe towing operations and recommends that owners and ARs
- conduct a stability assessment and ensure that crew members understand the stability book and any stability limitations for operating the tug, including the effects of forces exerted by the towline on the tug’s stability;
- measure the tug’s bollard pull and use it to help establish the tug’s operational limits;
- ensure that crew members understand the tug’s operational limits and are supported in making decisions not to sail where the tug’s operational limits would be exceeded;
- ensure that crew members are sufficient in number, experience, and certification to safely undertake the intended voyage, keeping in mind that towing is a specialized skill that requires experience to obtain; and
- ensure that a passage plan and a tow plan is in place before every operation.Footnote 16
At the time of the occurrence, the SVCP-T was not in place. In 2006, a Canadian Marine Advisory Council working group was initiated to discuss a report produced by a tug and barge task force convened in 2004 following a fatal girding occurrence. Among other things, the working group recommended that bollard pull on tugs, which is used to determine suitability for operations such as barge towing, be calculated by a common method and officially recorded. The recommendation resulted in TC developing some guidance for bollard pull aimed at barges carrying oil or dangerous chemicals in bulk. The guidance was published in TP 11960, Standards for the Construction, Inspection, and Operation of Barges Carrying Oil or Dangerous Chemicals in Bulk. The recommendation was not implemented for tugs engaged in other types of towing operations.
For other types of towing operations, TC has provided TP 15180, Guidelines for the Construction, Inspection, Certification, and Operation of Tugs < 24 Metres in Length. This document references International Maritime Organization (IMO) and classification society guidelines for towing operations (e.g., IMO’s Guidelines for Safe Ocean Towing and GL-Noble Denton’s Guidelines for the Approval of Towing Vessels). Paragraph 1.5.3 of this document refers to TP 11960 as additional guidance for determining whether the tug is of the appropriate size and power to tow the desired load.
TC has also published Ship Safety Bulletin 16/2020, Hazards and Risks of Girding During Towing Operations, which contains guidance on planning a tow and specifically notes that the plan should consider the tug’s capability in terms of both horsepower and bollard pull.
1.11.1 Bollard pull
Bollard pull is a measure of a tug’s towing capacity and is defined as the thrust developed by a vessel’s propulsion system when it has no speed in the forward direction. Calculating a tug’s bollard pull provides a data point to help owners and operators assess a tug’s operational limitations. However, a bollard pull calculation alone is not enough to make an accurate assessment of a tug’s operational limits for a given towing operation. A tug’s size, hull design, freeboard, horsepower, manoeuvrability, visibility from the wheelhouse, and towing equipment are also considerations in determining operational limits, as well as the towed object’s size, freeboard, windage, and any deck structures such as cargo and ramps. Environmental forces must also be considered, including wind speed, wave height, and current speed. Environmental information should be obtained for the specific time of the year when the tow is expected to take place. For example, if the towing operation is being carried out in February, then environmental data from December to May should be referenced. The most extreme values for the period should be used when calculating bollard pull.
For towing operations of the type undertaken by the Ingenika, there is no regulatory requirement for the tug’s bollard pull to be ascertained, nor is there definitive guidance for determining the required bollard pull for any particular size of tow. The Ingenika’s bollard pull had not been calculated before the occurrence.
Using industry standards,Footnote 17 the TSB calculated that the Ingenika’s maximum bollard pull was likely around 8 tonnes.Footnote 18 When taking into account an efficiency factor of 80%,Footnote 19 the effective bollard pull of the tug was around 6 tonnes in calm waters (Figure 7). At the time of the occurrence, in the forecasted environment conditions, the bollard pull required for the Miller 204 to maintain headway was approximately 12 tonnes.

1.12 Safety culture
Safety culture is the way that safety is perceived, valued, prioritized, and managed throughout all levels of a company. It encompasses the attitudes, beliefs, perceptions, and values of all employees in an organization in relation to safety. One of the most important factors affecting safety culture is the company management’s degree of commitment to safety. It is vital that owners and operators actively demonstrate their commitment by providing leadership and resources to manage safety. For example, management should support employees in ensuring safe operations and reporting safety-related issues, and provide documented procedures. One way to encourage a good safety culture is to implement formal safety management processes; a safety management system (SMS) is a tool to help a company or vessel with these processes.
1.13 Safety management systems
Safety management involves individuals at all levels of an organization and requires that a systematic approach be taken in identifying and mitigating operational risks. An SMS is an internationally recognized framework that allows companies to identify hazards, manage risks, and make operations safer, ideally before an accident occurs. The principal objective of an SMS on board a vessel is to ensure safety at sea, prevent human injury or loss of life, and avoid damage to property and the environment.
Some elements of an effective SMS are:
- procedures and checklists for the vessel’s operations
- maintenance procedures for the vessel and its associated equipment
- documentation and record-keeping procedures
- procedures for identifying hazards and managing risks
- procedures to prepare for and respond to emergency situations
- drills, training, and familiarization for the vessel’s crew.
Currently, only Canadian vessels that operate on international voyages and are subject to Chapter IX of the International Convention for the Safety of Life at Sea must comply with the existing Safety Management Regulations. These regulations do not apply to the majority of domestic vessels.
TC has recently indicated that it is planning to expand the application of these regulations. Under the proposed Marine Safety Management System Regulations, Class IV vessels (which include tugs like the Ingenika) would be required to develop a documented SMS that names a ship managerFootnote 20 and submit their SMS to TC for approval. TC would then issue a Canadian safety management certificate if the SMS meets the requirements below. The ship manager would be required to review the SMS internally at intervals not exceeding 12 months. There would be no requirements for external audits.
A documented SMS would need to include
- a safety and environmental protection policy;
- instructions and procedures to ensure compliance with provisions of the CSA 2001 and its regulations respecting the safe operation of the vessel and the protection of the environment;
- defined levels of authority and lines of communication between, and among, shore-based and on-board personnel;
- procedures for reporting shipping casualties and non-compliance with the requirements of the SMS;
- procedures to prepare for and respond to emergency situations; and
- procedures for internal reviews of the SMS.
The instructions and procedures to ensure compliance with provisions of the CSA 2001 and its regulations must specifically address
- equipment inspection, maintenance, and testing;
- ensuring the vessel’s seaworthiness and stability;
- voyage planning, safe navigation, and handling of the vessel; and
- ensuring safety at sea and preventing human injuries, loss of life, and damage to the marine environment and to property.
The procedures required for preparing and responding to emergency situations must specifically address
- preparing for and responding to shipping casualties and personnel accidents;
- dealing with equipment failure;
- responding to pollution incidents; and
- reporting emergency situations.
TC published the proposed regulations in the Canada Gazette, Part I in June 2022 and expects to publish the final regulations in the Canada Gazette, Part II in April 2023.
Under the regulations in effect at the time of the occurrence, the Ingenika was not required to have an SMS.
1.14 Company safety management
Vessels that are not required to have an SMS are still obliged to comply with subsection 106(1) of the CSA 2001, which requires the AR to provide procedures for the safe operation of the vessel and for dealing with emergencies, and to ensure that the crew receive safety training.Footnote 21
1.14.1 Safe operating procedures and emergency procedures
In 2014, Wainwright Marine Services voluntarily developed an SMS manual. This manual contained safe operating procedures and emergency procedures. At the time of the occurrence, the SMS manual had last been updated in 2019. All of the SMS documentation was transferred to Bates Properties Ltd. when it purchased Wainwright Marine Services in July 2020.
When Wainwright Marine Services was operating under its former owner, the AR had assigned the masters of each vessel the responsibility to implement the organization’s procedures on board. However, the extent to which the voluntary SMS was implemented under the former Wainwright Marine Services owner was unclear as there was no supervision process to validate whether the SMS was being implemented on vessels. At the time of the occurrence, Bates Properties Ltd. had not yet reviewed all of the SMS documentation that it had received when it purchased Wainwright Marine Services.
The SMS manual contained 3 documents that the masters routinely used during towing operations:
- a pre-departure checklist
- a passage plan / tow plan check sheet
- a tug and barge trip sheet
The pre-departure checklist prompted the crew to check all operational equipment, such as bridge and engine controls and navigational equipment. The passage plan/tow plan check sheet prompted the crew to enter the waypoints for the voyage and make note of any hazards (e.g., bridges, traffic, or other restrictions). The tug and barge trip sheet prompted the crew to keep track of what freight was being transported for each chartered customer. After a completed shift, copies of these 3 documents were usually handed over to Wainwright Marine Services or left on board for company personnel to collect.
The SMS manual also contained written procedures for the safe operation of the vessels and for dealing with emergencies such as fire, abandoning ship, grounding, a person overboard, collision, propulsion failure, and girding. Finally, the SMS manual covered topics such as towing and yarding of barges, hours of work and rest, safety meetings and drill reports, a captain’s review, hiring and training of employees, and operations.
The investigation determined that there were inconsistencies in the ways that different masters filled out the pre-departure checklists, passage plan/tow plan check sheets, and tug and barge trip sheets, with some masters not filling out certain sections of the documents.
There were no procedures or guidance in the SMS about operating limits with respect to weather, and the masters were left to monitor the marine weather forecasts in advance of any trip and decide whether to go or not. The masters normally communicated concerns or noteworthy observations about the weather and the timing of a trip to Wainwright Marine Services dispatch.
1.14.2 Familiarization
At the time of the occurrence, the AR was required to provide the master with written instructions for familiarizing crew members with shipboard equipment, operational instructions, and their assigned duties. Footnote 22 The SMS manual had a universally applicable familiarization checklist that prompted crew members to be familiarized with the location and operation of safety equipment, including the life raft, rescue boat, immersion suits, and first aid kits.
The master had initially completed the familiarization checklist in April 2017 when he had worked as a deckhand. He completed the same familiarization checklist a second time on 30 April 2019 when he became master of the Ingenika. DH1 had completed the familiarization checklist in July 2020.
Because the occurrence trip was DH2’s 1st voyage with this company, it was intended to be the trip on which he completed his familiarization checklist. Prior to the occurrence, DH2 was familiarized with engine room details specific to the tug and the location of the lifejackets and immersion suits. During the occurrence voyage, DH1 had familiarized him with the navigation, communication, and safety equipment that was in the wheelhouse.
As part of their familiarization, the crew had been shown the location of the immersion suits, but they had not practised donning them.
1.14.3 Drills
At the time of the occurrence, the AR was required to ensure that procedures were established for the use of lifesaving equipment and fire extinguishing equipment in the event of an emergency and that the crew practised the procedures in order to be proficient at carrying them out at any time. Footnote 23
The SMS manual contained drill reports. The reports provided suggestions for different types of drills and required the type of drill being conducted to be identified. The reports also required the actions taken during a drill and any lessons learned to be noted. The form had a line for the office to indicate who had received the drill report and on what date.
There was no formal drill schedule set out by Wainwright Marine Services, and masters were left to use their discretion with regard to if, when, or how drills were carried out. It was not the practice for drills to be carried out on the Ingenika.
1.14.4 Inspections of on-board equipment
The Ingenika had a computer-based planned maintenance system that was programmed with the dates that certain on-board equipment inspections were to be carried out. The system was not used consistently and was not up to date at the time of the occurrence. A log generated by the company on 18 February 2021 showed the following inspection frequency and last inspected dates for items relevant to this occurrence (Table 3).
| Item | Inspection frequency | Last inspected |
|---|---|---|
| Inspect immersion suits | Once a year | 01 January 2020 |
| Check towing pins | Once a month | 31 May 2020 |
| Inspect lifejackets and personal flotation devices | Every 6 months | 01 January 2020 |
| Inspect EPIRB | Once a year | 14 June 2019 |
| Replace batteries in survival suits | Once a year | 11 April 2018 |
| Inspect seals for watertight doors | Once a month | 14 June 2019 |
1.14.5 Crewing and certification
At the time of the occurrence, TC required the AR to ensure that a vessel was crewed in accordance with the requirements of the Marine Personnel Regulations. Footnote 24 This involved ensuring that the master and crew had the certification necessary to operate the vessel.
Under the Marine Personnel Regulations, the Ingenika was required to be crewed with a master holding at least a Master, Limited for a Vessel of Less than 60 GT certificate of competency that was applicable to the type of vessel and its area of operations, and at least 1 other crew member. Any person left in charge of the deck watch was required to hold a certificate of competency.
In this occurrence, the master held a Master, Limited for a Vessel of Less than 60 GT certificate of competency, but it was valid only for vessels operated by Metlakatla Ferry Service Ltd. operating between Prince Rupert and Metlakatla, Alaska, United States, and not more than 25 NM from shore. From 2009 to 2017, the master had worked for the Metlakatla Ferry Service Ltd. operating the Koprino Wind, a passenger ferry of 24.05 GT, on a route between Prince Rupert and Metlakatla. The crossing time for this route is approximately 15 minutes one way. The master’s certificate was not valid for operating a tug. Neither deckhand held a certificate of competency.
1.14.6 Vessel safety equipment
The Ingenika carried the required vessel safety equipment, including 2 life rings stowed on either side of the wheelhouse, a fire hose, fire extinguishers, a life raft, 3 lifejackets, 3 immersion suits, emergency flares, and an EPIRB.
1.14.6.1 Immersion suits
Immersion suits are designed to keep a person buoyant, warm, and dry. They can reduce the effects of cold water shock, delay the onset of cold incapacitation and hypothermia, and prevent drowning. They also make people more visible in the water, which aids with rescue.
At the time of the occurrence, the Ingenika was carrying 3 immersion suits. The suit that the master was found in was an adult size suit manufactured in 1997. Footnote 25 It had an inflatable head support with an inflation hose, a neoprene hood, gloves stowed in the sleeves, wrist seals, ankle straps, built-in non-slip boots, and a rescue whistle. The suit that DH2 was found in was an adult size suit manufactured in 2017. It had built-in gloves and booties, ankle straps, a harness to assist with retrieval from the water, an inflation hose, a rescue whistle, and a strobe light. The size of the 3rd suit on the Ingenika was unknown.
To don an immersion suit effectively, the user needs to pull on the suit as they would a pair of coveralls, don the hood, and then zip up the suit all the way to prevent water from getting in. The hood must be donned before the suit is zipped up, because momentum is required to secure the zipper and this is achievable only with the hood donned and the left and right sides of the suit pulled together. If the suit has ankle and wrist straps, these need to be secured. If the suit has separate gloves, for example tucked into the bottom of the sleeves, these need to be donned to maintain a seal and to reduce the effects of cold water shock. If the suit has an inflatable head support, the user should inflate the head support to maintain the ideal flotation angle.
Because the zipper must be fully secured before the user enters the water, manufacturers frequently place warnings in their guidance documentation. For example, the guidance document for the master’s immersion suit warns that failure to completely close the waterproof zipper will result in water leaking into the suit and reduce in-water survival time. The warning directs users to double-check the zipper to ensure that it is completely closed against its sealing plug.
In 2000, TC issued a Ship Safety Bulletin stating that drills afford an opportunity for crew to practise donning their immersion suits, to ensure that they are of an appropriate size, and to ensure that the zippers are properly lubricated. Footnote 26 Through drills, crew members can also check their suits for any potential areas of damage and familiarize themselves with key steps for donning the suits, such as ensuring it is fully zipped up. Immersion suit zippers, even when lubricated, are naturally difficult to zip up because the zipper has some inherent resistance and, depending on the size of the person, the fabric may need to be held together in order to facilitate closing the zipper. In 2019, TC also issued a Ship Safety Bulletin on safety measures concerning lifesaving appliances, which discussed the importance of crew members trying on their immersion suits before departure to ensure correct fit. Footnote 27
The company SMS required the immersion suits to be inspected annually. The manufacturer of the immersion suits recommended that the zippers be tested and lubricated to ensure they were working properly. The investigation found that the immersion suits on board the Ingenika had not been routinely maintained, which involves lubricating the zippers.
When SAR responders recovered the bodies of the master and DH2, they found that both of their suits were partially zipped up and their hoods were not donned. The inflatable head supports were uninflated, and the suits were saturated internally with water and ice. The gloves for the master’s suit were found stowed in the sleeves.
1.14.6.2 Emergency position-indicating radio beacon
EPIRBs are designed to alert SAR authorities in the event of an emergency. Some EPIRBs are fitted with HRUs that allow the EPIRB to float free of a vessel and automatically transmit a distress signal when submerged. The activation of an EPIRB with an HRU is dependent on the vessel sinking to a certain depth. Once an EPIRB activates, it transmits a signal to SAR resources. The signal allows SAR resources to target the specific location of the EPIRB, which can expedite rescue.
At the time of the occurrence, TC required vessels of less than 12 m in length on inland waters or Class 2 near coastal voyages to carry a float-free or manually activated EPIRB, or a personal locator beacon (PLB). Footnote 28 Through the SVCP-T, TC also recommends that ARs and owners ensure that emergency equipment is available and properly maintained. TC points out that EPIRBs must be registered properly, as this facilitates the task of the SAR authorities in an emergency and helps eliminate false alarms.
EPIRBs that have up-to-date registration information can make it easier for SAR personnel to access useful data about vessels in a distress situation: for example, what type of vessel to search for, how many people need assistance, what type of help might be needed, and how to contact the owner.
The Ingenika had a Category 1 float-free EPIRB with an HRU, as required by regulation. The HRU was designed to automatically activate when submerged in 1.5 to 4 m of water. During the occurrence, the EPIRB automatically deployed and floated free, as designed. The EPIRB was registered to the Ingenika, but the registration information had not been updated and was still that of the former owner. This led to a delay of approximately 35 minutes in SAR resources being able to contact the current owner of the Ingenika. The delay did not affect the timing of the SAR response, however, as SAR resources were tasked shortly after the EPIRB signal was received.
Finding: Other
The registration information for the Ingenika’s EPIRB was not up to date, which meant that SAR resources were not able to immediately contact the tug’s current owner.
1.15 Personal locator beacons
PLBs are portable units that can transmit a distress signal in much the same way as EPIRBs. PLBs are designed to be carried or worn by individuals and must be registered for the unit to provide vital personal information (name, address, emergency contact phone numbers, and medical conditions). PLBs are manually activated and operate on 406 MHz with a built-in low-power homing beacon that transmits on 121.5 MHz. PLBs also have an integrated GPS unit, which gives them the capability to transmit specific location coordinates when a distress signal is sent. A PLB with a strobe light can further aid rescuers when they search.
Although PLBs can improve one’s chances of survival in the event of an emergency, there are currently no regulations requiring crew members to carry them. Some safety associations across Canada are promoting their use, especially in the fishing industry, where crew members are at increased risk of falling overboard or experiencing a sudden capsizing.
1.16 Cold water immersion
Entering cold water, especially water below 15 °C, may trigger an initial cold water shock response, which causes the person in the water to gasp for air. Wearing an immersion suit, a personal flotation device, or lifejacket may prevent drowning during initial cold water shock by keeping a person’s mouth away from the surface of the water, preventing water ingestion.
Cold water shock is followed by cold incapacitation, which reduces the ability to swim. Hypothermia can occur quickly depending on water temperature; activities such as swimming or trying to board a life raft increase heat loss and speed up the onset of hypothermia. This can lead to further incapacitation and death if the person is not rescued. While a person in the water waits for rescue, protection from the elements is essential to survival (Table 4).
| Stage of immersion/rescue | Life raft | Immersion suit | Lifejacket/personal flotation device | No equipment |
|---|---|---|---|---|
| Cold water entry | Reduced or no exposure time in water | Enters water | Enters water | Enters water |
| Initial cold water shock | Prevents or reduces cold water shock response | Prevents onset of cold water shock response and keeps people afloat | Keeps head and mouth above surface when gasping | Gasping, water intake, cardiac response |
| Psychological response | Reduces threat to life, potentially reducing stress response | Reduces threat to life, potentially reducing stress response | Some reduction in threat to life, may reduce stress response | Immediate threat to life, stress exacerbates cold water shock response |
| Cold water incapacitation | Prevents or reduces cold effects | Delays onset of cold effects | Keeps people afloat after loss of swimming ability and dexterity | Erratic breathing, loss of swimming ability, shivering |
| Hypothermia | May significantly delay effects if people remain dry | May significantly delay effects if people remain dry | Hypothermia onset – reduced chance of survival | Hypothermia onset – unlikely to survive |
| Rescue from distress signal* | Likely to survive | Likely to survive | Reduced chance of survival | Unlikely to survive |
* Signal may include radio communications sent during emergency preparations, PLBs, or hand-held or float-free EPIRBs.
1.17 Regulatory oversight of tugs
At the time of the occurrence, in Canada, tugs of 15 GT or less were not required to be inspected and certified by TC under the Hull Inspection Regulations or the Vessel Certificates Regulations. Footnote 29 Consequently, these tugs were not subject to any limitations on voyages, on the type of activity for which they were used (e.g., towing), or on the conditions in which they were operating (e.g., weather). Moreover, although TC marine safety inspectors had the authority to conduct risk-based monitoring inspections to verify compliance with the CSA 2001 and associated regulations, there were no specific provisions in these regulations for the application of voyage limitations to these tugs.
At September 2022, there were approximately 1343 steel-hulled tugs of 15 GT or less registered in Canada, with approximately 1035 of these in BC. These tugs are not part of a structured inspection cycle, although TC has inspected a few of them following reported occurrences and has recently set an annual target of inspecting 3% of tugs of 15 GT or less nationwide. TC has also inspected some of them during concentrated inspection campaigns, which are targeted at specific safety concerns and tend to encompass a variety of vessels, including tugs, that are selected on a risk basis and in consideration of the campaign objectives.
In comparison, at September 2022, there were approximately 494 tugs of greater than 15 GT registered in Canada, with approximately 240 of these in BC. These tugs are required to be inspected before being certified and then again periodically by TC under the Vessel Safety Certificates Regulations. Inspections include boarding the tug to validate lifesaving appliances and emergency procedures and drills. Inspections also involve observing an emergency drill. As part of the inspection process, tugs of greater than 15 GT are issued voyage limitations and/or limitations with respect to the weather conditions and/or type of activity (e.g., towing) for which the vessel is used. Tugs of greater than 15 GT are also provided guidance regarding crewing levels in the form of a safe manning document.
From April to October 2022, TC conducted 30 risk-based monitoring inspections of tugs of 15 GT or less. Overall, 21 of these inspections resulted in a total of 62 deficiencies, including 13 related to lifesaving equipment, 12 related to structure or stability, 8 related to crew certificates, 6 related to fire safety, and 5 related to navigation safety.
From April to October 2022, TC also conducted 120 statutory inspections of tugs of greater than 15 GT. Sixty-four of these inspections resulted in the identification of deficiencies. In addition, TC conducted 30 risk-based monitoring inspections of tugs of greater than 15 GT on the basis of findings from the statutory inspections. Of these 30 risk-based monitoring inspections, 19 resulted in the identification of deficiencies.
In 2018–19, TC conducted a concentrated inspection campaign on domestic vessels. According to the campaign report, Footnote 30 83 vessels were inspected nationwide, 49 of which were inspected under the annual inspection category and 34 through quadrennial inspections per the Hull Inspection Regulations. Footnote 31 Nineteen of the vessels inspected were tugs, but none were of 15 GT or less. The data showed that vessels inspected every 4 years had more deficiencies than those inspected annually.
TC also focused on tugs in a concentrated inspection campaign conducted in BC from January to March 2017. Thirty tugs of 15 GT or less and 30 tugs of greater than 15 GT were selected for inspection. TC concluded that tugs of 15 GT or less had significantly more instances of regulatory non-compliance than tugs of greater than 15 GT. Footnote 32
1.17.1 Certification requirements for masters of tugs of 15 gross tonnage or less
At the time of the occurrence, to operate a tug of 15 GT or less, a person was required to hold a Master, Limited for a Vessel of Less than 60 GT certificate of competency. Footnote 33 This certificate was achieved by acquiring relevant experience on the type of vessel for which the certificate was sought and by acquiring the appropriate MEDs. Footnote 34
Candidates seeking a Master, Limited for a Vessel of Less than 60 GT certificate of competency were required to pass a written and oral examination as set out in The Examination and Certification of Seafarers. Footnote 35 These examinations required candidates to demonstrate, among other things, a good knowledge of the area for which the certificate would be valid, a basic knowledge of stability and its application, and the ability to deal with emergency situations (collision, grounding, flooding, fire, etc.).
For candidates intending to carry out towing operations, their knowledge, understanding, and proficiency for towing operations were also tested. Topics examined included
- cables used for towing and their required length
- the towing point
- the effect of the towing cable on the centre of gravity of the tug and on its stability
- events that may result in the capsizing of the tug
- tow abort systems
No formal training courses specific to towing operations were required in order to obtain a Master, Limited for a Vessel of Less than 60 GT certificate of competency valid for towing operations. As well, there was no requirement for recurrent MED training for crew members who sail on vessels engaged on near coastal or sheltered water voyages. Footnote 36
1.18 Coastal pilotage waivers
The Pacific Pilotage Authority (PPA) is a Crown corporation that was created in 1972 under the Pilotage Act. The PPA has a mandate to establish, operate, maintain, and administer safe and efficient pilotage services in the coastal waters of BC, including the Fraser River. Pilotage services are provided by licensed pilots, who are highly trained navigators that use their knowledge of local waters to direct a vessel and navigate it using the safest route. These routes can change daily depending on factors like other marine traffic, wind, and tides.
At the time of the occurrence, the PPA had the authority to, among other things,
- establish compulsory pilotage areas,
- determine which vessels are subject to compulsory pilotage, and
- prescribe the circumstances under which compulsory pilotage may be waived.Footnote 37
The PPA had implemented a process through which some vessels, mainly tugs and barges,Footnote 38 could obtain pilotage waivers, making these vessels exempt from compulsory pilotage in designated pilotage areas (Appendix B), if the operators met certain requirements. Under these requirements, every person in charge of a deck watch
(a) holds the certificates that are required by Part 2 of the Marine Personnel Regulations or, if the ship is not Canadian, equivalent certificates;
(b) has completed, as a person in charge of the deck watch on voyages in the region, at least
(i) 150 days of service in the preceding 18 months, or
(ii) 365 days of service in the preceding 60 months, including at least 60 days in the preceding 24 months; and
(c) has served as a person in charge of the deck watch in the compulsory pilotage area for which the waiver is sought on at least one occasion within the preceding 24 months.Footnote 39
In addition, vessels were required to
- be operating with a bridge navigational watch alarm system;
- be fitted with, and transmitting on, a Class A AIS; and
- have 2 persons on the bridge when operating in confined watersFootnote 40 or in conditions of restricted visibility or in hours of darkness.
Under the PPA’s waiver system, an acceptable standard of care had to be maintained by the waivered company, vessel, and crew, such that the risk to life, property and the environment was not substantially greater than would be anticipated if the vessel were under a pilot’s direction.Footnote 41
Before issuing a waiver, the PPA requested that the AR provide a signed statement of compliance for each watchkeeper’s sea time. The PPA recorded the information supplied by ARs but did not verify its accuracy.
For vessels berthing at terminals at various locations in BC, the PPA provided guidance regarding the minimum size (bollard pull) and number of tugs to be used. There was no such guidance for tugs that were approved within the PPA’s waiver system that were used for towing barges.
Tugs and barges owned by Bates Properties Ltd. operated in compulsory pilotage waters off the west coast of Canada and in the northwestern states of the U.S. At the time of the occurrence, the Ingenika was operating in Area 4, which is identified as compulsory pilotage waters by PPA. Wainwright Marine Services, the company that operated the Ingenika, had applied for and was granted a pilotage waiver from the PPA in March 2017 for all company employees who might perform watchkeeping duties on a tug. The waiver covered all of the company’s 6 tugs, as well as 8 of its barges and 23 personnel.
At the time of the occurrence, neither the company nor PPA had identified that the master, who had been granted a pilotage waiver, did not meet the PPA’s eligibility requirements with respect to his certificate of competency. As well, DH1, who did not hold a pilotage waiver, was in charge of a navigational watch from 1620 to 1900 on the occurrence voyage and the master was not in the wheelhouse during this time. Finally, the Ingenika was not fitted with a bridge navigational watch alarm system, nor did it have a Class A AIS.
The TSB found similar issues in occurrences involving the tug Ocean Monarch Footnote 42 in 2017and the tug Nathan E. Stewart Footnote 43 in 2016. In the Ocean Monarch occurrence, the mate did not have a pilotage waiver and was keeping a lone navigational watch at night. In the Nathan E. Stewart occurrence, the second mate did not have a pilotage waiver and was keeping a lone navigational watch at night. The Nathan E. Stewart was also not fitted with a bridge navigational watch alarm system.
1.19 Previous occurrences
Since 2015, the TSB has investigated 6 occurrences involving tugs of 15 GT or less operating on the west coast of Canada that raised issues around the adequacy of regulatory surveillance (Appendix A). Following one of these occurrences, Footnote 44 the Board issued a safety concern stating that, without adequate oversight by the Department of Transport, shortcomings in the safety management and operations of tugs of 15 GT or less may not be addressed.
Two of the 6 occurrences mentioned above also identified that the towing companies operating the tugs involved had no formal risk management processes. Footnote 45 The TSB also investigated a 3rd occurrence where the risks of the marine operations being undertaken had not been assessed and masters were left to make ad hoc decisions. Footnote 46
The TSB has identified that the trend for accidents and incidents of any type involving tugs of 15 GT or less has been relatively stable since 2013, numbering between 11 and 16 occurrences annually, with the exception of 2016, which had 27 occurrences .
1.20 TSB Watchlist
The TSB Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer.
Safety management is a Watchlist 2022 issue. Although the Ingenika was not required to have an SMS, Wainwright Marine Services had developed one voluntarily. At the time of the occurrence, however, the voluntary SMS was not fully implemented and there were gaps present in the management of safety, including an absence of guidance to help masters assess the suitability of tugs for safe operations.
ACTION REQUIRED The issue of safety management in marine transportation will remain on the Watchlist until
|
Regulatory oversight is a Watchlist 2022 issue. At present, tugs of 15 GT or less are not subject to regular inspections by TC, which means that there are few opportunities to identify and rectify regulatory contraventions until after an accident occurs. In this case, there were regulatory requirements that went unaddressed, demonstrated by the absence of emergency drills, past-due inspections and maintenance of lifesaving equipment, and crew members who did not hold the required certificates of competency for the voyage being undertaken.
ACTION REQUIRED The issue of regulatory surveillance in marine transportation will remain on the Watchlist until TC provides more oversight of the commercial vessel inspection process by demonstrating that its surveillance and monitoring are effective in ensuring that authorized representatives and recognized organizations are ensuring vessel compliance with regulatory requirements; and until TC demonstrates an increase in proactive surveillance. |
1.21 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP055/2021 – Survival Suits Examination
- LP093/2022 – Investigation of tug girding conditions
As part of the investigation into this occurrence, the TSB laboratory examined the immersion suits worn by the master and DH2 to determine their efficacy. Both suits showed resistance in zipper function. The master’s suit had resistance in the first 53 cm of the zipper, and DH2’s suit had resistance in the central part of the zipper. When the bodies of the master and DH2 were recovered, the zippers on both of their suits were found to be stopped in the area of resistance.
The TSB laboratory also used data collected during the investigation to examine the influence of certain parameters, such as towline length, as well as wind and current speed and direction for a generalized tug and barge combination that was similar to the Ingenika and Miller 204 combination. The examination had a specific focus on the tug’s intact stability.
2.0 Analysis
The analysis will focus on the causal and contributing factors that likely led to the sinking of the tug and the loss of life. The analysis will also look at management of risk in towing operations and regulatory surveillance for tugs of 15 gross tonnage (GT) or less.
2.1 Sinking of the Ingenika
Towing operations are subject to unique risks that must be managed effectively to ensure the safety of the vessel, the crew, and the environment. Although the recently introduced Small Vessel Compliance Program for Tugs highlights the need for owners and authorized representatives (ARs) to ensure that a tug’s operational limits have been ascertained, many still rely solely on the experience and judgment of individual masters for this task. At Wainwright Marine Services, ascertaining a tug’s operational limits was left to the individual masters, and there was no guidance to help them with this safety-critical task. As a result, assessments were done ad hoc without any prescribed weather limits, load limits, data regarding effective bollard pull, or information regarding the tug’s stability.
The master on the occurrence voyage had some towing experience and had informally assessed the potential effects of the weather and current on the tug and tow for the occurrence voyage.
Finding as to causes and contributing factors
Without guidance to support a comprehensive assessment of the Ingenika’s suitability for the towing operation being undertaken, the tug and barge departed in adverse weather conditions unsuitable for the operation.
The exact sequence of events leading up to the sinking could not be reconstructed, but at some point, as the tug and barge were making the turn around Europa Point, the tug suddenly heeled to starboard and began to take on water. The TSB calculated that the Ingenika’s maximum bollard pull was likely around 8 tonnes, with an effective bollard pull of around 6 tonnes in calm waters. At the time of the occurrence, in the forecasted environmental conditions, the bollard pull required for the Miller 204 to maintain headway was approximately 12 tonnes. The TSB’s calculations of bollard pull for the Ingenika demonstrate that, at the time of the occurrence in the prevailing weather conditions, the tug’s effective bollard pull was not adequate to tow the barge.
When the tug left Kitimat, it was in following seas; however, as it started making the turn around Europa Point, it encountered opposing wind and current. These conditions likely caused the tug’s effective bollard pull to decrease until it was insufficient to tow the barge. As the tug was attempting to make the turn, the heavily loaded barge may have continued on its trajectory instead of following behind the tug. This could have created a drag force on the tug that, combined with the tug’s relatively low freeboard, may have caused the tug to heel over and the deck edge to submerge.
With the tug heeled over, there was an opportunity for water to enter the hull through openings on the deck: for example, through the open engine room exhaust vents. The engine room exhaust vents were the lowest downflooding point on the tug when the other deck openings were secured. Within a short period of time, water entering through these openings would begin to downflood the tug, causing it to sink.
Finding as to causes and contributing factors
As the tug and barge were making the turn around Europa Point in opposing wind and current with a reduced effective bollard pull, the drag force of the barge may have led the tug to heel over and the deck edge to submerge, resulting in downflooding through deck openings and the vessel sinking.
The actions taken by the master and DH2 in the moments before DH1 entered the wheelhouse are not known. However, the fact that the towline was no longer attached to the tug post-occurrence and the fact that it showed no signs of having parted under tension suggest that the towing winch brake was released at some point in an attempt to abort the tow and prevent the tug from capsizing or sinking.
2.2 Survivability
As the tug sank, the 3 crew members were forced to abandon into the cold rough sea conditions. The master and DH2 had been in the process of donning their immersion suits before entering the water. For an immersion suit to work optimally, it must be fully zipped up, the hood and gloves must be donned, the inflatable head support must be inflated, and the ankle straps must be secured. If the suit is only partially zipped up or the hood is not donned, water can enter the suit and act as a weight that causes the person to sink. If the ankle straps are not secured, air pockets can collect in the lower part of the suit and cause the person’s feet to float to the surface. If the inflatable head support is not inflated, the person has no buoyant head support to keep their head above the water. A person floating horizontally in the water without an inflatable head support has a harder time keeping their head above the water than a person with an inflatable head support.
Post-occurrence, it was determined that the immersion suits worn by the master and DH2 were not fully donned. There are a number of possible reasons for this: the crew had a limited time available to don their suits before abandoning the tug and were likely hurrying to do so on a wet and unstable surface without assistance. The investigation also determined that the crew had not practised donning their suits in drills because it was not the practice for drills to be carried out on the Ingenika, which undermined their ability to become familiar with donning the suits and learn the importance of the steps involved.
The investigation also found that the zippers on both the master’s and DH2’s suits encountered an area of resistance before they were fully zipped up. Immersion suit zippers inherently have some resistance, but it was not possible to determine exactly how much resistance the zippers had before the master and DH2 entered the water. Nonetheless, the investigation did establish that the suits had not been routinely maintained, an element of which is lubricating the zippers. This may have exacerbated the resistance felt when trying to don the suits. Zipper resistance may therefore have been another factor that contributed to the master’s and DH2’s suits being only partly zipped up.
Finding as to causes and contributing factors
The immersion suits on 2 of the crew members were only partially donned, which resulted in cold water entering the suits and caused the crew members’ deaths by hypothermia and subsequent drowning.
Once in the water, a person’s survival depends on remaining afloat, keeping their mouth above the water, preserving body heat, and performing necessary survival actions. In this occurrence, considering the sequence of events, there were 2 key differences that affected survivability with respect to DH1 in relation to the master and DH2:
- Partially donned immersion suits and not using the suits’ key features reduced the master’s and DH2’s chance of survival. In particular, these factors exacerbated heat loss, increased the risk of water ingestion, and hindered their ability to manoeuvre.
- The ability to stay afloat, the absence of restrictions from a partially donned immersion suit, and DH1’s ability to enter the life raft increased his chance of survival.
Despite not having any flotation device or thermal protection, DH1 was able to stay afloat by holding onto the other crew members and he was not physically restricted by a partially donned suit full of water, which meant that he was initially in a better survival situation than the master and DH2. However, DH1’s subsequent swim to and from the life raft resulted in acute heat loss and further water ingestion, which meant that, comparatively, DH1 became in a worse survival situation than the master and DH2. Because the life raft deployed within a critical window of time when DH1’s diminishing capability to swim still matched the distance required to swim to the raft, DH1 was able to remove himself from the water before cold incapacitation caused him to drown.
Finding: Other
The surviving crew member, unencumbered by restrictions from a partially donned immersion suit, was able to remove himself from the water into the life raft before cold incapacitation caused him to drown.
2.2.1 Training and drills
In an emergency, crew members may be required to make decisions in a high-stress environment. They may have limited time available to respond and little previous experience in emergency situations. When crew members have an opportunity to regularly practise responding to different emergency scenarios through drills, the likelihood of a successful emergency response is increased.
In this occurrence, although drills were required by regulation, Wainwright Marine Services did not track or enforce the conduct of drills, and drills were not conducted on the Ingenika. This meant that crew members did not have an opportunity to regularly practise abandoning ship and the associated steps such as transmitting a distress signal, deploying the life raft, and donning immersion suits.
Additionally, although the master had completed Marine Emergency Duties (MED) training courses in 2006 and 2010, there was no requirement for him to take recurrent MED training. In this occurrence, the master had to rely on MED training that was taken many years before, and the skills acquired during training had likely degraded over time.
Findings as to risk
If crew members do not have an opportunity to regularly practise responding to emergencies through drills, there is a risk that they will not respond effectively in an emergency, decreasing their chances of survival.
If recurrent MED training is not required for crew members engaged on domestic voyages, there is a risk that they will not maintain their skills or be up to date with current knowledge and practices for handling emergencies.
2.3 Managing risk in towing operations
Tug and barge operations along the west coast of BC can involve transits through remote areas towing large quantities of fuel oils and other dangerous goods, making it critical that these operations are carried out safely. Towing accidents in such areas put the lives of crew members and the environment at risk given that distress alerting, search and rescue operations, and environmental response can be more challenging because there are fewer responding stations and VHF or cellphone signals are not always available.
Managing risk in towing operations can be a complex undertaking given that the risks change based on variables such as the specifications of the tow, the towing arrangement, the route taken, and the weather, wind, wave, and current conditions. Companies must prioritize risk management and develop guidance for masters on managing risk. Specifically, comprehensive guidance outlining operational limits supports masters in making decisions to employ risk elimination or mitigation strategies, such as delaying departure until weather conditions improve, changing the towing arrangement (e.g., using towing pins or other hold-down gear), requesting an assist tug, or using a larger tug with a higher bollard pull.
At Wainwright Marine Services, there was no guidance to help the masters manage the risks for each towing operation. The master on the occurrence voyage had some towing experience and had informally assessed the potential effects of the weather and current on the tug and tow for the occurrence voyage. However, the absence of guidance meant that he had no prescribed operational limits, data regarding effective bollard pull, or stability information to help with his assessment. This issue is not unique to this company; previous TSB investigations have identified an absence of formal risk management processes in other towing companies.
Finding as to risk
If towing companies do not prioritize risk management and provide guidance to help masters assess the suitability of tugs for the towing operations being undertaken, operational limits can be exceeded, placing the crew, the tug, the tow, and the environment at risk.
2.4 Regulatory surveillance
2.4.1 Transport Canada
Effective oversight by Transport Canada (TC) is required to ensure that owners and operators of tugs of 15 GT or less comply with safety-critical regulations. Unlike larger tugs, this particular class of smaller vessels is not required to be certified or inspected under the current regulatory framework. Consequently, these tugs are not subject to any limitations on voyages, on the type of activity for which the vessel is used (e.g., towing), or on the conditions in which the vessel is operating (e.g., weather).
To assist in managing risk, TC requires ARs to develop safe operating procedures and emergency procedures. However, what constitutes safe operating procedures is open to interpretation, and this requirement has not been effective in ensuring that tugs of 15 GT or less have risk management processes to help tug masters assess the hazards present in their towing operations.
In this occurrence, in addition to an absence of guidance on tug suitability, there were some regulatory requirements that were not met. The investigation identified that
- emergency drills were not conducted,
- maintenance of lifesaving equipment was not always done according to schedule,
- inspection records were not up to date,
- the master’s certificate of competency was limited to passenger vessels operated by a specific company, and his practical knowledge of towing operations had not been assessed by TC, and
- the deckhand in charge of a navigational watch did not hold a certificate of competency.
Without any regulatory surveillance of the tug by TC, these issues persisted.
The TSB has previously issued a safety concern on the issue of regulatory surveillance for tugs of 15 GT or less. Over the past 15 years, TC has undertaken some initiatives on tug and barge issues, but none of these initiatives have resulted in a reduction in the number of reported hazardous situations. In 2022, TC provided additional guidance to owners and ARs through the Small Vessel Compliance Program for Tugs. However, participation in the program is not mandatory and, without regular TC inspections, there is no way to verify its effectiveness.
Finding as to risk
If tugs of 15 GT or less are not subject to adequate regulatory surveillance, there is a risk that hazardous conditions and practices will not be addressed, leading to accidents.
2.4.2 Pacific Pilotage Authority
Under the pilotage waiver system, the Pacific Pilotage Authority (PPA) relies on companies to ensure that, during transit, company crew members are maintaining a standard of safety comparable to that provided by a licensed pilot. The PPA provides requirements for waiver holders to meet with respect to crew members in charge of a navigational watch, as well as for navigational equipment that must be on board.
The investigation into this occurrence identified shortcomings in Wainwright Marine Services’ compliance with the conditions of its pilotage waiver and with oversight of the waiver system provided by the PPA. For example, although the master had been issued a pilotage waiver, he held a certificate of competency that was restricted to passenger vessels operated by a specific company and therefore should not have been eligible for a waiver on a towing vessel. As well, DH1 had, on various occasions, been put in charge of a navigational watch on board the Ingenika, but did not hold a certificate of competency or a pilotage waiver. Further, the tug was not fitted with a bridge navigational watch alarm system and did not have a Class A automatic identification system, both of which are requirements for a vessel operating under a waiver.
Because the PPA does not routinely review restrictions on certificates of competency before issuing waivers and relies on ARs to verify that crew members and vessels comply with PPA requirements, these shortcomings went unnoticed.
Finding as to risk
Without verification that crew members and vessels meet PPA waiver requirements, there is a risk that non-compliance with waiver requirements will go undetected and compromise safety in compulsory pilotage waters.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- Without guidance to support a comprehensive assessment of the Ingenika’s suitability for the towing operation being undertaken, the tug and barge departed in adverse weather conditions unsuitable for the operation.
- As the tug and barge were making the turn around Europa Point in opposing wind and current with a reduced effective bollard pull, the drag force of the barge may have led the tug to heel over and the deck edge to submerge, resulting in downflooding through deck openings and the vessel sinking.
- The immersion suits on 2 of the crew members were only partially donned, which resulted in cold water entering the suits and caused the crew members’ deaths by hypothermia and subsequent drowning.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If crew members do not have an opportunity to regularly practise responding to emergencies through drills, there is a risk that they will not respond effectively in an emergency, decreasing their chances of survival.
- If recurrent Marine Emergency Duties training is not required for crew members engaged on domestic voyages, there is a risk that they will not maintain their skills or be up to date with current knowledge and practices for handling emergencies.
- If towing companies do not prioritize risk management and provide guidance to help masters assess the suitability of tugs for the towing operations being undertaken, operational limits can be exceeded, placing the crew, the tug, the tow, and the environment at risk.
- If tugs of 15 gross tonnage or less are not subject to adequate regulatory surveillance, there is a risk that hazardous conditions and practices will not be addressed, leading to accidents.
- Without verification that crew members and vessels meet Pacific Pilotage Authority waiver requirements, there is a risk that non-compliance with waiver requirements will go undetected and compromise safety in compulsory pilotage waters.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- The registration information for the Ingenika’s emergency position-indicating radio beacon was not up to date, which meant that search and rescue resources were not able to immediately contact the tug’s current owner.
- The surviving crew member, unencumbered by restrictions from a partially donned immersion suit, was able to remove himself from the water into the life raft before cold incapacitation caused him to drown.
4.0 Safety action
4.1 Safety action taken
4.1.1 Wainwright Marine Services
Following the occurrence, Wainwright Marine Services carried out a review of all crew certification and worked with all existing and new crew to ensure that their certification was not restricted to other organizations or vessels. In addition, Wainwright Marine Services hired an individual to provide training to crew members on decision making, stability, and girding. Finally, Wainwright Marine Services digitized its safety management system to facilitate updates and to ensure that company employees can access it at any time.
4.1.2 Transport Canada
In January 2022, Transport Canada (TC) established the Pacific Coast Tow and Workboat Safety Advisory Group, which includes representatives from industry, labour, and the government of British Columbia. The group’s purpose is to raise issues, develop initiatives, and put forward practical solutions and industry best practices. It also presents findings and makes recommendations to federal marine safety regulators and provincial occupational health and safety regulators regarding potential changes to regulatory, enforcement, and health and safety regimes.
TC has also increased its outreach efforts to enrol tugs of 15 gross tonnage (GT) or less in the Small Vessel Compliance Program for Tugs. The authorized representatives for all of these tugs were contacted directly by TC. In the Pacific region, a targeted monitoring inspection campaign was initiated in January 2022 to verify compliance of tugs of 15 GT or less. At September 2022, more than 50 compliance inspections had been conducted.
Finally, the scope of the existing memorandum of understanding between TC and WorkSafeBC is being expanded to include all commercial vessels in British Columbia, including tugs. Previously, the memorandum of understanding was limited to sharing information on operational or occupational health and safety concerns about fishing vessels.
4.2 Safety action required
4.2.1 Safe operation of tugs of 15 gross tonnage or less
On 10 February 2021, the tug Ingenika, with 3 crew members on board, was towing the loaded barge Miller 204 in the Gardner Canal when the tug sank approximately 16 nautical miles west‑southwest of Kemano Bay, British Columbia (BC). The barge subsequently drifted and went aground about 2.5 nautical miles southwest from where the tug sank. The search and rescue operation located 1 surviving crew member on land and recovered the bodies of the 2 other crew members from the water. The barge was recovered; the tug was not found. At the time of the occurrence, the tug had 3500 L of diesel fuel in tanks on board.
4.2.1.1 Regulatory surveillance for tugs of 15 gross tonnage or less
At September 2022, there were approximately 1343 tugs of 15 GT or less registered in Canada, approximately 1035 of which were registered in BC. Since 2015, the TSB has investigated 6 occurrences involving tugs of 15 GT or less operating on the west coast of Canada that have raised issues around the adequacy of regulatory surveillance. Footnote 47
TC does not certify tugs of 15 GT or less, nor are these vessels required to undergo regular inspections. By comparison, before being certified by TC under the Vessel Safety Certificates Regulations, tugs of greater than 15 GT but of less than 150 GT are required to be inspected every 4 years, and tugs of 150 GT and greater are required to be inspected annually. Although TC has set an annual target of inspecting 3% of tugs of 15 GT or less nationwide, most will go years between inspections and may never be inspected over the life of the vessel. For example, the Ingenika was built in 1968 and had been in operation for over 50 years before this occurrence; the investigation found that there were no records of TC performing an inspection at any point in the tug’s operational life.
The TSB also recently investigated another occurrence involving a tug of 15 GT or less, the Risco Warrior, Footnote 48 which was built in 1961 and had never been inspected. That investigation found that, in the absence of comprehensive regulatory surveillance and enforcement, there is a risk that tugs of 15 GT or less will continue to be operated with unsafe equipment and operating practices. While vessel owners and operators have the primary responsibility to manage safety, it is vital that TC provide effective oversight and proactively intervene to ensure that vessel owners and operators comply with regulations and standards and can manage the safety of their operations effectively.
From April to October 2022, TC conducted 30 risk-based monitoring inspections of tugs of 15 GT or less. Overall, 21 of these inspections resulted in a total of 62 deficiencies, including 13 related to lifesaving equipment, 12 related to structure or stability, 8 related to crew certificates, 6 related to fire safety, and 5 related to navigation safety.
From April to October 2022, TC also conducted 120 statutory inspections of tugs of greater than 15 GT. Sixty-four of these inspections resulted in the identification of deficiencies. Statutory inspections are generally more comprehensive than risk-based monitoring inspections. In addition, TC conducted 30 risk-based monitoring inspections of tugs of greater than 15 GT on the basis of findings from the statutory inspections. Of these 30 risk-based monitoring inspections, 19 resulted in the identification of deficiencies.
In 2018–19, TC conducted a concentrated inspection campaign on domestic vessels. According to the campaign report, Footnote 49 83 vessels were inspected nationwide, 49 of which were inspected under the annual inspection category and 34 through quadrennial inspections per the Hull Inspection Regulations. Footnote 50 Nineteen of the vessels inspected were tugs, but none were of 15 GT or less. The data showed that vessels inspected every 4 years had more deficiencies than those inspected annually.
TC also focused on tugs in a concentrated inspection campaign conducted in BC from January to March 2017. Thirty tugs of 15 GT or less and 30 tugs of greater than 15 GT were selected for inspection. TC concluded that tugs of 15 GT or less had significantly more instances of regulatory non-compliance than tugs of greater than 15 GT. Footnote 51
For tugs of 15 GT or less, the onus is on the authorized representative (AR) to ensure compliance with the regulations and the safe operation of the vessel. However, in its Watchlist 2022, the TSB highlighted that many ARs of small vessels, such as the Ingenika, have limited awareness of key sections of the Canada Shipping Act, 2001 and of the broader regulatory framework. Other ARs may not be motivated to comply with regulations, given that it is well known that TC is unlikely to inspect their vessels and so the probability of enforcement is low.
Recognizing the level of risk present, in 2016, the Board issued a safety concern Footnote 52 on the issue of regulatory surveillance for tugs of 15 GT or less. On 25 June 2022, TC pre-published the proposed Marine Safety Management System Regulations, which will require tugs of 15 GT or less to develop a safety management system and obtain a Canadian safety management certificate. TC also developed and implemented the Small Vessel Compliance Program for Tugs (SVCP-T), which provides a simplified description of regulatory requirements and useful information that companies and ARs can use to evaluate their regulatory compliance. Although these are encouraging initiatives, neither are a replacement for vessel inspections under a broader program of regulatory surveillance, which would provide an opportunity to examine a vessel and its equipment to verify that it is in compliance with the regulatory requirements and being operated safely. Without adequate surveillance by TC, shortcomings in the safety management and operations of tugs of 15 GT or less will continue to go unaddressed, leading to accidents. Therefore, the Board recommends that
the Department of Transport expand its surveillance program to include regular inspections of tugs of 15 gross tonnage (GT) or less to verify that these vessels are complying with regulatory requirements.
TSB Recommendation M23-01
4.2.1.2 Risk assessments for tugs of 15 gross tonnage or less
The TSB has noted that, in addition to the need for regulatory surveillance for tugs of 15 GT or less, there is currently no requirement for towing companies operating these tugs to assess any of the risks that might be present in their operations, even when it comes to something as essential as assessing the suitability of their tugs for the towing operations they are undertaking. Although the present investigation focused on tugs of 15 GT or less, it was noted that there are also no requirements for risk assessments for tugs of greater than 15 GT.
Although the Canada Shipping Act, 2001 requires the AR of any vessel to develop safe operating procedures and requires the master to ensure the safety of the vessel and anyone on board, what constitutes safe operating procedures is open to interpretation, and these requirements have not resulted in the effective management of risk on tugs of 15 GT or less. Combined with the fact that tugs in this category go largely uninspected and have no restrictions on their operations, there is the potential for accidents like the one involving the Ingenika to occur.
Requirements for risk assessment do exist for some towing vessels; TC requires a risk assessment to be performed when a vessel is towing a vessel carrying oil or dangerous chemicals in bulk. Footnote 53 These types of risk assessments provide an opportunity to look at each aspect of the towing operation, such as the weather, hazards posed by the cargo, and suitability of the tug for the tow. TC’s recently developed SVCP-T Footnote 54 also provides useful data that can be used in risk assessments to support safe towing operations.
Since the occurrence involving the Ingenika, TC has taken some initiatives to improve tug safety through the development of the SVCP-T and the pre-publication of the proposed Marine Safety Management System Regulations in the Canada Gazette, Part I. The proposed regulations, in particular, give TC an opportunity to develop regulatory provisions to ensure that companies operating tugs of 15 GT or less incorporate risk assessments into their operations. However, although the SVCP-T and the proposed regulations are positive steps forward, in their present forms, they do not explicitly require tug operators to conduct risk assessments. This means that risks in towing operations will continue to go undetected and unmitigated, placing crews, tugs, tows, and the environment in danger. Therefore, the Board recommends that
the Department of Transport require authorized representatives of tugs of 15 gross tonnage (GT) or less to assess the risks present in their operations, including the suitability of their tugs for the specific towing operations they are undertaking.
TSB Recommendation M23-02
4.2.1.3 Pacific Pilotage Authority oversight of pilotage waivers
At the time of the occurrence, the Ingenika was operating in a compulsory pilotage area that falls under the responsibility of the Pacific Pilotage Authority (PPA). The PPA is a Crown corporation that has a mandate to establish, operate, maintain, and administer safe and efficient pilotage services in British Columbia. Pilotage services are provided by licensed pilots, who are highly trained navigators that use their knowledge of local waters to direct a vessel and navigate it using the safest route.
The PPA has a pilotage waiver system under which some vessels, mainly tugs, may obtain waivers that exempt them from having to take a licensed pilot on board in designated pilotage areas if the operators and tugs meet certain requirements. However, when a company requests a pilotage waiver, the PPA does not check the information submitted to ensure that it meets regulatory requirements, and the PPA relies on operators to ensure that they are complying with waiver conditions once a waiver is granted. In BC, there are currently 364 tugs, owned by 85 different companies, that operate under pilotage waivers.
This investigation identified that, although the master of the Ingenika had been issued a pilotage waiver, he held a certificate of competency that was restricted to passenger vessels operated by a specific company and therefore should not have been eligible for a waiver on a towing vessel. As well, one of the deckhands had, on various occasions, been put in charge of a navigational watch on board the Ingenika, but he did not hold a certificate of competency or a pilotage waiver. Further, the tug was not fitted with a bridge navigational watch alarm system and did not have a Class A automatic identification system, both of which are requirements for a vessel operating under a waiver.
This investigation is not the first to identify shortcomings around the PPA’s process for issuing waivers and its reliance on companies to ensure ongoing compliance with waiver conditions. The TSB found similar issues in occurrences involving the tug Ocean Monarch Footnote 55 in 2017and the tug Nathan E. Stewart Footnote 56 in 2016.
Without an effective process to verify that crew members and vessels meet PPA waiver requirements, there is a risk that non-compliance with waiver requirements will go undetected and compromise safety in compulsory pilotage waters. Given the need to ensure that waivered vessels are operating at a level of safety comparable to that afforded by a licensed pilot, the Board recommends that
the Pacific Pilotage Authority verify that eligibility requirements are met before issuing pilotage waivers to companies operating tugs in compulsory pilotage areas.
TSB Recommendation M23-03
the Pacific Pilotage Authority implement a process to verify ongoing compliance with waiver conditions by companies operating tugs in compulsory pilotage areas.
TSB Recommendation M23-04
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Occurrences involving regulatory surveillance of tugs of 15 gross tonnage or less operating on the west coast of Canada
M20P0230 (Risco Warrior) – On 07 August 2020, an explosion occurred in the battery compartment of the tug Risco Warrior while at the dock in Bute Inlet, British Columbia (BC). The vessel sustained structural damage, and 2 people on board sustained minor injuries. The investigation into the occurrence found that in the absence of comprehensive regulatory surveillance and enforcement, there is a risk that tugs of 15 gross tonnage (GT) or less will continue to be operated with unsafe equipment and operating practices.
M19P0246 (Sheena M) – On 01 October 2019, the tug Sheena M was towing a loaded barge when the tug capsized and sank near Williamsons Landing, BC. The 2 people on board were rescued by a nearby boom boat. The investigation into the occurrence found that without adequate oversight by Transport Canada, shortcomings in the safety management and operations of tugs of 15 GT or less may not be addressed.
M17P0244 (Ocean Monarch) – On 09 July 2017, the tug Ocean Monarch was towing a barge when the tug made bottom contact in Princess Royal Channel, BC. The tug’s hull and starboard propeller nozzle were damaged. The investigation into the occurrence found that if tugs of 15 GT or less are not subject to adequate regulatory oversight, there is a risk that shortcomings in operations will not be resolved, endangering the crew, the vessel, and the environment.
M16P0241 (Ken MacKenzie) – On 11 July 2016, the tug Ken Mackenzie sustained a fire in the engine room while transiting the Fraser River, BC. The 2 crew members abandoned the vessel and the fire was extinguished. The investigation into the occurrence found that if adequate regulatory oversight is not applied to tugs of 15 GT or less, instances of unsafe equipment and operating conditions may continue to occur, putting people, assets, and the environment at risk.
M16P0062 (H.M. Scout) – On 02 March 2016, the tug H.M. Scout lost the 2 barges it was towing when the tow line parted off Victoria, BC. The broken tow line then fouled the tug’s propeller. The investigation into the occurrence found that if tugs of 15 GT or less are not subject to adequate regulatory oversight to ensure compliance with regulations, there is a risk that shortcomings in operations will go unresolved.
M15P0037 (Syringa) – On 18 March 2015, the tug Syringa was towing a loaded barge when the tug sank 6 nautical miles west of Sechelt, BC. Following the investigation into the sinking, the Board issued a safety concern stating that, without adequate oversight by the Department of Transport, shortcomings in the safety management and operations of tugs of 15 GT or less may not be addressed.
Appendix B – Pacific Pilotage Authority compulsory pilotage waters
