Loss of control and collision with terrain
Airspan Helicopters Ltd.
Bell 212, C-GNYI
Bowen Island, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 05 March 2021, the Airspan Helicopters Ltd. Bell 212 helicopter (registration C-GNYI, serial number 30569) with 2 pilots on board was travelling from Sechelt Aerodrome (CAP3), British Columbia, to Cypress Provincial Park, located in West Vancouver, British Columbia, to support a BC Hydro project.
At 0946 Pacific Standard Time, while in the cruise portion of the flight, the helicopter entered wind shear and experienced a sudden, dramatic right roll with nose-down pitch. After regaining control, the number 2 engine experienced an uncommanded in-flight shutdown and the flight controls became very hard to manipulate.
A location on nearby Bowen Island, British Columbia, was selected for an emergency landing; however, the helicopter was still difficult to control and the pilots were unable to manoeuvre it to the desired location. During the descent, the helicopter began a rapid rotation to the right, which the pilots were unable to arrest. After several rotations, the helicopter collided with trees and came to rest on a rocky ridge approximately 270 feet above sea level on the northwest corner of Bowen Island.
Both occupants received serious injuries. The helicopter was substantially damaged, but there was no post-impact fire. The emergency locator transmitter activated and a signal was received by the Canadian Mission Control Centre, in Trenton, Ontario.
1.0 Factual information
1.1 History of the flight
On 05 March 2021, the Airspan Helicopters Ltd. (Airspan Helicopters) Bell 212 helicopter (registration C-GNYI, serial number 30569) was scheduled to depart Sechelt Aerodrome (CAP3), British Columbia (BC), with 2 pilots on board for a visual flight rules (VFR) flight. The helicopter would be heading to a staging area about 21 nautical miles (NM) east in Cypress Provincial Park, BC, to complete a multi-day longline project in collaboration with BC Hydro. The plan, once the aircraft arrived at the staging area, was for the second pilot to do the longline work and the pilot-in command (PIC) to monitor him as part of a performance evaluation by BC Hydro for the installation of 230 kV high-voltage transmission line structures.
Before preparing the helicopter for departure, the pilots checked the available weather resources, which included graphic area forecasts (GFAs), aerodrome forecasts (TAFs), aerodrome routine meteorological reports (METARs), and the marine forecast issued by Environment and Climate Change Canada. According to the forecasts, moderate, with localized severe, mechanical turbulence and low-level wind shear were expected in the area in which the pilots would be operating. Though the strong winds were a concern, the flight was dispatched with the knowledge that it would be a turbulent flight. The PIC made the decision to depart based on an improving forecast later in the day, the desire to complete the operational flight, and the observation that other aircraft were operating in and out of Sechelt Aerodrome. The second pilot then began to prepare the helicopter for the flight.
At approximately 0900,Footnote 1 the PIC contacted BC Hydro crews, who had just arrived at the work site in Cyprus Mountain Provincial Park, for additional wind information. At 0927, the helicopter was started, and an engine power assurance check was completed. The helicopter then lifted off and headed east towards Cypress Provincial Park at approximately 0935. The PIC was seated in the right seat and the second pilot, who was the pilot flying, was seated in the left seat.
The helicopter climbed and established a cruise between 2300 feet and 2600 feet above sea level (ASL) for the next several minutes, encountering light turbulence and variable winds from the east and southeast.
As the helicopter flew towards Keats Island, BC (Figure 1), the pilots observed localized surface waves (or “cat’s paws”Footnote 2) indicating downdrafts in the area. They discussed the likelihood of increasing turbulence based on those observations. Above the northern tip of Keats Island, the second pilot slowed the helicopter to 75 knots indicated airspeed (66 knots ground speed)Footnote 3 and changed its track slightly to the north at approximately 2600 feet ASL. The pilots were expecting mechanical turbulence coming from Bowen Island, which has a peak elevation of 2388 feet ASL.

The helicopter’s speed increased as it began crossing Collingwood Channel, reaching a speed of 78 knots ground speed at an altitude of approximately 2560 feet ASL. As it flew above the channel, the helicopter passed through an area of moderate turbulence. Soon after, at 0945:24, the helicopter was roughly 2 NM west of Bowen Island, on the lee side at an altitude of approximately 2430 feet ASL, when it entered another area of turbulence with a severe downward force.
While travelling at a ground speed of 73 knots on a track of approximately 110°, the helicopter violently pitched nose down and began a rapid right roll. The cyclic was momentarily pulled from the second pilot’s hand due to the aircraft’s violent, rapid movement. The helicopter rolled inverted, or close to inverted, during this loss of control, and the PIC joined the second pilot on the controls to attempt a recovery. The second pilot applied maximum aft cyclic in the recovery attempt. During this period, the helicopter fell approximately 1400 feet to an altitude of approximately 1040 feet ASL; a descent rate of 8220 fpm.
Several items, such as a spare headset, handheld radio, flight manual, and lunchbox, were launched forward from the rear cabin and struck the pilots on their helmets. The visor cover and yellow visor on the second pilot’s helmet were knocked down over his face, blocking his vision momentarily. With the PIC also on the controls, the second pilot was able to let go of the flight controls momentarily in order to force the visor cover up off his face and out of his vision. The yellow visor remained down for the remainder of the flight.
Several gauges broke from their mounts during the violent descent. These gauges slid from their seated position within the instrument panel.
The pilots were able to regain some control of the helicopter 0.6 NM east of Bowen Island and 1 NM from Keats Island, maintaining the helicopter on an easterly heading. Observers on the ground saw a puff of grey smoke come from the helicopter as it levelled off.
Moments after the helicopter had levelled off, both pilots were still struggling to use the controls, and they noticed that the anti-torque pedals had become very difficult to move and the cyclic was slow to respond to inputs. At that time, the pilots observed a hydraulic caution light indicating a drop in hydraulic pressure below an acceptable threshold for operations. Due to the high workload of trying to control the helicopter, neither pilot had the opportunity to look at the instruments to determine whether the No. 1 or No. 2 hydraulic system had failed. The pilots selected a large field on the northwest corner of Bowen Island as an emergency landing site.
The PIC then observed the No. 2 engine out indication light illuminate when the helicopter was at an altitude of approximately 900 feet ASL and 1.2 NM from the proposed landing site. He communicated an engine out indication to the second pilot, but did not specify which engine had the indication, causing some uncertainty as to which engine was working. The second pilot glanced at the caution lights but was unable to ascertain which engine light was on while he was maintaining control of the helicopter. He then confirmed that both throttles were at maximum power. The controllability of the helicopter, along with a loss of engine power, caused the pilots to revise their choice of landing site to a closer field.
On final for the field, the PIC turned on the emergency locator transmitter (ELT), prompting the second pilot to broadcast a mayday call over the radio on frequency 123.20 MHz. The mayday call was heard by other aircraft in the area, but not by air traffic control.
As they descended and decelerated, the helicopter began to yaw to the right, resulting in another loss of control. The PIC communicated to the second pilot that they had a tail rotor failure.
At approximately 150 feet above the landing site, the second pilot reduced both throttles to the idle position in an attempt to slow the rotation. Moments later, the helicopter began contacting the trees at approximately 310 feet ASL. As tree contact was made, the second pilot pulled up on the collective to slow the descent and cushion the impact. The helicopter dropped and came to rest inverted on a rocky ledge at approximately 270 feet ASL.
Fuel lines under the cabin floor panel were compromised during the impact and began leaking fuel onto the pilots, who were still seated in the inverted fuselage, restrained by their safety harnesses. Footnote 4 The PIC assisted the second pilot, whose foot was pinned in the footwell, and they both egressed successfully. The pilots were located by locals who had witnessed the accident and rushed to the area to assist. Both pilots were transported to hospital for evaluation.
1.2 Injuries to persons
Both pilots received serious injuries.
| Degree of injury | Crew | Passengers | Persons not on board the aircraft | Total by injury |
|---|---|---|---|---|
| Fatal | 0 | - | - | 0 |
| Serious | 2 | - | - | 2 |
| Minor | 0 | - | - | 0 |
| Total injured | 2 | - | - | 2 |
1.3 Damage to aircraft
The helicopter was substantially damaged as a result of impact forces.
1.4 Other damage
The helicopter came to rest on a vacant piece of private property. Several trees were knocked down, cut, or dislodged from the hillside.
An unknown amount of jet fuel leaked onto the rocks and soil surrounding the wreckage.
1.5 Personnel information
| Pilot-in-command | Second pilot | |
|---|---|---|
| Pilot licence | Commercial pilot licence – helicopter | Commercial pilot licence – helicopter |
| Medical expiry date | 01 April 2021 | 01 January 2022 |
| Total flying hours | 9125.5 | 5756.5 |
| Flight hours on type | 1247 | 479.5 |
| Flight hours in the 7 days before the occurrence | 0.2 | 2.2 |
| Flight hours in the 30 days before the occurrence | 1.5 | 9.5 |
| Flight hours in the 90 days before the occurrence | 5.7 | 24.7 |
| Flight hours on type in the 90 days before the occurrence | 0.2 | 12.9 |
| Hours on duty before the occurrence | 1 | 1.5 |
| Hours off duty before the work period | 15 | 15 |
The PIC held a commercial pilot licence – helicopter and had worked at Airspan Helicopters for more than 20 years. He was the company’s President and Operations Manager. He had completed recurrent training in the Bell 212 on 05 March 2020 and his initial mountain flying training in 2001. He had also completed an Airspan Helicopters mountain flying refresher course on 09 January 2020 and a pilot proficiency check on 06 March 2020, which tested the following abnormal and emergency procedures: engine inoperative, autorotation from hover and 180°, hydraulic failure, governor failure, engine fire, and tail rotor failure.
The PIC was also qualified as a Transport Canada approved check pilot. He had completed the recurrent ground training from 20 to 22 February 2021 and the Transport Canada-monitored flight test on 24 February 2021.
The second pilot held a commercial pilot licence – helicopter and had worked at Airspan Helicopters for approximately 6.5 years. He had completed his recurrent training on 19 February 2021, his initial mountain flying training in 2010, an Airspan Helicopters mountain flying refresher course on 22 January 2021, and a pilot proficiency check on 24 February 2021, which tested the following abnormal and emergency procedures: engine inoperative, tail rotor jam, in-flight fire, governor failure, and hydraulic failure.
Both pilots had completed the company crew resource management course on 26 October 2020. The course covered several topics, including threat and error management, communications, decision making, pressure, and stress.
The investigation determined that the pilots held the appropriate licences and met the recency requirements for the flight in accordance with existing regulations. Based on a review of the pilots’ work-rest schedules, fatigue was not considered a factor in the occurrence.
1.6 Aircraft information
The Bell 212 is a twin-engine, single-main-rotor helicopter that can carry up to 14 passengers with 1 pilot. On the day of the occurrence, however, only the pilot seats were installed. All the others had been removed to reduce weight for longlining.
The occurrence helicopter had been modified to have an increased horsepower rating, a configuration incorporated in Bell Textron Inc. Technical Bulletin 212-91-138.Footnote 5 A helicopter with this modification is commonly referred to as a Bell 212 HP.
The main rotor assembly is a 2-bladed, teetering, semi-rigid type. The design of the rotor allows for blade flapping and pitch change of individual blades. Blade flapping is necessary to compensate for dissymmetry of lift. The blades are free to flap vertically to compensate for various in-flight aerodynamic forces. They are rigidly connected to the hub, allowing them to flap as a unit, and the hub is free to teeter with respect to the rotor mast.
In April 2013, the helicopter had been modified to include a Boundary Layer Research Aerospace FastFin system. The FastFin system modifies the tail boom with 2 parallel stall strips (tail boom strakes) and a re-shaped vertical fin. The results of this modification are a performance enhancement during hover operations and a tail rotor made more efficient by having less thrust blocked than with the original vertical fin. The newly shaped vertical fin also assists with pilot workload because fewer anti-torque pedal inputs are required during flight.
A technical records review did not reveal any conditions related to aircraft maintenance that would have contributed to the occurrence. The helicopter had no known deficiencies before the occurrence flight. Its weight and centre of gravity were within the prescribed limits, and there was sufficient fuel on board to complete the flight.
| Manufacturer | Bell Textron Inc. |
|---|---|
| Type, model and registration | Bell 212, C-GNYI |
| Year of manufacture | 1973 |
| Serial number | 30569 |
| Certificate of airworthiness / flight permit issue date | 13 March 2012 |
| Total airframe time | 29 220.0 hours |
| Engine type (number of engines) | Pratt & Whitney Canada PT6T-3B (2) |
| Rotor type (number of blades) | Semi-rigid (2) |
| Maximum allowable take-off weight | 5080 kg |
| Recommended fuel type(s) | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A |
The Bell Model 212 Rotorcraft Flight Manual (RFM) outlines procedures for engine failure, hydraulic system failure, and complete loss of tail rotor thrust. There are currently no procedures that apply to the scenario faced by the occurrence pilots. The RFM states that “[i]ntentional manoeuvring resulting in roll attitudes in excess of 50° angle of bank […] are prohibited.” Footnote 6 While not intentional, during the first loss of control, the aircraft exceeded this limit.
1.7 Meteorological information
1.7.1 Forecasted weather
The pilots departed Sechelt (CAP3) at approximately 0930. The most recent GFAs issued for the area were issued at 0330. Those reports forecast that at 1000 a cold front would be moving through the vicinity of Bowen Island. The forecast included moderate mechanical turbulence and low-level wind shear from the surface to 3000 feet above ground level (AGL) as well as localized severe mechanical turbulence and low-level wind shear at the same altitudes. Frequent towering cumulus clouds with tops at 16 000 feet ASL were also forecasted. The surface winds in the area were forecasted to be 25 knots with gusts to 35 knots.
Vancouver International Airport (CYVR), BC, is the closest weather reporting station for which a TAF is produced. The TAF for CYVR was issued at 0639 on 05 March 2021 and was valid for a 27-hour period starting at 0700. The TAF indicated the following conditions between 0700 and 1100:
- winds from 110° true (T) at 18 knots, gusting to 28 knots
- visibility more than 6 statute miles (SM)
- scattered cloud at 6000 feet AGL
- overcast ceiling at 10 000 feet AGL
Between 0700 and 1100, there would be the following temporary change to the prevailing conditions:
- light rain showers
- overcast ceiling at 6000 feet AGL
After 1100, the weather was forecasted to be:
- winds from 130°T at 15 knots
- visibility more than 6 SM
- light rain
- scattered cloud at 2000 feet AGL
- overcast ceiling at 5000 feet AGL
1.7.2 Actual weather
The 0800 and 0900 METARs issued for CYVR, both showed a visibility of 20 SM, few clouds below 2000 feet ASL, and ceilings at 7400 feet ASL or higher. Table 4 lists other reported observations.
| Observation | 0800 | 0900 |
|---|---|---|
| Wind direction | 100°T | 120°T |
| Wind speed | 16 knots with gusts to 25 knots | 19 knots with gusts to 26 knots |
| Temperature / dew point | 10° C / 5° C | 11° C / 5° C |
| Altimeter setting | 29.74 inches of mercury | 29.78 inches of mercury |
In addition to the information available from the weather observations at CYVR, there are a number of other stations in the vicinity of the accident that also report weather (Figure 2).

The wind direction and speed from weather observations taken at 0900 and 1000 at these weather reporting stations are listed in Table 5.
| Station | Wind direction and speed at 0900 | Wind direction and speed at 1000 |
|---|---|---|
| Sechelt (CAP3)* | 130°T at 15 knots | 130°T at 15 knots |
| Pam Rocks | 130°T at 32 knots, with gusts to 45 knots | 120°T at 36 knots, with gusts to 52 knots |
| Point Atkinson* | 110°T at 30 knots | 110°T at 30 knots |
| Vancouver (CYVR) | 120°T at 19 knots with gusts to 26 knots | 140°T 26 knots, with gusts to 38 knots |
* These automated weather stations only collect sustained winds and not wind gusts.
In addition to the recorded weather observations, local observers reported similar conditions. On the day of the accident, a floatplane pilot heard the occurrence helicopter’s mayday call and attempted to overfly the accident site at 1000 feet ASL to gain more information. The floatplane encountered severe turbulence as it flew into the Collingwood Channel (Figure 1), causing the airplane to bank steeply (in excess of 70°) and items to be thrown from the seat pockets. The pilot of the floatplane left the area.
1.7.3 Environment and Climate Change Canada analysis
After the accident and at the request of the TSB, Environment and Climate Change Canada performed an in-depth analysis of the weather conditions affecting the Howe Sound area at the time of the occurrence.
The meteorological assessmentFootnote 7 determined that on the morning of the occurrence, a low-pressure centre just north of Vancouver Island was moving inland with associated warm and cold fronts, and there were relatively higher surface pressures in the interior of BC. This pressure gradient, with high pressure inland and lower pressure over the coast, often leads to strong outflow winds draining from the interior through any inlets and channels. These strong outflow winds were observed over Howe Sound.
Radar images from the Aldergrove radar, located approximately 48.6 NM from the accident site, indicated localized heavier precipitation that may have been a result of convection embedded within the precipitation band. Convection is known to produce turbulence, wind shear, and icing.
The assessment further explained that Howe Sound, like all inlets along the BC coast is prone to strong and sometimes gusty outflow winds. In addition, the complex terrain within the inlet would lead to varying wind directions and speeds as one considers airflow being diverted around and over the various islands within the Sound.
1.7.4 Wind effects
On the morning of the occurrence, strong southeasterly winds were blowing in the vicinity of the accident site. The west side of Bowen Island is dominated by a long ridge which is anchored at the south end by Mount Gardner with an elevation of 2388 feet ASL. The flight’s intended destination, Cypress Provincial Park, is approximately 6 NM east of Bowen Island. Within the park are Mount Strachan with an elevation of 4714 feet ASL and Black Mountain with an elevation of 4016 feet ASL (Figure 3).

The final minutes of the occurrence flight would have been flown on the downwind, or lee side, of this terrain. NAV CANADA’s The Weather of British Columbia Graphic Area Forecast 31 explains that,“[w]hen air flows across a mountain or hill, it is disturbed the same way as water flowing over a rock.”Footnote 8 Wind on the lee side of a hill or mountain is affected by its passage over the terrain and lee effects of wind in mountainous areas are known to create severe turbulence. A large eddy called a “rotor” may form below each wave crest once a lee wave pattern has been established (Figure 4). Lee effects are described in The Weather of British Columbia as follows:
When the winds blow against a steep cliff or over rugged terrain, gusty turbulent winds result. Eddies often form downwind of the hills, which create stationary zones of stronger and lighter winds. These zones of strong winds are fairly predictable and usually persist as long as the wind direction and stability of the air stream do not change. The lighter winds, which occur in areas called wind shadows can vary in speed and direction, particularly downwind of higher hills. In the lee of the hills, the wind is usually gusty and the wind direction is often completely opposite to the wind blowing over the top of the hills. Smaller reverse eddies may also be encountered close to the hills.Footnote 9
![Lee effects (Source: NAV CANADA, The Weather of British Columbia: Graphic Area Forecast 31 [2001], Figure 2-10.)](/sites/default/files/eng/rapports-reports/aviation/2021/a21p0018/images/a21p0018-figure-04.jpg)
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
Not applicable.
1.11 Flight recorders
1.11.1 General
The occurrence helicopter was not equipped with a cockpit voice recorder or a flight data recorder, nor was it required to be by the Canadian Aviation Regulations (CARs). The helicopter was, however, equipped with 2 systems that had the capability of recording flight data pertaining to the occurrence flight. These 2 systems are described in the following subsections.
1.11.2 Latitude Technologies flight tracking
A Latitude Technologies SkyNode S200 flight-tracking unit was installed in the occurrence helicopter in April 2013, in accordance with Supplemental Type Certificate SH06-4.Footnote 10 The S200 is a small aircraft-mounted system that records 5 flight-data parametersFootnote 11 at 1-second intervals for 2 minutes. At the end of the 2 minutes, the unit begins recording over the previous data. This occurs on a continuous loop so long as electrical power and the GPS (global positioning system) signal are supplied to the unit.
The S200 was recovered and flight data was retrieved from the unit.
1.11.3 Garmin Aera 660 global positioning system
The occurrence helicopter was also equipped with a Garmin Aera 660 GPS. This system presents flight instrumentation, position, navigation, and hazard avoidance information to the pilot on a 5-inch display. The GPS was not permanently mounted in the helicopter but was secured in the cockpit on a GPS mount.
The GPS was shipped to the TSB Engineering Laboratory in Ottawa, Ontario, where the data for the occurrence flight was extracted. Data points at variable intervals were recovered for the flight.
1.12 Wreckage and impact information
1.12.1 Accident site
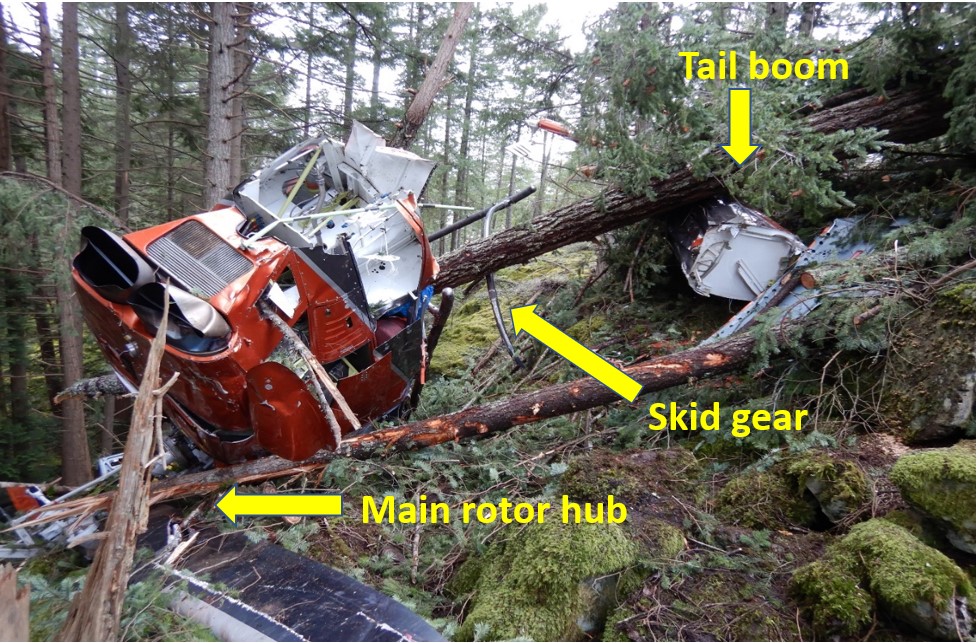
All of the helicopter debris was located within an 80-foot radius of the fuselage. The fuselage came to rest on its upper left side, ¾ inverted on the roof and with a nose-down attitude. The tail boom was severed at the mounts and sitting uphill from the fuselage, facing the opposite direction. The nose of the helicopter had sustained substantial impact damage, and the left cockpit area was partially crushed. The right horizontal stabilizer was crushed while the left stabilizer had minor damage. The remainder of the fuselage and tail boom remained largely intact with the major components (engines, main transmission, main rotor, and tail rotor) still installed in their normal positions. The skid gear had been partially torn from the fuselage after becoming hooked on a tree during the initial impact.
The main rotor hub was found intact with the 2 main rotor blades still attached. One main rotor blade was missing the outer 2/3 with 92 inches of the blade tip embedded in the ground approximately 35 feet northeast of the main rotor mast. The second main rotor blade was largely intact with the leading edge spar in one piece from the blade root to the blade tip.
A deformation on one side of the mast was measured at 0.055 inches deep where the mast had made significant contact with the static stop. The opposite side showed that contact had been made with the other static stop. The mast deformation observed is consistent with a mast bump,Footnote 12 which is the result of blade flapping in a low-G condition.
The No. 1 fuel valve switch was found to be broken and in the OFF position. The investigation was unable to determine the cause of the broken switch or the point at which the switch had been moved to the OFF position.
The tail rotor was attached to the tail boom and found intact (Figure 6). It was suspended over a cliff without any surrounding obstructions. Investigators observed the following damage indicating that the tail rotor was free-spinning during the flight:
- Both tail rotor blades had damage on the trailing edges near the blade tips.
- The vertical fin had 2 impact marks that were consistent with the impact of the tail rotor blade trailing edges.
- The tail rotor driveshaft cover was severed 15 inches from the aft end and the tail rotor aft driveshaft was severed 15 inches from the aft end. This is consistent with the main rotor blade striking the tail rotor driveshaft.

Continuity among the engine, transmission, and tail rotor assembly was verified (with the exception of the missing section of the tail rotor driveshaft).
1.12.2 Wreckage examination
1.12.2.1 Engines
The helicopter was equipped with 2 identical Pratt & Whitney Canada PT6T-3B turboshaft engines that were mounted side-by-side in the aircraft and connected to 1 common reduction gearbox that had a single output driveshaft to the main transmission.
After the accident, both engines (including engine accessories and the combining gearbox) were shipped to the Pratt & Whitney Canada facility in Saint-Hubert, Quebec, for further evaluation. This evaluation was supervised by the TSB. The engines were inspected and run individually and in dual mode. There were no findings from the engine examination that indicated an in-flight engine problem or anomaly had occurred.
The disassembly of the No. 2 engine indicated that it was not running when the aircraft impacted the terrain.
According to Pratt & Whitney Canada representatives who reviewed the accident details, if a helicopter rolls beyond 90° from vertical towards being fully inverted and the main rotor experiences a sudden load reduction that results in a main rotor overspeed, the engine governors will limit or reduce fuel flow to stop this overspeed and bring the main rotor back within limits.
1.12.2.2 Hydraulic system
The helicopter has 2 separate and independent hydraulic systems that provide hydraulic boost to the main rotor and tail rotor flight controls. Each hydraulic system is controlled by a switch located on the centre console. According to the RFM, “both hydraulic systems shall be operational prior to takeoff”Footnote 13 due to the excessive force required to move unboosted main rotor flight controls. The hydraulic system has 2 hydraulic pressure indicators (1 for each system). There is 1 warning light that illuminates on the caution panel if hydraulic pressure drops below the normal operating range in either hydraulic system.
Each system has an unpressurized reservoir mounted on the upper deck of the fuselage that uses gravity to provide hydraulic fluid to a variable delivery pump mounted on the main transmission. The No. 1 and No. 2 hydraulic pumps then deliver high-pressure fluid to the 3 main-rotor dual servoactuators and, in the case of the No. 1 pump, to the single tail rotor servoactuator. As a result, following a No. 1 hydraulic system failure, hydraulic boost to the tail rotor controls will be lost. Following a No. 2 hydraulic system failure, the main and tail rotor flight controls will continue to be hydraulically boosted by the No. 1 hydraulic system. If both hydraulic systems fail, all hydraulic boost to the flight controls will be lost. In the event that the helicopter is subjected to extreme flight attitudes, e.g. inverted or near -inverted, air could enter the system through the gravity-fed hydraulic pumps from their unpressurized reservoirs.
During the examination of the wreckage, both hydraulic system switches were found in the ON position. An inspection of the hydraulic pumps, filters, and hydraulic system fluid did not reveal any abnormalities.
The main rotor and tail rotor servoactuators were removed from the helicopter for inspection and bench testing. Due to excessive bending caused by the impact, the bench test was limited to 1 main rotor servoactuator and the tail rotor servoactuator, in which no significant anomalies were observed. The remaining 2 main rotor servoactuators were disassembled and visually inspected with no internal damage found. No anomalies were found during the testing.
1.12.2.3 Transmission
The main transmission uses the engine power to drive the main rotor and the tail rotor drive system. The transmission remained mostly in place throughout the accident sequence, but the right rear elastomeric vibration isolator mount and the 5th mount were found broken away from the fuselage.
The 5th mount damage was determined to be a result of impact with the ground.
The cracked portions of the right rear mount were forwarded to the TSB Engineering Laboratory for analysis. It was determined that this mount failure was most likely the result of impact forces and not likely to have been caused by an overstress condition while the helicopter was in flight.
1.12.2.4 Tail rotor drive system
The tail rotor drive system consists of 6 driveshaft sections, 4 hanger bearings, the intermediate gearbox (42°), and the tail rotor gearbox (90°). Flexible couplings located at each hanger bearing and gearbox compensate for tail boom flexing due to dynamic loads.
The tail rotor provides 2 essential functions: it produces a force that counteracts the torque generated by the main rotor, and it allows the pilot to steer the helicopter around the vertical axis. On a helicopter with a counter-clockwise rotating main rotor, like the Bell 212, a complete loss of tail rotor thrust will cause an uncommanded yaw to the right.
In this occurrence, the main rotor blades made contact with the tail rotor drive system, disabling the tail rotor driveshaft ahead of the intermediate gearbox and leaving the helicopter with a loss of tail rotor thrust. The missing pieces of the tail rotor driveshaft cover and driveshaft were not recovered.
As the pilots regained control of the helicopter following the initial loss of control, neither pilot was aware that the main rotor had disabled the tail rotor driveshaft. With the helicopter moving at high speed after the upset, very little yaw control was required because the vertical fin was doing much of the work to keep the helicopter from yawing. As the speed decreased, there was a greater demand for tail rotor thrust to maintain directional control.
1.13 Medical and pathological information
There was no indication that the performance of the pilots was degraded by fatigue or any other physiological or pathological factors.
1.14 Fire
There was no post-impact fire.
1.15 Survival aspects
1.15.1 Cargo restraint
A remote hook, longline, and several cargo nets were being carried inside the helicopter and were restrained before the flight. Several smaller items were placed in a milk crate secured to the floor in the back of the helicopter. Airspan Helicopters had installed the milk crate, which was commonly used by pilots to help contain smaller items in the cabin. The crate did not have a cover over it. During the occurrence, the loose items were thrown around the cabin; some entered the cockpit.
CARs paragraph 602.86(2)(b) states:
(2) No person shall operate an aircraft with carry-on baggage, equipment or cargo on board unless
[…]
(b) all of the equipment and cargo that are stowed in a passenger compartment are packaged or covered to avoid possible injury to persons on board; Footnote 14
1.15.2 Flight helmets
Both pilots were wearing flight helmets that had been manufactured within the last few years and had no pre-existing damage. Both helmets were significantly damaged in the occurrence.
These flight helmets effectively protected the pilots from head injury, which could have resulted from the items that were thrown around the cabin during the first loss of control or from the trees through which the helicopter descended during the accident sequence. The TSB has previously stressed the importance of wearing a helmet to prevent fatal injuries or to reduce the effects of non-fatal injuries to the head in an accident. Footnote 15 These effects may vary from confusion to complete loss of consciousness.
1.15.3 Seats and safety belts
The left seat was an original Bell 212 cockpit seat. It remained intact with no visible signs of damage, compression, or twisting. The right seat was a DART Aerospace Comfort Seat installed in accordance with Supplemental Type Certificate SH08-37. Footnote 16 The front of this seat was deformed downward, revealing that it had absorbed some of the compression forces as the aircraft settled in the trees. There were no visible signs of twisting or breakage of the seat frame.
The investigation determined that the pilots were wearing a 4-point safety belt. Footnote 17
Finding: Other
Wearing flight helmets and a 4-point safety belt reduced the severity of injuries to the pilots, who were able to egress unassisted from the aircraft quickly.
1.15.4 Emergency locator transmitter
The aircraft was equipped with a Kannad ELT model 406 AF-Compact that transmitted on frequencies 121.5 MHz and 406 MHz. The PIC, who was in the right seat, manually activated the ELT by turning the remote switch to the ON position before impact with the trees. The ELT transmission was received by the Canadian Mission Control Centre in Trenton, Ontario.
1.16 Tests and research
1.16.1 Comprehensive Program for the Theoretical Evaluation of Rotorcraft simulator
Bell Textron Inc. assisted in the investigation of this occurrence by using its Comprehensive Program for the Theoretical Evaluation of Rotorcraft (COPTER) simulator. The simulator is a physics-based computer model that captures numerous parameters for each simulation.
The Bell Textron Inc. team completed several computer-based flight simulations based on occurrence GPS data, weight and balance information, and forecast weather data. These simulations included several assumptions where the data, such as pilot inputs, were unknown.
The simulations were run from the point of the first loss of control, when lee effects caused the helicopter to pitch nose down and begin a rapid right roll. They demonstrated the following:
- a loss of tail rotor thrust increased the rolling of the fuselage along with a nose-down pitch
- the descent profile during the loss of control was achievable in the occurrence helicopter’s configuration
- the flight profile resulted in a low-G condition on at least 2 occasions
- the flight profile resulted in substantial blade flapping
1.16.2 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP038/2021 – NVM Data Recovery
- LP056/2021 – Transmission Mount Analysis
- LP098/2021 – Warning and Caution Lamps Analysis
- LP111/2021 – Witness Video Acoustic Analysis
1.17 Organizational and management information
Airspan Helicopters is a privately owned company providing commercial helicopter air services to the public. The fleet at the time of the accident consisted of 6 helicopters, including AS350, Bell 206, and Bell 212 helicopters.
The company employs approximately 15 people and operates helicopters from a main base located at CAP3. The primary area served by the company is western Canada, and the air services it provides are VFR air taxi and longline operations in accordance with CARs subparts 702 and 703.
The company uses a Type D operational control system.Footnote 18 The occurrence flight had an operational flight plan that was filed with a company flight follower.
The company also has a Transport Canada–approved maintenance organization with ratings for all non-specialized work for the types of aircraft operated.
1.17.1 Single-pilot helicopter operations
Operational flights conducted by the company are typically single pilot. Except for training, there are no company operating procedures for situations where 2 pilots are in the cockpit at the same time during a flight and where dual flight controls are installed. As stated in Transport Canada’s Approved Check Pilot Manual (TP 6533) “[n]otwithstanding an operator’s SOPs [standard operating procedures], the method of transferring control from one pilot to the other must be established.”Footnote 19,Footnote 20
A Notice of Proposed Amendment is under development by Transport Canada to mandate the use of SOPs in all single-pilot and two-pilot aircraft operated under Part VII of the CARs.
1.17.2 Airspan Helicopters mountain flying training
The Airspan Helicopters initial and recurrent training form in its company operations manual lists the following 3 items for mountain flying review: recce [reconnaissance], approach, and pads.Footnote 21
Airspan Helicopters also has a mountain flying training form, which is not included in the company operations manual. The form is part of its recurrent training program. The associated test flight has been intertwined with heli-ski recurrent training and focuses primarily on the skills required for heli-ski operations.
1.18 Additional information
1.18.1 Mountain flying
Mount Gardner on Bowen Island has a northeast/southwest orientation, creating a mountain ridge at 2388 feet ASL. With the winds blowing from the east/southeast at the time of the occurrence, this ridge formed an approximate 90° angle with the wind, creating eddies on the lee side of the mountain.
Transport Canada recommends the following prior to flying VFR in the mountains:
- Delay your flight when the winds at mountain-top level are greater than 30 knots
[…]
- Don’t try to out-climb downdrafts—your aircraft may not be able to. Turn out of the sinking air as soon as you can and locate the rising air (usually by turning upwind or downwind), which will be nearby
- Cross ridges at a 45-degree angle
- Stay away from violent turbulence from mountain waves and rotors; know what warning clouds look likeFootnote 22
In addition, the U.S. Federal Aviation Administration (FAA) makes the following recommendations for mountain flying:
- “It is suggested that you cross mountain passes at an altitude at least 1,000 feet above the pass elevation.”Footnote 23
- “Plan to be at that altitude at least three miles before reaching the ridge and stay at that altitude until at least three miles past it. This clearance zone will give you a reasonable safety zone to avoid the most severe turbulence and down drafts in windy conditions.”Footnote 24
- “To minimize the chance of encountering dangerous turbulence, mountain flying should not be attempted if the winds aloft forecast at mountain top levels are greater than 25 knots.”Footnote 25
1.18.2 Low-G conditions
A low-G condition is an undesired phase of aerodynamic flight in which the airframe is temporarily unloaded. The helicopter and occupants inside it may experience a temporary feeling of weightlessness. For 2-bladed teetering rotor systems, which rely on the tilting of the rotor disc for control, low-G conditions can be catastrophic.
The FAA Helicopter Flying HandbookFootnote 26 contains the following:
Helicopters rely on positive G to provide much or all of their response to pilot control inputs. The pilot uses the cyclic to tilt the rotor disk, and, at one G, the rotor is producing thrust equal to aircraft weight. The tilting of the thrust vector provides a moment about the center of gravity to pitch or roll the fuselage. In a low-G condition, the thrust and consequently the control authority are greatly reduced. […]
[H]elicopters with two-bladed teetering rotors rely entirely on the tilt of the thrust vector for control. Therefore, low-G conditions can be catastrophic for two-bladed helicopters. […]
[A]n abrupt forward cyclic input or pushover in a two-bladed helicopter can be dangerous and must be avoided, particularly at higher speeds. During a pushover from moderate or high airspeed, as the helicopter noses over, it enters a low-G condition. Thrust is reduced, and the pilot has lost control of fuselage attitude but may not immediately realize it. Tail rotor thrust or other aerodynamic factors will often induce a roll. The pilot still has control of the rotor disk, and may instinctively try to correct the roll, but the fuselage does not respond due to the lack of thrust. If the fuselage is rolling right, and the pilot puts in left cyclic to correct, the combination of fuselage angle to the right and rotor disk angle to the left becomes quite large and may exceed the clearances built into the rotor hub. This results in the hub contacting the rotor mast, which is known as mast bumping. […] Low-G mast bumping has been the cause of numerous military and civilian fatal accidents. It was initially encountered during nap-of-the-earth flying, a very low-altitude tactical flight technique used by the military where the aircraft flies following the contours of the geographical terrain. The accident sequence may be extremely rapid, and the energy and inertia in the rotor system can sever the mast or allow rotor blades to strike the tail or other portions of the helicopter.
Turbulence, especially severe downdrafts, can also cause a low-G condition and, when combined with high airspeed, may lead to mast bumping. […] During flight in turbulence, momentary excursions in airspeed, altitude, and attitude are to be expected. Pilots should respond with smooth, gentle control inputs and avoid overcontrolling. Most importantly, pilots should slow down, as mast bumping is less likely at lower airspeeds.
1.18.3 Human factors issues
Emergencies are stressful, high-workload situations in which people have limited time to process various types of critical information, make decisions, and adjust actions accordingly. Footnote 27 These increased stress levels and high workloads, can adversely affect a pilot’s ability to perceive and evaluate cues from the environment. Footnote 28 Having both a good situation assessment and situational awareness are critical for good decision making. Situational awareness is a construct that describes how humans perceive information, understand it, and make predictions about it, creating an awareness of the present situation about themselves.
1.18.3.1 Decision making
Information processing becomes part of decision making as decisions grow more complex. Classical or normative decision-making models are focused on making rational, optimal decisions, such as buying a house, and are often characterized by slow, analytical evaluation of options and selection of the optimal choice. In comparison, behavioural and naturalistic decision-making models are focused on how decisions are made in time-sensitive, dynamic, real-world settings. These models account for human cognitive limitations and are characterized by making decisions in routine, nonanalytical ways, comparing actions in terms of expected value or utility. Research shows that professionals in real-world settings use naturalistic decision making depending on their experience, the task, and the operational context. Footnote 29
Decision making, in this way, “fuses two processes: the way decision makers size up the situation to recognize which course of action makes sense, and the way they evaluate that course of action by imagining it.” Footnote 30 In these types of situations, decision makers recognize situations as typical and familiar and proceed to take action. They understand what types of goals make sense, what priorities to set, which cues are important, and what to expect next, as well as typical ways to respond in given situations. By recognizing a situation as typical, they also recognize a course of action likely to succeed. This strategy of decision making is extremely efficient and performed very quickly. However, a pilot may face a situation that is neither typical nor included in any procedures, standard operating procedures, or training they may have received.
The surprise and startle effect can also affect human performance and result in reactions ranging from being distracted to taking inappropriate action or making panicked decisions. The surprise and startle effect can be defined as a cognitive and emotional response to an unexpected situation arising from a disparity between what is expected and what is perceived. The effect tends to interrupt an action and focus a person’s attention on certain elements to the detriment of the overall situation, and may lead to inappropriate actions being taken.
Training is therefore important for pilots because it allows them to acquire the knowledge and skills necessary to fly an aircraft safely and effectively, especially under challenging conditions. Ongoing experience and regular practice also improve proficiency by reinforcing lessons learned.
1.18.3.2 Single-pilot crew resource management in helicopter operations
Humans are only able to process information from the environment and use it to make decisions if they detect that information and perceive it to be relevant. Effective communications are an important element in the decision-making process. One of the primary goals of crew resource management (CRM) training is to “enhance communication, interaction, human factors, and management skills of the crew members concerned”. Footnote 31
In 2020, to help pilots understand, prepare for, and manage potential degradation of a known or unknown situation, Transport Canada recommended that aerial work and air taxi operators conduct single-pilot resource management (SRM) training.
As described in Transport Canada’s Advisory Circular 700-042, Crew Resource Management,
SRM adapts concepts from CRM to the single-pilot environment. […] Current CRM training concepts include threat and error Management (TEM), which speaks to the identification and analysis of potential hazards; the implementation of appropriate strategies to handle threats; and the implementation of steps to avoid, trap, or mitigate errors before they lead to undesired consequences such as an undesired aircraft state. Footnote 32
The Advisory Circular also states that single-pilot CRM should be focused on areas relevant to the single-pilot and to the operation. It recommends that, among other topics, training should include situational awareness, workload management, decision making, and surprise and startle effect. Footnote 33
2.0 Analysis
In this investigation, there was no indication that any pre-existing helicopter system malfunctions or physiological conditions played a role in the occurrence. As a result, the analysis will focus on the environmental conditions at the time, the decision to depart and continue in those conditions, helicopter system limitations, unsecured objects, and emergency handling.
2.1 Weather
2.1.1 Turbulence and wind shear
Before departure, both pilots had checked the weather forecasts, which called for strong winds from the southeast, localized severe mechanical turbulence, and the potential for low-level wind shear. The visibility was good, and the only significant conditions were the turbulence and strong winds.
A low-pressure centre just north of Vancouver Island moving inland with associated warm and cold fronts produced strong outflow winds over Howe Sound. Winds in the area of the occurrence were variable both in speed and in direction because the air was forced around the islands in Howe Sound. In addition, the complex terrain surrounding Howe Sound and the wind direction were conducive to the production of lee effects.
Conditions at 2000 to 2500 feet above sea level (ASL) were very likely turbulent, with the potential for severe mechanical turbulence and low-level wind shear. These conditions may have been further complicated by the presence of convective clouds in the area, which may have provided an additional source of turbulence.
Finding as to causes and contributing factors
The combination of a low-pressure system, the associated cold front, and the geography of Howe Sound created conditions conducive to severe mechanical turbulence, lee waves, and low-level wind shear along the helicopter’s flight path in the vicinity of Bowen Island.
2.1.2 Decision to depart
At the time of departure, the winds at the Sechelt Aerodrome were around 15 knots and typical for the time of year. The graphic area forecast (GFA) showed a cold front passing through the Bowen Island area around 1000 and the potential for active weather en route. The Vancouver International Airport terminal area forecast called for diminishing winds later in the day. The pilots were aware of the forecast and prepared for a turbulent flight.
The planned longline work for the day would complete a multi-day project. The pilots’ consideration of the weather was focused on the longline work ahead. The flight from Sechelt Aerodrome to the work site was considered routine. The day before the accident, the second pilot had flown a similar route to the longline site without issue. The pilots decided that if they arrived on site and the weather was not suitable for longlining, they could wait for the better weather called for in the forecast.
Other aircraft were operating in and out of the Sechelt Aerodrome around the time that the pilots were preparing for their departure. This reinforced the pilots’ decision to depart because it was consistent with decisions made by other pilots.
Finding as to causes and contributing factors
The pilots were aware of the forecasted weather, low-level wind shear, and mechanical turbulence, but decided to continue with the day’s planned flights based on improving weather forecast later in the day, the desire to complete the operational flight, and the observation that other aircraft were operating around the Sechelt Aerodrome.
2.1.3 Active weather en route
As the flight progressed towards the destination, localized surface waves (“cat’s paws”) could be seen on the water indicating downdrafts near the Collingwood Channel. The helicopter had been travelling at an altitude of approximately 2600 feet ASL 2 minutes before the initial upset. As it moved across Howe Sound, it gradually, and likely unintentionally, descended. By descending to a height close to that of the peak of Mount Gardner (2388 feet ASL), the helicopter entered an area of hazardous wind and turbulence.
The aircraft was on Mount Gardner’s lee side, and, approximately 2 NM from the mountain ridge, it was at an altitude of approximately 2430 feet ASL. This ridge created dangerous eddies on its lee side. A large eddy called a “rotor” likely formed below the lee wave crests; however, the pilots were unaware of the severity of these lee effects.
Finding as to causes and contributing factors
After observing visual cues of strong downdrafts and low-level wind shear when approaching Collingwood Channel, the pilots modified their heading, altitude, and airspeed; however, they continued toward Bowen Island unaware of the severity of the lee effects there.
2.2 Low-G condition
The strong winds on the day of the occurrence, mixed with the complex terrain within the inlet, produced severe turbulence that resulted in low-G conditions and a loss of control. During the loss of control, the helicopter experienced extreme attitudes that exceeded the manoeuvring limitations outlined in the Bell Model 212 Rotorcraft Flight Manual (RFM).
A low-G condition occurs when the main rotor is temporarily unloaded from the forces that are applied during the flight. During this low-G condition, the lateral cyclic has little, if any, effect because the rotor thrust has been reduced. Pilots should respond with smooth, gentle control inputs and avoid overcontrolling. The investigation was unable to determine which control inputs were applied by the pilots during the low-G condition; however, aft cyclic was heavily applied at some point during the recovery attempt.
The examination of the wreckage found marks on the upper section of the rotor mast, which indicate that a mast bump occurred. This happens in flight when excessive blade flapping occurs and leads to contact between the main rotor hub and the rotor mast. Also, it was determined that the tail rotor drive system was cut by the main rotor blades at some point during the loss of control, leaving the helicopter with a loss of tail rotor thrust.
Severe turbulence and a low-G condition are 2 situations that can cause blades to flap enough to strike the tail boom. According to the Bell Textron Inc. Comprehensive Program for the Theoretical Evaluation of Rotorcraft (COPTER) simulator’s computer simulations for the flight, the helicopter entered a low-G condition at least twice during the first loss of control.
Finding as to causes and contributing factors
The helicopter entered an area of severe turbulence that led to low-G conditions and a loss of control that included extreme attitudes, that resulted in excessive flapping of the main rotor blades. As a result, the main rotor blades contacted and severed the tail rotor driveshaft, causing a loss of tail rotor thrust and yaw control.
2.3 Unsecured objects
Before departure, several small items had been placed in a milk crate without a cover. The milk crate was secured to the floor behind the right pilot seat, which was common practice at Airspan Helicopters.
During the first loss of control, the items from the milk crate were launched forward from the rear cabin and struck the pilots on their helmets. The visor cover and yellow visor on the helmet of the second pilot (the pilot flying, who occupied the left seat) was knocked down over his face, blocking his vision. With the pilot-in-command (PIC) also on the controls, the second pilot was able to let go of the flight controls momentarily to force the visor cover up off his face and out of his vision. The yellow visor remained down for the remainder of the flight.
A visor cover may create a serious hazard if it blocks a pilot’s vision in flight, particularly during an attempt to recover control of an aircraft. In this occurrence, having a second pilot likely played a role in the recovery.
Finding as to risk
If loose items are stowed, but not adequately secured, there is a risk that, in the event of an in-flight upset, the items will be thrown around the cabin or into the cockpit, possibly distracting the flight crew or injuring aircraft occupants.
2.4 Emergency handling
2.4.1 Hydraulic and engine malfunctions
During the first loss of control, the helicopter exceeded the manoeuvring limitations as outlined in the RFM. Once the control of the helicopter had been regained and the helicopter had returned to level flight, the pilots, who were both still on the controls, noticed that the anti-torque pedals had become stiff, the cyclic was slow to respond, and the hydraulic caution light was on.
The hydraulic system uses gravity to deliver hydraulic fluid to the hydraulic pumps. In this occurrence, it is likely that air was introduced into both of the hydraulic systems via the unpressurized hydraulic reservoir when the helicopter experienced extreme attitudes during the loss of control. As a result, the performance of the hydraulic system for all flight controls was likely degraded, leading to a lag in servoactuator response, increased feedback load on the controls from aerodynamic forces, and greater pilot inputs to achieve normal main rotor and tail rotor response.
At around the same time, the PIC observed the No. 2 engine out indication light illuminate and the engine shut down. Although the uncommanded engine shutdown was likely a result of the extreme attitude, the exact reason for it could not be determined.
It is likely that after the helicopter had experienced a sudden reduction in main rotor load that resulted in a main rotor overspeed, the fuel governors limited or reduced fuel flow in order to bring the main rotor speed back within limits, which resulted in a reduction of available engine power from the No. 1 engine.
Finding as to causes and contributing factors
The helicopter’s extreme attitude during the initial loss of control likely caused the hydraulic system to malfunction, the No. 2 engine to shut down in flight, and the No. 1 engine to reduce fuel flow (resulting in less power), which subsequently reduced the main rotor speed.
2.4.2 Loss of tail rotor driveshaft thrust
The tail boom was struck by the main rotor blades, causing the tail rotor drive shaft to be severed. Given the forward speed of the helicopter, the airflow over the vertical fin would have been sufficient to keep the helicopter aligned with the direction of travel. As the speed decreased, tail rotor thrust would have been required to maintain directional control. Since there was no tail rotor thrust being generated to counter the torque created from the main rotor system, the helicopter began to rotate, initiating a second loss of control.
The pilots initiated an emergency landing without knowing that they had no tail rotor thrust. The PIC communicated the tail rotor failure to the second pilot (pilot flying), who quickly reduced both throttles to idle and reduced the collective to slow the rotation. As tree contact was made, the second pilot pulled up on the collective in order to slow the descent and cushion the impact.
Finding as to causes and contributing factors
As the helicopter slowed for the emergency landing, yaw control was lost due to the absence of tail rotor thrust, and the helicopter collided with terrain.
2.4.3 Reaction to in-flight emergency
The aircraft system indications and flight control forces experienced by the pilots did not match any training scenario they had completed in the past. They encountered a novel situation, were therefore unprepared, and had very limited time to troubleshoot the situation as it unfolded.
Given the sudden forces and extreme attitude and altitude changes experienced by the helicopter, it is likely that the pilots experienced the effects of surprise and startle. The surprise and startle effect is a cognitive and emotional response to an unexpected situation arising from a disparity between what is expected and what is perceived.
The company operates only single-pilot helicopters and does not have any established procedures for 2-pilot operations. Normally, multi-crew operations have defined procedures in place to establish roles and responsibilities during normal and emergency operations, such as the transfer of aircraft control. The roles and responsibilities of pilots who have access to aircraft controls needs to be clear. Such procedures are not required by regulation for single-pilot operations, but from a crew resource management perspective, they reduce ambiguity created in decision making and command by defining roles and responsibilities.
In this occurrence, the 2 pilots each made inputs on the flight controls in an attempt to regain control of the helicopter; the investigation was unable to determine which inputs were effective and which were not.
Finding as to risk
When 2 qualified pilots fly a single-pilot helicopter with dual controls installed, ambiguity can arise in decision making and command if roles and responsibilities are not clearly articulated. In the event of an in-flight emergency or critical situation, there is an elevated risk of discoordination in the cockpit, resulting in a delayed response or the exacerbation of the in-flight emergency or critical situation.
3.0 Findings
3.1 Finding as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The combination of a low-pressure system, the associated cold front, and the geography of Howe Sound created conditions conducive to severe mechanical turbulence, lee waves, and low-level wind shear along the helicopter’s flight path in the vicinity of Bowen Island.
- The pilots were aware of the forecasted weather, low-level wind shear, and mechanical turbulence, but decided to continue with the day’s planned flights based on improving weather forecast later in the day, the desire to complete the operational flight, and the observation that other aircraft were operating around the Sechelt Aerodrome.
- After observing visual cues of strong downdrafts and low-level wind shear when approaching Collingwood Channel, the pilots modified their heading, altitude, and airspeed; however, they continued toward Bowen Island unaware of the severity of the lee effects there.
- The helicopter entered an area of severe turbulence that led to low-G conditions and a loss of control that included extreme attitudes, that resulted in excessive flapping of the main rotor blades. As a result, the main rotor blades contacted and severed the tail rotor driveshaft, causing a loss of tail rotor thrust and yaw control.
- The helicopter’s extreme attitude during the initial loss of control likely caused the hydraulic system to malfunction, the No. 2 engine to shut down in flight, and the No. 1 engine to reduce fuel flow (resulting in less power), which subsequently reduced the main rotor speed.
- As the helicopter slowed for the emergency landing, yaw control was lost due to the absence of tail rotor thrust, and the helicopter collided with terrain.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If loose items are stowed, but not adequately secured, there is a risk that, in the event of an in-flight upset, the items will be thrown around the cabin or into the cockpit, possibly distracting the flight crew or injuring aircraft occupants.
- When 2 qualified pilots fly a single-pilot helicopter with dual controls installed, ambiguity can arise in decision making and command if roles and responsibilities are not clearly articulated. In the event of an in-flight emergency or critical situation, there is an elevated risk of discoordination in the cockpit, resulting in a delayed response or the exacerbation of the in-flight emergency or critical situation.
3.3 Other findings
These items could enhance safety, resolve an issue of controversy, or provide a data point for future safety studies.
- Wearing flight helmets and a 4-point safety belt reduced the severity of injuries to the pilots, who were able to egress unassisted from the aircraft quickly.
4.0 Safety action
4.1 Safety action taken
4.1.1 Airspan Helicopters Ltd.
As a result of the accident, Airspan Helicopters Ltd. took the following actions:
- suspended operations and maintenance until it completed an all-staff debrief to discuss details and initial lessons learned;
- suspended Bell 212 operations until it completed a maintenance review;
- held a formal critical incident stress management session for personnel;
- developed a pre-flight risk assessment that includes specific thresholds for severe turbulence;
- completed an internal safety investigation in accordance with its safety management system policy;
- implemented new procedures for securing smaller items to ensure they are secure in flight; and
- created and distributed a safety memo to company pilots detailing:
- pre-flight turbulence analysis
- en route turbulence awareness/avoidance
- mitigating actions for turbulence.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .