Runway excursion during take-off roll
Air Creebec Inc.
de Havilland DHC-8-102, C-GTCO
Rouyn-Noranda Airport, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 23 January 2019, a de Havilland DHC-8-102 aircraft (registration C-GTCO, serial number 119) operated by Air Creebec Inc. was conducting a scheduled flight from Rouyn-Noranda Airport, Quebec, to Montréal/Pierre Elliott Trudeau Airport, Quebec, with 3 crew members and 6 passengers on board. At 2135 Eastern Standard Time, the aircraft began its take-off roll on Runway 26. The aircraft began to veer to the left and continued to do so until the left main landing gear rolled off the surface of the runway and hit a snow windrow 5 feet beyond the edge of the runway. The aircraft continued to veer to the left and came to rest in a compacted snowbank 40 feet from the runway. One of the passengers received minor injuries. The aircraft sustained substantial damage to the fuselage, landing gear, and propellers. The accident occurred during the hours of darkness, when visibility was reduced to approximately 2 statute miles in snow showers. The emergency locator transmitter did not activate.
1.0 Factual information
1.1 History of the flight
On 23 January 2019, at 1544,Footnote 1 a de Havilland DHC-8-102 aircraft operated by Air Creebec Inc. (Air Creebec), conducting flight Cree 926 with 3 crew members on board, took off from Timmins/Victor M. Power Airport (CYTS), Ontario. The flight was bound for Rouyn-Noranda Airport (CYUY), Quebec, where 6 passengers were going to board; the aircraft would then proceed with its scheduled flight to Montréal/Pierre Elliott Trudeau Airport (CYUL), Quebec. At 1619, when the aircraft landed at CYUY, the CYUY flight service station (FSS)Footnote 2 informed the crew that flow controlFootnote 3 was in effect at CYUL due to adverse weather conditions and that their take-off slot was 2230. Shortly afterward, the FSS changed the timeslot to 2045.
Snow was continuing to fall at CYUY, and the CYUY winter maintenance team was performing snow clearing operations, giving priority to clearing the snow from the active runway.
At 2012, the crew began boarding the 6 passengers for the flight to CYUL. The captain was the pilot flying (PF) and was seated on the left, while the first officer (FO) was the pilot monitoring (PM). At 2020, the flight attendant gave the passenger safety briefing, and the aircraft was de-iced with Type I de-icing fluid before receiving an application of Type IV anti-icing fluid.Footnote 4 The crew then started the engines. At 2035, the crew received clearance from the FSS for the instrument flight rules (IFR) flight to CYUL.
The crew also received the latest aircraft movement surface condition report (AMSCR) for Runway 26, which had been issued at 2018, indicating that the runway was covered with ¼ inch of snow over a width of 110 feet. The remaining 40-foot width was covered with 1 inch of snow. The report also indicated the presence of snow windrows on each side of the runway between the edge of the runway and the runway edge lights, specifically 5 feet from the runway edge lights and the edge of the runway.
The aircraft began to taxi toward Runway 26 for takeoff. The crew performed the AFTER START checklist and the TAXI checklist according to standard operating procedures (SOPs).Footnote 5
At approximately 2040, while the aircraft was on Taxiway A, near the threshold of Runway 26, the FSS informed the crew that there was a ground stopFootnote 6 at CYUL and it had to return to the CYUY apron. Once the aircraft had returned to the apron (at approximately 2045), the crew shut down the engines and deplaned the passengers. Shortly afterward, the FSS informed the crew that their new take-off slot for CYUL was 2145.
At 2123, the passengers boarded the aircraft; the flight attendant then gave the safety briefing. During this time, at the crew’s request, the de-icing team was once again applying Type I de-icing fluid to the aircraft.
At approximately 2128, the crew started the engines and advised the FSS that the aircraft was beginning to taxi. The FSS provided the crew with the same AMSCR as before for Runway 26, which had been issued at 2018, because it was still the most recent report.
At approximately 2135, the aircraft exited Taxiway A and headed toward the threshold of Runway 26 for takeoff.
At 2136:38, the aircraft reached the runway threshold and began its take-off roll without first coming to a stop. The aircraft was 17 feet to the left of the runway centreline, on a heading of 4° to the left of the runway centreline (Figure 1, position 1). Visibility was approximately 2 statute miles (SM) in snow showers. The crew could see the runway edge lights along the entire runway, but could not see the runway centreline markings, which were covered with snow.
Throughout the take-off roll, the aircraft maintained a heading of 4° to the left, but the crew did not notice that the aircraft was veering to the left, getting further and further away from the runway centreline.
At 2136:50, when the aircraft had reached a speed of approximately 80 knots, the PF realized that the aircraft was near the left edge of the runway. As soon as the aircraft reached 80 knots, 12 seconds after beginning its take-off roll, the left main landing gear rolled off the runway surface and hit the snow windrow 5 feet beyond the edge of the runway (Figure 1, position 2). The left wheel then lost speed rapidly and the aircraft spun approximately 5° to the left. The PF attempted to control the aircraft’s direction using the rudder pedals, and decided to reject the takeoff by reducing engine power.
At 2136:53, intending to grab both power levers with his right hand, the PF caught the right engine lever with his little finger, pushing it completely forward. At the same time, the PF only succeeded in grabbing the left engine lever and pulling it back completely. The asymmetric power made the aircraft veer even further to the left. The PF then tried to control the aircraft using the rudder pedals, but the nose wheel and right main landing gear also hit the snow windrow. The PF continued to try controlling the aircraft’s direction using the rudder pedals, but the aircraft continued to veer to the left. Approximately 5 seconds later, the aircraft hit a compact snowbank approximately 36 inches high about 40 feet beyond the edge of the runway, and spun rapidly to the left.
At 2137:01, the PF reduced power to the right engine.
At 2137:04, the aircraft came to a stop 3000 feet from the threshold and 200 feet to the left of the Runway 26 centreline, on a heading of 147° (Figure 1, position 3 and Figure 2). The PF then carried out the engine shutdown procedure.

Position legend:
1: Beginning of take-off roll.
2: Left main landing gear rolled off the runway surface.
3: The aircraft came to rest.

The captain advised the FSS of the runway excursion and gave the order to evacuate the aircraft, but then changed his mind when he noticed that there was no danger and everyone could remain inside the passenger cabin while waiting for the emergency response crew. The emergency vehicles arrived, then the passengers were deplaned using the main door and taken to the terminal in the emergency vehicles.
One of the passengers received minor injuries. The aircraft sustained substantial damage to the fuselage, landing gear and propellers. The inspection of the aircraft after the accident revealed no faults before the impact that may have caused the aircraft to veer during the take-off roll.
1.2 Injuries to persons
| Injuries | Crew | Passengers | Total number of persons on board | Other persons |
|---|---|---|---|---|
| Fatal | 0 | 0 | 0 | – |
| Serious | 0 | 0 | 0 | – |
| Minor | 0 | 1 | 1 | – |
| None | 3 | 5 | 8 | – |
| Total | 3 | 6 | 9 | – |
1.3 Damage to aircraft
When the aircraft hit the 36-inch compacted snowbank, sections of both propellers broke off and damaged each side of the fuselage. Also, the aircraft’s nose, belly and landing gear were damaged (Figure 3).

1.4 Other damage
Not applicable.
1.5 Personnel information
| Captain | First officer | |
|---|---|---|
| Pilot licence | Airline transport pilot licence (ATPL) | Commercial pilot licence (CPL) |
| Medical expiry date | 01 February 2020 | 01 June 2019 |
| Total flying hours | 12 500 | 1000 |
| Flight hours on type | 8000 | 300 |
| Flight hours on type in the last 90 days | 145 | 132 |
| Hours on duty prior to the occurrence | 9 | 7 |
| Hours off duty prior to the work period | 13.5 | 15.5 |
The flight crew was certified and qualified for the flight in accordance with existing regulations.
1.5.1 Captain
At the time of the accident, the captain had more than 12 years of experience with Air Creebec. He had accumulated approximately 10 500 hours as captain.
He had an airline transport pilot licence (ATPL), which was restricted because he had insulin-treated diabetes mellitus (ITMD). He also had a valid Category 1 medical certificate. The captain had undergone all of his medical exams, including an eye exam, and met all of the requirements for the annual medical recertification. Furthermore, on the day of the accident, the captain was accompanied by a pilot who was aware of his medical condition. Finally, measurements of his blood glucose level were within norms and therefore had no impact on his ability to function normally.
The captain had been on duty for approximately 9 hours straight at the time of the occurrence. The investigation did not find any indicators that the captain’s performance was degraded by fatigue or physiological factors.
1.5.2 First officer
The FO joined Air Creebec in 2016. While completing his pilot training, he began working on the apron. His initial pilot proficiency check as FO of the DHC-8-102 was conducted on 17 August 2018. At the time of the accident, he had accumulated approximately 1000 total flying hours.
He had been on duty for approximately 7 hours at the time of the occurrence. The investigation did not find any indicators that the FO’s performance was degraded by fatigue or physiological factors.
1.6 Aircraft information
| Manufacturer | de Havilland |
|---|---|
| Type and model | DHC-8-102 |
| Year of manufacture | 1988 |
| Serial number | 119 |
| Certificate of airworthiness issue date | 13 October 1988 |
| Total airframe time | 43 522.2 |
| Engine type (number of engines) | PW120A (2) |
| Propeller/Rotor type (number of propellers) | Hamilton Standard 14SF-7 (2) |
| Maximum allowable take-off weight | 34 500 lb |
| Recommended fuel type(s) | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A-1 |
Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. The weight and centre of gravity were within the prescribed limits.
1.7 Meteorological information
Weather conditions at CYUY were favourable for an IFR flight.
The aerodrome routine meteorological report (METAR) issued at 2100 for CYUY was:
- winds from 030° true (T) at 5 knots;
- visibility 2¼ SM in light snow;
- overcast ceiling at 3800 feet above ground level (AGL);
- temperature −10°C, dew point −11°C;
- altimeter setting 29.55 inches of mercury (inHg).
Three minutes later, at 2103, the following aerodrome special meteorological report (SPECI) was issued:
- winds from 030°T at 6 knots;
- visibility 3 SM in light snow;
- broken ceiling at 3800 feet AGL and overcast cloud at 6800 feet AGL;
- temperature −10°C, dew point −11°C;
- altimeter setting 29.55 inHg.
At 2135, as the aircraft was taxiing toward the runway, the snow showers were slightly heavier, with visibility reduced to approximately 2 SM. A second SPECI, issued at 2147, 10 minutes after the accident, reported:
- winds from 030°T at 6 knots;
- visibility 2 SM in light snow;
- vertical visibility 1300 feet AGL;
- temperature −10°C, dew point −11°C;
- altimeter setting 29.54 inHg.
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
1.10.1 General
The City of Rouyn-Noranda is responsible for CYUY’s management, operations and development. As an airport certificate holder, the City has implemented a safety management system (SMS) approved by Transport Canada (TC).
CYUY has a single paved runway, Runway 08/26, which is 7500 feet long and 150 feet wide. Two taxiways provide access to Runway 08/26. Taxiway A joins the threshold of Runway 26 directly while Taxiway B joins the runway 1500 feet from the threshold of Runway 26 (Figure 1).
1.10.1.1 Runway 08/26 markings
Runway 26 has several white painted markings that comply with TC’s Aerodrome Standards and Recommended Practices.Footnote 7 The runway threshold is marked with the number 26, which corresponds to the whole number closest to the tenth of the magnetic bearing of the runway centreline. This runway designation marking is located approximately 12 m (39 feet) from the runway threshold, centred on the runway centreline.
Runway 26 also has runway centreline markings, which consist of 8 evenly spaced longitudinal lines. These lines begin 12 m (39 feet) from the runway designation marking and are spaced 50 to 75 m (164 to 246 feet) apart along the full length of the centreline (Figure 4). At the time of the accident, the runway markings were covered with snow and was not visible to pilots.

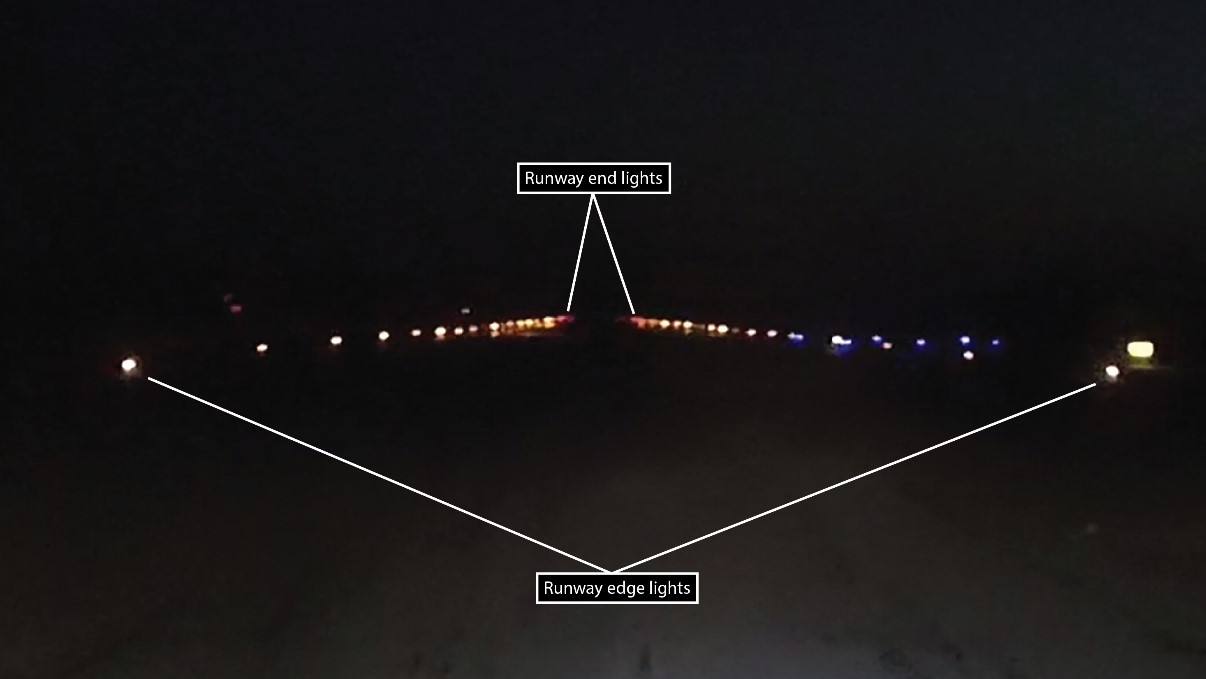
1.10.1.2 Airport lighting
Runway 26 is lit by runway lighting in accordance with Aerodrome Standards and Recommended Practices.Footnote 8
This lighting (Figure 5) consists of 1 row of runway edge lights on either side of the runway. They are raised fixed white lights, installed approximately 10 feet beyond the paved surface and spaced 200 feet apart. The lights are installed on opposite sides of the runway centreline, aligned at right angles to the runway centreline. The lighting also includes green threshold lights and red runway end lights. Also, the taxiways are lit by 2 rows of fixed blue lights installed on either side of the taxiway.
The evening of the accident, all runway edge lights were visible to pilots.
1.10.2 Snow clearing procedures at the Rouyn-Noranda Airport
The procedures found in the CYUY snow clearing manualFootnote 9 were developed in accordance with existing regulations and based on several advisory circulars published by TC.Footnote 10 As stipulated in the CYUY snow clearing manual, CYUY maintenance staff are responsible for runway inspections and maintenance, and AMSCRs. AMSCRs and Canadian runway friction index (CRFI) reports are available at all times during hours of operation, and on demand with 1 hour notice outside hours of operation.
The evening of the accident, the runway was maintained in accordance with procedures in effect at CYUY.
1.10.3 Flight service station
NAV CANADA operates an FSS at CYUY 24/7. The role of an FSS is to provide pilots with information on weather conditions, local traffic, winds, the altimeter setting, and any other information required. An FSS also controls the movement of maintenance vehicles that need to operate on the runway and taxiways and provides assistance in the event of an emergency.
1.11 Flight recorders
The aircraft was equipped with a flight data recorder (FDR) and a cockpit voice recorder (CVR).
The FDR contained 26.5 hours of flight data, including data for the occurrence flight. An analysis of this data helped to establish the aircraft’s speed and path, the point where the landing gear wheels entered the snow windrow, and the PF’s use of flight controls and power levers.
The CVR, which had a recording capacity of 120 minutes, contained high quality recordings for the occurrence flight.
1.12 Wreckage and impact information
The aircraft came to an abrupt stop in a compacted snowbank approximately 36 inches thick around 40 feet from the runway, on the left (Figure 1, position 3). The snowbank stopped the aircraft, which was headed toward a ditch located a bit further on. At the time of the impact, the right engine was producing full power and the left engine was not producing any. When the aircraft hit the snowbank, the tips of the propellers came into contact with the snowbank, and as a result, sections of the blades broke off and flew through the air, damaging the sides of the aircraft’s fuselage.
1.13 Medical and pathological information
Not applicable.
1.14 Fire
Not applicable.
1.15 Survival aspects
The captain did not evacuate the passengers from the aircraft because there was no risk of fire and the cabin had not sustained damages that would put the occupants’ lives in danger. Also, the aircraft had been damaged during the impact with the snowbank. The propeller tips that had been projected into the snow may have been dangerous during an evacuation. The passengers were therefore considered to be safer inside the aircraft while waiting for the emergency response team.
The deceleration forces were not sufficient to activate the emergency locator transmitter (ELT).
1.16 Tests and research
1.16.1 Observations on the runway
On the evening of 04 April 2019, the TSB conducted a series of observation exercises on Runway 26 at CYUY. The visual conditions during the exercises were not exactly the same as the conditions at the time of the accident: there was no precipitation; visibility was more than 6 SM; the runway centreline markings were visible since the runway was not covered with snow, but there was snow on the ground surrounding the runway. The exercise consisted of using an airport vehicle to retrace the departure path taken by the aircraft the evening of the accident and to trace the path taken by a standard departure along the runway centreline.
The purpose of this exercise was to assess the visual references on Runway 26 while allowing the TSB investigators to become familiar with the runway and the surrounding area. Video glasses were used to record what the observer was seeing.
After a series of trips on the runway, the TSB investigators were able to make the following observations:
- The runway edge lights contrast well with the background and provide effective visual references.
- The centre area at the end of the runway, where the lights converge, provides an effective centring visual reference.
- When an aircraft is in the initial take-off position, if the runway centreline markings are not visible, then it is more difficult to accurately determine the location of the centre of the runway and the runway orientation.
- In a take-off roll, the runway edge lights provide optical flow for ambient vision as long as pilots look far enough ahead along the runway alignment.
- When the optical flow is not symmetrical, the observer can visually perceive that the runway edge lights are no longer equidistant and take the appropriate measure to re-establish the proper path and follow the centreline.
- If, during the take-off roll, the deviation from the runway centreline increases, pilots can more easily detect the difference in the optical flow between the 2 sides, even if they are not looking far ahead.
These exercises enabled investigators to determine that runway edge lights provide pilots with an adequate visual reference that helps them to remain in the centre of the runway during night departures, even when the centreline markings are not visible, provided that the observer looks far enough ahead along the runway alignment. No deficiencies were identified in the runway visual references, or the lighting at the airport and in the surrounding area, that may have led to incorrect visual perceptions.
1.16.2 TSB laboratory reports
The TSB completed the following laboratory report in support of this investigation:
- LP010/2019 – FDR Download and Analysis
1.17 Organizational and management information
1.17.1 General
Air Creebec is a regional air carrier based in Val-d’Or, Quebec, which conducts scheduled and chartered flights to 16 destinations in Quebec and Ontario. These destinations are often airports that have runways with no centreline markings, and which face tough winter weather conditions.
The company operates 18 aircraft under subparts 703 (Air Taxi Operations), 704 (Commuter Operations) and 705 (Airline Operations) of the Canadian Aviation Regulations (CARs). The occurrence flight was conducted under Subpart 705.
Its fleet includes 2 Hawker Siddeley HS-748, 14 DHC-8-100 and 2 DHC-8-300.
1.17.2 Safety management system
As required under CARs Subpart 705, Air Creebec has a SMS that incorporates TC guidelines. This SMS covers all of the company’s activities pertaining to aircraft operations and associated equipment, as well as service-related activities.
1.17.3 Air Creebec standard operating procedures
1.17.3.1 Monitoring role of each pilot
In November 2014, following a study into the factors leading to ineffective flight path monitoring, the Flight Safety Foundation published 20 recommendations in A Practical Guide for Improving Flight Path Monitoring. According to this guide, monitoring consists of observing and interpreting an aircraft’s flight path, configuration, and the state of the automated systems and the other pilot. This means that the pilot must direct his/her attention to the right place at the right time, and take enough time to observe and interpret information, rather than simply glancing at it quickly.Footnote 11
Monitoring is required by both the PF and PM, regardless of the seat in which each is sitting. Monitoring must be carried out during all phases of flight, including before and after takeoff. It is often performed concurrently with other tasks such as operating aircraft controls, making data entries, and communicating with ATC.
To enhance pilot monitoring performance, the Flight Safety Foundation recommended that operators clearly define the monitoring roles and responsibilities of each pilot in its documents. The example below is given in the guide:
The PF’s primary responsibility is to control and monitor the aircraft’s flight path (including monitoring the flight guidance automated systems, if engaged.) The PF is secondarily responsible for monitoring non-flight path actions (radio communications, aircraft systems, other crew members and other operational activities) but he/she must never allow this to interfere with his or her primary responsibility, controlling and monitoring the flight path.
The PM’s primary responsibility is to monitor the aircraft’s flight path (including autoflight systems, if engaged) and to immediately bring any concern to the PF’s attention. The PM is secondarily responsible for accomplishing non-flight path actions (radio communications, aircraft systems, other operational activities, etc.) but he/she must never allow this to interfere with his or her primary responsibility, monitoring the flight.Footnote 12
Air Creebec defines the roles of the captain and FO in its company operations manual. However, the operator does not define the monitoring roles of the PF and PM in this manual or in its SOPs.
1.17.3.2 Take-off briefing
Monitoring Matters,Footnote 13 published by the United Kingdom’s Civil Aviation Authority (CAA), explains how a good briefing can promote effective pilot monitoring.
When briefing, the brief should both confirm the intentions for the phase of flight and provide questioning in order to confirm that the proposed plan is adequately understood. Make the briefing interesting, informative and concentrate on the salient points and use aide memoires. […]
A structured and interactive briefing fulfills two important goals:
- It provides the crew with an opportunity to:
- share a common action plan; and
- set priorities and share tasks — possibly mentally rehearse forthcoming monitoring tasks.
- It helps achieve effective teamwork —requiring the optimum use of:
- communication skills; and
- monitoring skills.Footnote 14
A briefing contributes to a common understanding of existing conditions and threats. If a take-off briefing is done properly, the 2 pilots should be able to concretely project how events will unfold during takeoff and they should have a shared mental model.
Air Creebec’s SOPs describe 2 types of take-off briefings: a full briefing to be completed before the first takeoff of the day; and an abbreviated briefing to be completed before subsequent takeoffs.
The PF must carry out the pre-takeoff briefing after receiving clearance for an IFR departure. The briefing must be done at the end of the TAXI checklist.
The occurrence flight was the crew’s 3rd takeoff of the day. According to the procedure described in Air Creebec’s SOPs, the crew should have at least completed an abbreviated briefing before takeoff, including the following points:
- aircraft weight;
- take-off flap settings;
- decision speed (V1), rotation speed (Vr), safety speed (V2), flap retraction initiation speed (Vfri) and climb speed (VClimb)(all speeds must be indicated by speed bugs);
- standard calls;
- review of authorized departure procedures and the procedure to be followed in the event of an immediate return.Footnote 15
However, no briefing was done before takeoff.
1.17.3.3 Take-off procedures
In its SOPs, Air Creebec provides flight crews with the following guidelines for the procedure to be followed during the take-off roll:
The PF will advance both power levers in a smooth and steady manner towards the calculated take-off torque. The *PNF will call “Through 80% torque” when observed and the PNF will adjust the calculated take-off torque.
The following call-outs will be used:
PF
“Check” [PF checks speed on
airspeed indicator]PNF*
“Spoilers Down” (N/A on -300)
“Autofeather Armed”
“Through 80% torque” (when observed)
“70 knots, power set” (when observed)
“V1, rotate” (at calculated V1)Footnote 16
*Air Creebec uses the expression “pilot not flying (PNF)” to designate the PM.
Air Creebec’s SOPs provide guidelines on how a pilot should position his or her hands during takeoff.
If the Captain is the PF, he/she will place his/her left hand on the control column to maintain wings level and elevator in the neutral position. Directional control is maintained through the rudder pedals. He/she will place his/her right hand on the power levers and advance them towards the calculated take-off torque and relax his/her grip at the call “Through 80% torque” from the First Officer. The First Officer will adjust and fine-tune the torque setting to the calculated take-off value. The Captain will leave his/her right hand on the power levers until the call “V1, rotate”, at which time he/she will place his/her right hand on the control column and rotate the aircraft into the Flight Director command bars.Footnote 17
1.17.3.4 Rejected takeoff
Some situations may require a rapid rejection of the takeoff. In order for a takeoff to be rejected quickly and safely, it is important for the PF to be able to maintain control of the power levers and pull them back at any time to reject the takeoff. The PF must therefore keep his or her hand on the power levers until V1 is reached.
1.18 Additional information
1.18.1 Processing visual information
Processing visual information includes focal (central) vision and ambient (peripheral) vision. Focal vision involves the recognition of objects and surfaces within the observer’s field of vision and there is an emphasis on detail. Ambient vision pertains to the observer’s spatial position in relation to the objects and surfaces in his or her field of vision and is therefore linked to spatial orientation. Ambient vision is better when a larger surface in the observer’s field of vision is stimulated and requires little or no cognitive effort.
Optical flow is the apparent movement of objects or surfaces in a visual scene caused by the relative movement between an observer and the objects and surfaces in his or her field of vision as the observer moves. The apparent position, speed and acceleration of an object in the visual scene depend on the distance of this object and the direction the observer is moving, as well as the observer’s point of focus in the visual scene.
For example, the driver of an automobile establishes and maintains the car’s position in the middle of a lane that has no markings in the centre by using the lines on the left and right edges of the lane. When the driver looks straight ahead, the lines on the edges of the lane and the peripheral objects produce an optical flow in the driver’s ambient vision, providing a visual reference that helps the driver to establish and maintain spatial orientation in the middle of the lane. At night, on roads with no lighting, the lines on the edges of the lane and the centre area where these lines converge provide the driver with a visual reference that produces an optical flow that is effective in maintaining the car in the middle of the lane.
When an aircraft taxis on a runway, the runway edge lights on either side produce an optical flow. However, since the lights on either side of the runway are much further from an aircraft than the borders of a lane are from a car, and pilots are sitting higher than automobile drivers, pilots must look much further ahead before they can get an effective optical flow. When the optical flow of the left and right edge lights is symmetrical—in other words, the distance between the lights on the left is the same as the distance between the lights on the right—the aircraft remains exactly in the centre of the runway (Figure 6).

However, when the optical flow is no longer symmetrical and the distance between the runway edge lights appears to decrease on one side and increase on the other, it means that the aircraft is deviating toward the side where the distance is decreasing (figures 7 and 8).


Night flight operations have their own particular threats due to the physiology of the human eye and the way it works. Flight crews must take these threats into consideration and manage them. At night, there are few external visual references, so spatial orientation is hindered. In this occurrence, other than the edge lights on either side of the runway, external visual references were limited because snow was covering the runway centreline markings and the snow-covered edges of the runway blended into the snow-covered surfaces beyond the runway. However, the runway edge lights are more visible at night than during the day, since the white lights contrast with the black background. This contrast is less pronounced in the daylight, especially against a snow-covered background.
1.18.2 Decision making and situational awareness
Decision making is a cognitive process used to choose a plan of action from several possibilities. The process involves identifying issues and threats and assessing options, taking into account the associated risks. Decision making is done in a dynamic environment, and consists of 4 steps: gathering information; processing information; making decisions; and acting on decisions. Decision making may be biased if the information gathering step is not done properly and if the information gathered is inaccurate.
Information processing is influenced by organizational and individual factors, operational circumstances and the experience of the person processing the information. Communication between the pilots of a flight crew is vital. Pilots must communicate available information to have the same understanding of the situation and be able to make the best decision.Footnote 18
Situational awareness is key to pilot decision making. Situational awareness is the perception of the elements in the environment, the comprehension of their meaning and the projection of their status in the future.Footnote 19 In a dynamic environment, situational awareness requires extracting information from the environment, integrating this information with relevant internal knowledge to create a coherent mental picture of the current situation, and using this picture to anticipate future events.Footnote 20
Shared situational awareness Footnote 21,Footnote 22 between the pilots of a flight crew depends on the extent to which the respective situational awareness of each pilot is similar. Flight crew members who have a shared situational awareness can anticipate and coordinate their actions and therefore act with cohesion and efficiency.
1.18.3 Trans-cockpit authority gradient
Optimum trans-cockpit authority gradient means that there is coherence between pilots on the same aircraft. It is well known that a too-strong or too-weak authority gradient between crew members can be a barrier to effective crew resource management (CRM).Footnote 23 An authority gradient is attributable to differences between the pilots, such as age, experience, rank of the crew members, and the manner in which one or both crew members explicitly or implicitly place emphasis on these differences. A gradient may be too weak, as in the case of 2 pilots with the same ratings and the same degree of experience, or too strong, as in the case of an experienced chief pilot working with an inexperienced FO. In circumstances such as those, there is a risk of lowered coherence between the crew members and reduced crew effectiveness, which increases the risk of an error going undetected and/or uncorrected.
In the case of flight Cree 926, the FO was 20 years younger than the captain. He had approximately 5 months’ experience as a commercial pilot and approximately 1000 total flying hours, while the captain had approximately 23 years of experience as a commercial pilot and more than 12 500 total flying hours.
The evening of the accident, the PM did not believe that it was necessary to monitor the departure path or to double-check the captain’s actions because the latter had much more experience. In contrast, the PF felt obliged to monitor the PM’s actions quite closely, since the PM was not very experienced, which took the PF’s attention away for longer from what was happening outside of the cockpit.
1.18.4 Complacency
When pilots routinely fly the same routes to the same destinations, their performance can become automatic. They may pay less attention to detail and become complacent. Complacency results from a state of overconfidence, repetition of action, contentment with the status quo, familiarity, and boredom. It is associated with experience and confidence, both found in pilots with a high number of flight hours.
Pilot complacency can also impair the ability to maintain situational awareness, and has been implicated as a contributing factor in several aviation incidents and accidents.Footnote 24 When pilots receive information about the environment that they expect to receive, they tend to react quickly and without errors. However, when they receive information that is contrary to their expectations (and their situational awareness), their performance tends to be slow or inappropriate.Footnote 25
In this occurrence, the captain had conducted numerous flights between CYTS and CYUY over the past 10 years.
1.18.5 Medical condition: diabetes mellitus
Diabetes mellitus is a metabolic condition in which the blood contains abnormally high levels of sugar (glucose), due to an inability to adequately respond to insulin. If the diabetes mellitus needs to be treated by insulin injections, then it is referred to as insulin-treated diabetes mellitus (ITDM).
One of the major considerations in medically certifying diabetics who are insulin treated or who require oral hypoglycemic agents is the risk of subtle or sudden incapacitation, most likely caused by hypoglycemia.
Although hyperglycemia and hypoglycemia are both concerns in aviation, hypoglycemia would likely precipitate pilot incapacitation. Hypoglycemia is usually considered to be a blood glucose concentration in the range below the level at which symptoms could be expected to occur. Hypoglycemia may result from one or more of the following: the blood contains too much insulin or insulin-producing medication; the blood contains too little glucose; the person is over-expending their energy.Footnote 26
1.18.5.1 Medical certificate for pilots with insulin-treated diabetes mellitus
Before January 2019, TC did not issue Category 1 medical certificates to new ITDM applicants,Footnote 27 but it did renew Category 1 medical certificates for ITDM pilots. In January 2019, TC began issuing Category 1 medical certificates to new ITDM applicants using the same assessment criteria as those applicable to the renewal of Category 1 medical certificates for ITDM pilots.
To obtain a Category 1 medical certificate, an ITDM pilot must undergo an annual medical exam, for which the criteria are described in TP 13312Footnote 28,Footnote 29 published by TC. These assessment criteria include medical screening, annual recertification requirements and medical certificate restrictions. These restrictions include mandatory blood glucose monitoring while in flight and the mandatory presence of another pilot who has received incapacitation training (regardless of the reason for the incapacitation) and does not personally need to be accompanied.
Only pilots demonstrating a low risk of hypoglycemia may be considered by TC for a restricted medical certificate. Along with the medical certificate, an ITDM pilot receives a protocol that must be followed before and during the flight to manage his or her blood glucose levels (Appendix A).
ITDM pilots also receive a letter stating the conditions to be met. Failure to meet these conditions will render their licence invalid. In this occurrence, the pilot had received a letter stating the following conditions:Footnote 30
- The pilot must be accompanied by another pilot who holds an unrestricted, medically valid pilot licence with the appropriate category, class and rating for the intended flight.
- The accompanying pilot must have had incapacitation training.
- The aircraft must be equipped with dual controls.
- In the case of a commercial flight, the pilot must have informed his or her employer of the above conditions.
- The pilot must abide by the blood glucose management protocol before and during the flight.
1.18.5.2 United Kingdom guide for the medical certification of pilots with diabetes mellitus
As indicated in TC’s Pilot IncapacitationFootnote 31 brochure, a pilot holding a licence with a medical restriction requiring that he or she be accompanied by another pilot may be at increased risk of incapacitation compared with a pilot who does not have this medical restriction.
Mental or physical impairment can have a serious impact on flight safety. That is why the United Kingdom’s Civil Aviation Authority published a guide explaining its policy for the medical certification of pilots with diabetes. The guide also provides information for pilots, instructors, examiners and employers, including the following:
The pilot must brief the other members(s) of the flight crew (and other members of the crew as necessary) before each flight on:
- The reason for blood glucose tests
- How the blood glucose test is done
- When blood glucose tests are required […]
- Actions to be taken in the event of a blood glucose test outside of the acceptable range (below 5 or above 15 mmol/l)
- Whether, when and how insulin will be used during the flight duty period.
- Possible symptoms of low or high blood glucose […].
- Actions to be taken by the pilot if a test is ‘out of range’.Footnote 32
The guide also explains the responsibilities of the operator.Footnote 33 The operator
will need to ensure all additional operational procedures and information is promulgated to all pilots in the fleet of a pilot with insulin-treated diabetes. […] [F]light crew who have any concerns about flying with another pilot using a needle and syringe on the flight deck […] have the opportunity to raise these concerns.
TC also publishes the Handbook for Civil Aviation Medical Examiners (TP 13312), which states the medical standard for the certification of pilots with various medical conditions. Part of this document presents guidelines for the assessment of medical fitness in Canadian pilots, flight engineers, and air traffic controllers with diabetes mellitus. TC is reviewing this handbook as it currently contains information that is no longer applicable.Footnote 34
However, there is no handbook addressing the responsibilities of operators in Canada.
1.18.6 Crew pairing
Section 705.106 of the CARsFootnote 35 stipulates that no air operator shall permit a person to act as a member of a flight crew unless he or she “holds the [valid] licence, ratings and endorsements required” for the flight. If 2 pilots with a licence stipulating the restriction that they must be accompanied by a pilot without a similar restriction are paired for a flight, their respective licences are not valid since they do not meet the established conditions. In the occurrence flight, the PF had given Air Creebec the letter he had received from TC stating that he needed to be accompanied by a pilot who had taken incapacitation training. All Air Creebec pilots receive this training. However, for crew assignments, Air Creebec did not take into account the need to be accompanied by a pilot without a licence restriction. In this occurrence, there was nothing to impede this crew pairing since the accompanying pilot had no licence restriction.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
The aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures, and no mechanical failures that may have contributed to the occurrence were identified. The flight crew held the licences and ratings required to conduct the flight in accordance with existing regulations, and there was no indication that fatigue had reduced the crew’s performance. In order to understand why the aircraft overran the runway during the take-off roll, the analysis will focus on:
- the take-off briefing;
- the deviation from the path during the take-off roll;
- the flight path monitoring;
- the rejected-takeoff procedure.
The investigation also examined the following points, even though they did not play a direct role in the accident:
- insulin-treated pilots with diabetes mellitus (ITDM) and crew resource management (CRM);
- crew pairing.
2.1 Take-off briefing
Before beginning takeoff, the pilot flying (PF) must give a briefing to establish priorities, share tasks between the 2 pilots and create a shared mental model.
The abbreviated take-off briefing permitted by the operator was not carried out for the first takeoff on the evening of the accident, nor for the subsequent takeoff, which led to the accident.
Having conducted several takeoffs from CYUY, the PF possibly relaxed his vigilance and did not feel the need to repeat all of the actions and information. It is true that information and conditions may be similar from one flight to the next; however, the take-off briefing serves purposes other than simply repeating the same information. It also serves to establish priorities and direct pilots’ attention to the key points.
The evening of the accident, coordination between the pilots in the execution of the takeoff was not optimal. Also, given that the pilot monitoring (PM) did not have much experience, a briefing may also have helped him to mentally repeat the monitoring tasks to be completed during the take-off roll.
If pilots do not carry out a take-off briefing, they may not have a shared mental model of the actions that must be taken during the takeoff, increasing the risk of an accident.
2.2 Deviation from the path during the take-off roll
Given that Air Creebec serves many aerodromes where the runway has no centreline markings, the captain had enough experience to conduct a takeoff on such a runway. At night, with no visual references on either side of the runway, and with no runway markings visible on the snow-covered runway, the runway edge lights and the centre area at the point where the 2 rows of edge lights converge provide acceptable visual references for positioning the aircraft close to the centre of the runway on a heading close to the runway heading. It is possible for an aircraft to begin accelerating on takeoff while it is not exactly in the centre of the runway or exactly aligned on the runway heading. However, if the pilot looks far enough ahead for long enough during acceleration, the visual references produce a perceptible optical flow that enables the pilot to maintain the aircraft in the centre of the runway on the desired heading and to detect deviations from the centre of the runway.
In this occurrence, the pilot had positioned the aircraft 17 feet to the left of the runway centreline, on a heading of 4° to the left of the runway alignment. This heading was maintained without being corrected for approximately 12 seconds, until the left main landing gear hit the snow windrow.
Good spatial orientation begins with perception of external visual references to determine the current position, then anticipation of future positions by assimilating information pertaining to the speed, acceleration and direction of objects and surfaces in the observer’s field of vision. The runway edge lights and the centre area where the 2 rows of edge lights converged were sufficient to provide the crew with visual references that would help them to detect a deviation from the centre of the runway. However, the PF did not look far enough ahead for long enough to notice that the aircraft was deviating to the left before veering off the runway.
2.3 Flight path monitoring
According to the Flight Safety Foundation, the PM’s primary role during all phases of flight, including takeoff, is to monitor the aircraft’s path and immediately warn the PF if a deviation is detected.Footnote 36 Furthermore, if there is insufficient time to warn the PF, the PM must be prepared to act quickly if there is a deviation from a procedure or the flight path, or if the PF becomes incapacitated.
Although the PM does not handle the flight controls directly, he or she plays a crucial role in the execution of a takeoff. According to Air Creebec’s standard operating procedures (SOPs), the PM must check that the spoilers are retracted and the autofeather system is activated; once the aircraft has reached 80% torque, the PM must call “Through 80% torque” and set power to take-off power; once a speed of 70 knots has been reached, the PM must call “70 knots, power set”; finally, once the decision speed (V1 ) has been reached, the PM must call “V1, rotate”.Footnote 37 Given that takeoff occurs quickly, the PM must direct his or her attention to the right place at the right time and spend enough time monitoring the flight’s progress and completing all of the tasks required for the take-off roll.
The evening of the accident, the PM completed all of his tasks and made all of the standard calls during the take-off roll. However, given that the PM was not looking out the window to monitor the aircraft’s path, he did not notice the deviation and was therefore unable to help the PF correct the deviation in the path during the take-off roll.
According to A Practical Guide for Improving Flight Path MonitoringFootnote 38 published by the Flight Safety Foundation, the monitoring roles and responsibilities of the PF and PM must be clearly defined in the operator’s SOPs in order to improve pilot monitoring performance. The monitoring roles and responsibilities of the PF and PM are not defined in Air Creebec documents.
If the roles and responsibilities of the PF and PM are not well defined, monitoring may not be effective, increasing the risk that an aircraft’s deviation from its path may fail to be detected and corrected.
The lack of monitoring effectiveness between the crew members on the evening of the accident may be linked to a strong authority gradient between the PF and PM. On one hand, the PM did not believe that it was important to monitor the departure path since the PF was highly experienced. On the other hand, the PF felt obliged to closely monitor the actions taken by the PM, who was not very experienced, which diverted the PF’s attention longer toward what was happening inside the cockpit. The strong authority gradient between the pilots reduced the effectiveness of monitoring, which resulted in a failure to detect and correct the deviation from the departure path.
2.4 Rejected-takeoff procedure
When the left main landing gear hit the snow windrow, the PF decided to reject the takeoff. However, during the takeoff-rejection procedure, the PF accidentally caught the right engine power lever with his finger, pushing the lever completely forward, and placed only the left lever in the idle position, which produced a significant dissymmetry in the torque and accentuated the deviation from the path, resulting in the runway excursion.
Since the PF was able to place only 1 power lever in the idle position, it is highly likely that he did not have his right hand on the levers, contrary to what is stated in SOPs. Consequently, he was not ready to quickly and safely reject the takeoff.
2.5 Pilots with insulin-treated diabetes mellitus
To mitigate the risk of incapacitation by ITDM pilots, Transport Canada (TC) issues pilot licences with restrictions requiring mandatory blood glucose monitoring while in flight and the presence of an accompanying pilot who has received incapacitation training and does not personally need to be accompanied. Furthermore, TC requires that ITDM pilots notify the operator of the restriction on their licence.
However, neither the ITDM pilot nor the operator is required to inform the other crew members of the pilot’s medical condition, the elevated risk of incapacitation, or the blood glucose management protocol that needs to be followed before and during the flight. If the other crew members have not been informed, they may be surprised and uncomfortable at the sight of the pilot testing his or her blood glucose level or taking medication during the flight. This undesirable situation could raise questions and cause stress for crew members who have not had an opportunity to become familiar with the situation and raise their concerns. This situation could be a barrier to crew performance, which is primarily based on communication, coordination and cohesion between pilots. Furthermore, although there is a procedure to follow if the pilot becomes incapacitated, it is preferable to inform the accompanying pilot in advance that the other pilot’s state of health might affect performance, so that the accompanying pilot can be better prepared to take action as necessary. The United Kingdom’s guide for the certification of insulin-treated pilotsFootnote 39 requires that, before each flight begins, ITDM pilots must inform the other members of the flight crew of the situation and the actions to be taken, if necessary (see section 1.18.5.2 of this report).
On the occurrence flight, the first officer was aware of the captain’s medical condition, but had not been told what actions to take, if necessary.
If the accompanying pilot is not informed of the other pilot’s state of health before the flight, the accompanying pilot will be less prepared to take rapid and appropriate action as necessary, which could impact flight safety.
2.6 Crew pairing
TC recognizes that a pilot with a known medical condition that necessitates a restriction on the pilot’s licence requiring the presence of an accompanying pilot has a higher risk of becoming incapacitated than a pilot who does not have such a requirement. Lowered physical or mental faculties may have serious consequences for flight safety.
To reduce risks, TC requires pilots with certain known medical conditions such as ITDM to be accompanied by a pilot who does not require an accompanying pilot as a condition of their licence. If this criterion is not met, the pilot’s licence is considered to be invalid and the protection put in place by TC to reduce risks in the event of pilot incapacitation is removed.
The investigation was unable to determine whether all operators in Canada were taking into consideration a pilot’s need to be accompanied when pairing crew members for a flight.
If operators do not take into account the restrictions associated with pilots’ licences when assigning crew members to a flight, they risk pairing 2 pilots who both have a restriction associated with their licence requiring that they fly with an accompanying pilot, which eliminates the protection put in place by TC to reduce risks in the event of pilot incapacitation.
3.0 Findings
3.1 Findings as to causes and contributing factors
These are conditions, acts or safety deficiencies that were found to have caused or contributed to this occurrence.
- The pilot flying did not look far enough ahead for long enough to notice that the aircraft was deviating to the left before veering off the runway.
- Given that the pilot monitoring was not looking out the window to monitor the aircraft’s path, he did not notice the deviation and was therefore unable to help the pilot flying correct the deviation in the path during the take-off roll.
- The strong authority gradient between the pilots reduced the effectiveness of monitoring, which resulted in a failure to detect and correct the deviation from the departure path.
- During the takeoff-rejection procedure, the pilot flying accidentally caught the right engine power lever with his finger, pushing the lever completely forward, and placed only the left lever in the idle position, which produced a significant dissymmetry in the torque and accentuated the deviation from the path, resulting in the runway excursion.
- Since the pilot flying was able to place only 1 power lever in the idle position, it is highly likely that he did not have his right hand on the levers, contrary to what is stated in the standard operating procedures. Consequently, he was not ready to quickly and safely reject the takeoff.
3.2 Findings as to risk
These are conditions, unsafe acts or safety deficiencies that were found not to be a factor in this occurrence but could have adverse consequences in future occurrences.
- If pilots do not carry out a take-off briefing, they may not have a shared mental model of the actions that must be taken during the takeoff, increasing the risk of an accident.
- If the roles and responsibilities of the pilot flying and pilot monitoring are not well defined, monitoring may not be effective, increasing the risk that an aircraft’s deviation from its path may fail to be detected and corrected.
- If the accompanying pilot is not informed of the other pilot’s state of health before the flight, the accompanying pilot will be less prepared to take rapid and appropriate action as necessary, which could impact flight safety.
- If operators do not take into account the restrictions associated with pilots’ licences when assigning crew members to a flight, they risk pairing 2 pilots who both have a restriction associated with their licence requiring that they fly with an accompanying pilot, which eliminates the protection put in place by Transport Canada to reduce risks in the event of pilot incapacitation.
4.0 Safety action
4.1 Safety action taken
4.1.1 Air Creebec
Air Creebec uses an automated flight and crew management system which automatically pairs pilots for flights. This system was already preventing the pairing of certain crew members based on selected criteria. The requirement for certain Air Creebec pilots to have to fly with an accompanying pilot has been added to the list of criteria. Consequently, 2 pilots with the same restriction can no longer be paired on the same flight.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Blood Glucose Management Protocol for Insulin-treated Pilots with Diabetes Mellitus (Source: Transport Canada)
While exercising the privileges of any licence or permit you must comply with these conditions:
- You must maintain the appropriate supplies for blood glucose management, which shall include:
- a reliable calibrated glucose meter with a memory chip and blood sampling equipment;
- 10 g portions of readily absorbable carbohydrate (appropriate to the duration of flight).
- Your BG [blood glucose] must be greater than 6.0 mmol/L, but not greater than 15 mmol/L within the 30 minutes immediately prior to flight. Your BG must then be monitored every 60 minutes during flight. If the blood glucose falls below 6.0 mmol/L then you must ingest 10 g carbohydrate.
- If, for operational reasons, an in-flight 60 minute BG measurement cannot be made, then you must ingest 10 g carbohydrate, however, this shall not be done for two consecutive 60 minute intervals without an actual BG measurement.
- You shall measure your BG 30 minutes or less prior to landing and if it is below 6.0 mmol/L then you must ingest 10 g carbohydrate.
- If your blood glucose should ever exceed 15 mmol/L during flight then you must cease caloric intake until after retesting. You should consult your Civil Aviation Medical Examiner or Aviation Medical Officer as soon as practicable to determine whether your condition might impair your ability to exercise the privileges of your licence safely. When flying as a single pilot you must land as soon as safely possible if your blood glucose should ever exceed 15 mmol/L.