Loss of power and collision with trees
Ridge Rotors Inc.
Bell 206B (Helicopter), C-GHHU
Fox Creek Airport, Alberta, 12 nm SW
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 05 September 2016, the Ridge Rotors Inc. Bell 206B Jet Ranger helicopter (registration C‑GHHU, serial number 2196) was operating on a mountain pine beetle survey flight originating from Whitecourt Airport, Alberta (CYZU), during daylight hours, with the pilot and 2 surveyors on board. At 1520 Mountain Daylight Time, approximately 12 nautical miles southwest of Fox Creek Airport, Alberta (CED4), the engine lost all power while flying approximately 160 feet above ground level, and the helicopter lost altitude and collided with trees. The pilot was seriously injured. One surveyor received minor injuries and the other received fatal injuries. The helicopter was substantially damaged. There was no post-impact fire, and no dangerous goods were on board. The surviving surveyor exited the helicopter and called 911 on a personal cellphone. The pilot was evacuated by air ambulance. The 406‑megahertz emergency locator transmitter activated and the signal was received by the Cospas-Sarsat search‑and‑rescue satellite system.
1.0 Factual information
1.1 History of the flight
On 04 September 2016, the day before the occurrence, the Ridge Rotors Inc. (Ridge Rotors) Bell 206B Jet Ranger helicopter, registration C‑GHHU, was operating on a mountain pine beetle survey (MPBS) flight originating from Whitecourt Airport, Alberta (CYZU). At approximately 2000,Footnote 1 C-GHHU landed at the Ridge Rotors helipad, located at CYZU, upon completion of the daily survey flights. The occurrence pilot conducted the engine shutdown sequence, as per the Ridge Rotors checklist, including the rotor-low-revolutions per minute (rpm) system check. This procedure requires the collective lever to be raised from the fully down position, so that the rotor-low-rpm warning horn can activate. The engine-out warning horn activated at N1Footnote 2 below 55%. When the engine-out warning horn operation had been verified, the pilot pulled the caution circuit breakerFootnote 3 out, in accordance with the company checklist, to silence the warning horn.
Once the helicopter was shut down and secured, the operations manager refuelled it using the Ridge Rotors fuelling trailers. The total quantity of fuel on board after refuelling was approximately 86 U.S. gallons (USG). Upon completion of that task, the pilot departed the airport and ended the duty day.
On 05 September 2016, the day of the accident, the pilot of C-GHHU arrived at the helipad at approximately 0700 and conducted flight planning. During this time, the pilot installed the dual flight controls, to allow the surveyors to follow along on the controls. The survey area was located 44 nautical miles (nm) from CYZU, or 30 minutes’ flying time (Figure 1).

At approximately 1222, after a delay of several hours due to poor weather, the pilot of C‑GHHU initiated the engine-start sequence. The company engine-start checklist called for the caution circuit breaker to be reset after the engine stabilized at 60% to 62% N1. It is likely that the circuit breaker was not reset at this time. Additionally, the checklist required that all circuit breakers be checked following the control and engine checks at 70% N1. It is likely that the caution circuit breaker was not reset at this time either.
At 1228, C-GHHU departed CYZU and transited to the survey area. The pilot was seated in the front right-hand seat, 1 surveyor was seated in the front left-hand seat, and the other surveyor was seated in the rear forward-facing seat. C-GHHU was equipped with dual flight controls. During the transit flight, while the pilot‑in‑command controlled the helicopter, the pilot allowed the surveyor seated in the front left seat to follow the pilot on the controls. It is unknown how long this continued. There are no requirements in the rotorcraft flight manual (RFM), the Canadian Aviation Regulations (CARs), or the company operations manual requiring the removal of dual flight controls for non-training flights.
At 1300, C-GHHU arrived at the survey area and began to conduct the required survey flying. Another Ridge Rotors Bell 206B helicopter, C-GKMS, was also conducting survey operations within the same survey area. Both helicopters flew a north–south survey pattern.
The survey was laid out in lines that ran north to south in a specific block of forest. The lines were 32 nm in length and spaced 800 m apart. The helicopter would fly a line at 120 to 180 feet above the treetops and at 60 mph, while each of the surveyors was tasked with observing an area of 400 m on either side of the helicopter.
At 1448, after 2 hours and 20 minutes of surveying, C-GHHU landed on a gravel barFootnote 4 by the Little Smoky River for a rest break. The engine power was brought down to flight idle, and the pilot remained at the controls. The pilot and the surveyor in the front left-hand seat discussed the fuel remaining. The pilot indicated that 30 USG of fuel remained, which would allow for about 1 hour of flight, including reserve fuel. From the surveyor’s perspective, the fuel quantity gauge appeared to indicate approximately 24 USG. The pilot decided to continue with the surveying operations before proceeding to the company fuel cache located at Fox Creek Airport, Alberta (CED4), approximately 12 nm northeast of the survey area.
After 20 minutes on the ground,Footnote 5 the surveyors switched seats, and engine power was increased to 100% main-rotor rpm (NR). At 1508, C-GHHU departed the rest break area.
The pilot then began a northbound line, following a previously completed survey line. During this time, the pilot again allowed the surveyor seated in the front left seat to follow the pilot on the controls.
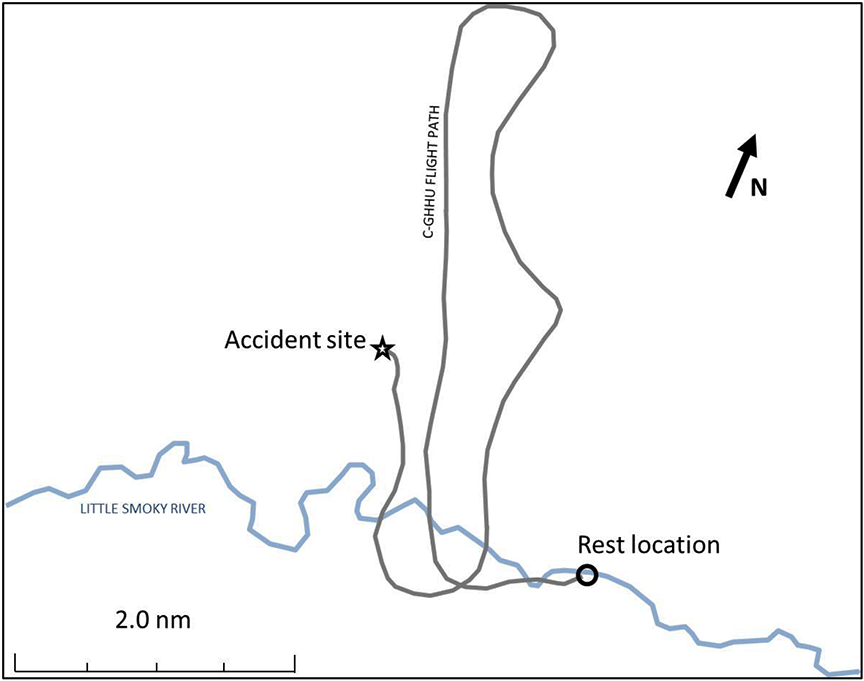
As the helicopter proceeded northbound, 1 of the surveyors identified the line as incorrect and indicated the need to reposition 1 line to the west. The pilot carried out a right turn and flew the helicopter approximately 4 nm south. The pilot then completed another right turn to roll out on the correct survey line (Figure 2). Moments later, at 1520, while flying at 58 mph in a descending left turn, approximately 160 feet above ground level (AGL), C-GHHU lost all engine power. This was immediately followed by a decay in NR and a descent. The engine‑out and rotor-low-rpm warning horns did not activate, and no warning lights illuminated on the annunciator panel.Footnote 6 Within 2 to 3 seconds, the aircraft descended and struck the trees. The heading at the time of impact was 246° magnetic. The helicopter came to rest suspended by the trees that it collided with, in a nose-high position, listing approximately 60° to the left and with its forward section approximately 7 feet above the ground; it did not strike the ground, but the aft portion settled to the ground.
The 406-megahertz (MHz) emergency locator transmitter (ELT) activated on impact, and was detected by the Cospas-Sarsat search‑and‑rescue satellite system. Within 10 minutes of ELT activation, the Joint Rescue Coordination Centre (JRCC) in Trenton, Ontario, had contacted Ridge Rotors. The company was able to locate C-GHHU using satellite flight‑following data.
The pilot was able to egress the wreckage by unfastening the seat belt and falling to the ground. The surveyor seated in the rear right seat was able to evacuate the helicopter through the right-rear cabin door, walk out of the accident site to a nearby service road, and place a 911 call by cellphone.
When the accident occurred, C-GKMS was refuelling at CED4. At approximately 1535, C‑GKMS was dispatched to locate the accident site, and arrived on location at 1557. The pilot of C-GKMS landed in a nearby clearing and, with the assistance of the surveyor who had been seated in the rear right seat, began administering first aid to the pilot of C-GHHU until the first responders arrived.
At 1700, the Royal Canadian Mounted Police arrived on scene with first responders. At approximately 1900, the Shock Trauma Air Rescue Society helicopter arrived on scene to evacuate the injured pilot to Grande Prairie, Alberta.
1.2 Injuries to persons
The pilot sustained serious blunt-force injuries to the chest and lower limbs.
The surveyor who had been seated in the rear right seat sustained minor head injuries, but was mobile and conscious during the entire event.
The surveyor who had been seated in the front left seat received fatal injuries during the impact sequence, as a result of trees penetrating the front left side of the helicopter.
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 0 | 1 | – | 1 |
| Serious | 1 | 0 | – | 1 |
| Minor | 0 | 1 | – | 1 |
| None | 0 | 0 | - | 0 |
| Total | 1 | 2 | – | 3 |
1.3 Damage to aircraft
The helicopter was significantly damaged as a result of impact forces.
1.4 Other damage
Not applicable.
1.5 Personnel information
Records indicate that the pilot was certified and qualified for the flight in accordance with existing regulations.
| Pilot licence | Commercial pilot licence (helicopter) |
|---|---|
| Medical expiry date | 01 October 2016 |
| Total flying hours | 1413 |
| Flight hours on type | 737 |
| Flight hours in the last 7 days | 53 |
| Flight hours in the last 30 days | 176* |
| Flight hours in the last 90 days | 230 |
| Flight hours on type in the last 90 days | 190 |
| Hours on duty prior to the occurrence | 8.83 |
| Hours off duty prior to the work period | 9.5 |
* The pilot’s flight time in the past 30 consecutive days was in accordance with Canadian Aviation Regulations Commercial Air Services Standard (CASS) 720.15. This standard allows the maximum flight time of 30 consecutive days (i.e., 150 hours) to be reset “if the flight crew member is provided with at least 5 consecutive days free from all duty” in the past 30 consecutive days [CASS paragraph 720.15(1)(g)], which was the case for the occurrence pilot.
1.6 Aircraft information
1.6.1 General
The Bell 206B helicopter was designed and manufactured by Bell Helicopter Textron Inc. It has a maximum take-off weight of 1451.5 kg (3200 pounds) and a maximum cruising speed of 150 mph. C-GHHU was equipped for day visual flight rules (VFR) and single-pilot operation. Dual flight controls were installed.
Records indicated that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. On 02 May 2013, it was registered as a commercial helicopter to Ridge Rotors. At the time of the occurrence, C-GHHU had accumulated approximately 17 061 hours of air time and 21 279 starts. The helicopter had no known deficiencies before the occurrence flight and was being operated within its weight‑and‑balance and centre-of-gravity limits. Nothing was found to indicate that the aircraft had encountered any type of system malfunction during the flight.
| Manufacturer | Bell Helicopter Textron Inc. |
|---|---|
| Type, model, and registration | BH06, 206B, C-GHHU |
| Year of manufacture | 1978 |
| Serial number | 2196 |
| Certificate of airworthiness / flight permit issue date | 11 August 1978 |
| Total airframe time (last logbook entry) | 17 061.2 hours |
| Engine type (number of engines) | Rolls-Royce 250-C20B (1) |
| Rotor type (number of rotor blades) | Semi-rigid (2) |
| Maximum allowable take-off weight | 1451.5 kg |
| Recommended fuel type(s) | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A |
1.6.2 Aircraft checklist
1.6.2.1 Rotorcraft flight manual engine pre-start checklist
In the Bell 206B helicopter, when the battery switch is turned ON as part of the engine pre‑start procedures, both the rotor-low and engine-out audio signals will activate. At N1 speeds greater than 55%, the engine-out audio signal will cease, and at greater than 90% NR, the rotor-low audio signal will cease.
The Bell 206B RFM engine pre-start checklist states that the warning-horn mute button (if installed) can be pressed to mute the engine-out warning horn. C-GHHU did not have the warning-horn mute button installed. Pulling the caution circuit breaker will silence the aircraft warning horns; however, there is no instruction in the Bell 206B RFM to do so.
The rotor-low-rpm system check procedure requires that the caution circuit breaker be engaged so that the rotor-low-rpm warning horn can activate when the collective lever is raised.
The risks associated with silencing aircraft warning and indication systems by circuit breaker usage have previously been identified, in TSB Aviation Investigation Report A94C0141.
1.6.2.2 Ridge Rotors Inc. checklist
It is common in the industry for companies to make changes in the aircraft checklist to reduce the distraction of the rotor-low-rpm warning horn activating during start-up and shutdown, for those helicopters that do not have the warning-horn mute system installed. Because C-GHHU was not equipped with a warning-horn mute system, Ridge Rotors had adopted a procedure to silence the rotor-low-rpm horn during start-up and shutdown. This procedure involved pulling the caution circuit breaker.
The Ridge Rotors engine shutdown checklist differs from the Bell 206B RFM normal operating procedures in that the rotor-low-rpm system check was moved from the engine‑start checklist to the engine‑shutdown checklist. Additionally, the engine‑shutdown checklist requires the caution circuit breaker to be pulled following the rotor-low-rpm and engine-out warning horn functionality test.
This change was made to identify deficiencies with the rotor-low-rpm system and allow maintenance personnel to rectify defects prior to the next flight. The company engine‑start checklist calls for the caution circuit breaker to be reset after the engine stabilizes at 60% to 62% N1 and requires that all circuit breakers be checked following the control and engine checks at 70% N1.
Ridge Rotors did not consult Bell Helicopter Textron Inc. for the checklist modifications, nor was it required by regulation to do so. Ridge Rotors did not conduct a risk assessment prior to implementing changes to the checklist.
1.6.2.3 Checklist modifications
Checklists are designed by aircraft manufacturers and approved by regulatory authorities as part of the original evaluation and approval of aircraft-type design data. Aircraft operators may decide to modify checklists to meet changing operational requirements, and it is important that these modified checklists retain all original restrictions and continue to follow the original design concepts contained in the approved flight manual or other documents associated with the certificate of airworthiness.
In TSB Aviation Investigation Report A98H0003, the Board expressed concern that, given the lack of checklist modification and approval standardization within the aviation industry, operators may unknowingly introduce latent unsafe conditions, particularly to emergency checklists.
1.6.3 Fuel system
The fuel system incorporates a single bladder-type fuel cell located below and aft of the rear passenger seats. Installed within the lower surface of the fuel cell are 2 electrically operated boost pumps, lower and upper tank indicating units, and an electrically operated sump drain valve.
The boost pumps are interconnected and supply fuel through a single hose assembly to the fuel shut-off valve. From the shut-off valve, the fuel is supplied to the airframe fuel filter and to the engine fuel system.
The fuel cell is filled from the right side. C-GHHU was fitted with a range-extender fuel system,Footnote 7 which increases the fuel capacity from 77.06 USG to 96.7 USG. The unusable fuel quantity is 1.06 USG.Footnote 8
1.6.3.1 Fuel boost pumps and potential for engine flame-out
Engine combustion stability is based on smooth burning and the ability of the combustion flame to remain alight over a wide operating range.Footnote 9 A flame-out is a condition in the operation of a gas turbine engine in which the fire in the engine goes out due to either too much or too little fuel sprayed into the combustors.Footnote 10
The Bell 206B RFM specifies that the “fuel boost pumps shall be ON at all times when [the] engine is being operated.”Footnote 11 The manual also states the following:
The engine will operate without boost pump pressure under 6000 feet pressure altitudeFootnote 12 and one boost pump will supply sufficient fuel for normal engine operations under all conditions of power and altitude.Footnote 13
The manufacturer does not authorize engine operation with both fuel boost pumps inoperative, due to a potential for unusual attitudes or out-of-trim conditions for fuel sloshing to occur,Footnote 14 which could result in an engine flame-out.
Flight with both boost pumps inoperative is not authorized. The manufacturer specifies that if 1 or both of the fuel boost pumps become inoperative during flight, the unusableFootnote 15 fuel is 10 USG.Footnote 16 With low fuel levels, it is possible for the fuel to slosh. Sloshing can result from uncoordinated flightFootnote 17 or during aircraft acceleration and deceleration. Uncoordinated flight can result from exposure to atmospheric turbulence or pilot flight control inputs. The sloshing can momentarily expose, or unport, 1 or both of the boost pumps to the air. The manufacturer confirmed that, given a sufficiently low fuel level, it is possible to unport even with 2 functional boost pumps while in uncoordinated flight or out-of-trim conditions.
During this investigation, the manufacturer also confirmed that “[t]he 206B fuel system does not have air-purging capabilities built in, and if [air ingestion] occurred, [it] could lead to an engine flame-out condition.”Footnote 18
After this report was first released, and in response to questions from the helicopter industry, the TSB laboratory conducted further analysis of potential unporting at various fuel levels. Table 4 summarizes the acceleration forces required at 3 fuel levels that resulted in fuel pump unporting. Additional calculations were made to determine what the ball in the turn and slip indicator would show at those levels of lateral acceleration.
| Quantity of fuel in tank (USG) | Lateral acceleration needed for complete fuel unporting | Representation on turn and slip indicator | |
|---|---|---|---|
| To left of helicopter (fuel displacement toward right side) | To right of helicopter (fuel displacement toward left side) | ||
| 10 | 0.18g | 0.12g | Ball halfway between centre and outer limit |
| 15 | 0.32g | 0.21g | Outer limit |
| 20 | 0.49g | 0.32g | Outer limit |
1.6.3.2 Fuel quantity indicating system
The fuel quantity gauge is mounted on the pilot’s instrument panel. The gauge is calibrated in USG from empty to 76 USG. The range-extender is equipped with a sight glass, which permits the pilot to visually observe the fuel level between 76 USG and full tank capacity.
Two float-type fuel-transmitting units are installed in the fuel cell (Appendix A). Both units are connected to a common quantity indicator. The lower unit is mounted in the bottom of the fuel cell and the upper unit is mounted in the upper section of the fuel cell. Together they transmit the total quantity of fuel.
Calibration of the fuel gauge is accomplished with the helicopter positioned 1° or 2° nose down and level in the lateral axis.Footnote 19 The investigation did not determine the slope of the gravel bar at Little Smoky River, where C-GHHU landed, and could not calculate how much indication error may have been introduced due to the attitude of the helicopter.
1.6.3.3 FUEL LOW caution light
An optional FUEL LOW caution light may be installed by operators of Bell 206B helicopters through the incorporation of Bell Helicopter Textron Inc. Technical Bulletin 206-84-94. The FUEL LOW indicating system equips the helicopter with a low-level float switch installed in the lower portion of the fuel cell that illuminates an amber FUEL LOW caution light on the caution panel, at approximately 20 USG of remaining fuel.
The Bell 206B RFMFootnote 20 specifies that when the FUEL LOW caution light is illuminated, the pilot should “[l]and as soon as practical,”Footnote 21 which the RFM defines as follows:
Landing site and duration of flight are at discretion of pilot. Extended flight beyond nearest approved landing area is not recommended.Footnote 22
C-GHHU did not have the FUEL LOW caution light installed.
1.6.4 Aircraft performance
The performance ratings at standard static sea level conditions for the Rolls-Royce model 250-C20B engine are applicable to the basic helicopter with all doors installed and without any optional equipment, which would appreciably affect lift, drag, or power available. The data do not include the effects on fuel consumption of bleed air heater and engine anti-ice operation. C-GHHU was not operating with bleed air heat or engine anti-ice on (Table 5).
| Maximum specific fuel consumption (pounds/shaft horsepower hour) |
Maximum fuel flow | ||
|---|---|---|---|
| (pounds/hour) | (USG/hour) | ||
| Takeoff (5 min.) | 0.650 | 273 | 39 |
| Normal cruise | 0.650 | 240 | 34 |
| Cruise A (90%)* | 0.665 | 221 | 31 |
| Cruise B (75%)** | 0.709 | 197 | 28 |
| Ground idle | – | 70 | 10 |
Source: Rolls-Royce Corporation, M250-C20 Series Operation and Maintenance Manual, Publication 10W2, Sixth Edition, Revision 21 (01 June 2016), section 72-00-00, Table 2, p. 40.
* Cruise A is the power level that is 90% of the rated normal cruise power at standard sea level static conditions.
** Cruise B is the power level that is 75% of the rated normal cruise power at standard sea level static conditions.
Rolls-Royce provided the specific fuel consumption numbers for flight conditions at a density altitude of 3900 feet above sea level for the power settings in Table 5. For the Cruise B (75%) power setting, this equated to a fuel burn rate of 27.2 USG per hour.
1.6.5 Canadian Aviation Regulations fuel requirements
The fuel requirements for helicopters operated in day VFR are published in CARs paragraph 602.88(3)(b), which stipulates that aircraft must carry sufficient fuel to allow them, “in the case of a helicopter, to fly to the destination aerodrome and then to fly for a period of 20 minutes at normal cruising speed.”Footnote 23
1.6.6 Flight planning and fuel consumption
The pilot left a flight itinerary with the company flight follower. The itinerary indicated that C-GHHU had 40 USG of fuel on board, and the endurance field indicated 1 hour and 32 minutes. These figures equate to a fuel burn of 26 USG per hour. A handwritten note, added by the flight follower at the bottom of this itinerary, indicated that the 40 USG figure was an error and that the helicopter had 90 USG on board (Table 6).
| Time | Airtime of flight leg (hh:mm) |
Total airtime (min.) |
Fuel burned during leg* (USG) |
Total fuel burned* (USG) |
Fuel remaining* (USG) |
Fuel burned during leg** (USG) |
Total fuel burned** (USG) |
Fuel remaining** (USG) |
|
|---|---|---|---|---|---|---|---|---|---|
| Takeoff | 1228 | 0 | 0 | 0 | 0 | 86 | 0 | 0 | 90 |
| River landing | 1448 | 02:20 | 140 | 64 | 64 | 22 | 61 | 61 | 29 |
| River takeoff | 1508 | 00:20 | 140 | 3 | 67 | 19 | 3 | 64 | 26 |
| Accident | 1520 | 00:12 | 152 | 5 | 72 | 14 | 5 | 69 | 21 |
Notes:
Times are based on global positioning system (GPS) data recovered from C-GHHU.
* Based on 86 USG on departure and fuel burn rate of 27.2 USG/hour, using data from the Rolls-Royce Cruise B (75%) performance rating.
** Based on 90 USG on departure and fuel burn rate of 26 USG/hour, using fuel amounts recorded in the company flight itinerary.
1.6.7 Height/velocity diagram
The height/velocity diagram (Appendix B) is a graph of safe and unsafe helicopter flight profiles; it shows the combinations of altitude and airspeed that may not allow sufficient time or altitude to enter a stabilized autorotative descent.Footnote 24 The diagram identifies altitude and airspeed combinations where operation should be avoided due to the low likelihood of being able to carry out a successful autorotative descent and landing.
The investigation determined that, based on the aircraft’s weight and density altitude during the occurrence flight, the aircraft was operating in and out of the “avoid” areas while conducting survey operations.
During a survey, when surveyors identify an area that requires closer inspection, the helicopter departs the survey line and circles the subject trees. It descends to 60 feet above the treetops and makes a slow pass (at less than 15 mph) over the affected trees so that the surveyor can mark the spot with a GPS-enabled computer. The slow pass is required for accurate GPS plotting because locations must be within 30 m of the subject trees.
During the occurrence flight, C-GHHU spent 1 hour and 48 minutesFootnote 25 in the survey area. Of this time, approximately 34 minutes, or 32% of the flight time, was spent within the “avoid” area of the height/velocity diagram.Footnote 26
On departure from CYZU, C-GHHU weighed 3101 pounds, and the density altitudeFootnote 27 was 2600 feet above sea level. At the time of the accident, C-GHHU weighed 2583 pounds, and the density altitude was 3900 feet above sea level. At the time of the occurrence, the helicopter was operating outside of the “avoid” areas on the height/velocity diagram (Appendix B).
The TSB has previously identified risks associated with operating helicopters within the “avoid” areas of the height/velocity profile.Footnote 28
1.6.8 Engine relight system
C-GHHU was equipped with an after-market engine relight systemFootnote 29 consisting of the electrical controller box (located in the engine compartment), a circuit breaker, and a switch (located in the instrument panel). An OFF–ARM switch controls the system. In the OFF position, the engine relight system is turned off. In the ARM position, the system will automatically engage the field/igniter relay if the power turbine rpm (N2) tachometer generator drops to 96% or below. Engagement of the field/igniter relay supplies a spark to the spark igniter assembly to attempt an engine relight. The system will automatically disengage when the gas producer rpm (N1) drops below 55%.
The Bell 206B RFM supplement for the engine relight system states that the system must be in the ARM position prior to operating the helicopter in falling or blowing snow conditions. There are no limitations for arming the system for all flight operations.
Ridge Rotors used the engine relight system for operations in falling or blowing snow only. The company did not consider having the system activated for low‑level survey operations. The engine relight system in C-GHHU was in the OFF position at the time of the engine flame‑out.
1.7 Meteorological information
The weather at 0700 was overcast and foggy, with visibilities as low as ⅛ statute mile (sm). The weather remained below VFR minimum requirements until 1200, when the visibility increased to 15 sm, with scattered clouds and light winds.
The 1500 hourly meteorological aerodrome report (METAR) for CYZU, 44 nm east of the accident site, indicated that the wind was 8 knots from 100° true (T) with variations from 50° to 150°. Visibility was 15 sm. There were few clouds at 2500 feet AGL with cumulonimbus clouds (CBs) in the area. The second layer of clouds was scattered at 10 000 feet AGL. The temperature was 14°C, the dew point was 7°C, and the barometric pressure was 29.85 inches of mercury, resulting in a density altitude of 3900 feet ASL. The remarks section of the METAR stated that the CBs were in the southwest quadrant.
As there were no CBs in the area of the accident and no associated turbulence, weather conditions were not considered a factor in the accident.
1.8 Aids to navigation
There was no indication of problems with the available aids to navigation.
1.9 Communications
The investigation received reports that, prior to the accident, the 3 occupants experienced some noise in their headsets, such as feedback or tone, that did not inhibit communication between the pilot and the surveyors. Although there was some tone or feedback on the intercom, the investigation determined that it did not contribute to the accident.
1.10 Aerodrome information
Not applicable.
1.11 Flight recorders
C-GHHU was not equipped with a flight data recorder or a cockpit voice recorder, and was not required to be by regulation.
The aircraft was equipped with a Blue Sky Network D1000C Iridium SATCOM GPS tracking unit. This unit was used to provide near-real-time GPS tracking of the helicopter.
The helicopter was equipped with 2 GPS units: a Garmin aera 796 GPS and a Garmin GPSMAP 296. The TSB laboratory successfully downloaded tracking and waypoint information from both units.
1.12 Wreckage and impact information
1.12.1 General
The wreckage was located in a dense coniferous forest. The average height of the trees was 80 feet, and the average diameter was 12 inches. The trees adjacent to the site showed very little damage related to the helicopter’s descent, although 2 trees had been topped.
All of the helicopter’s components were located and identified within a 50-foot radius of the aircraft (Figures 3 and 4). The helicopter’s forward section and cockpit were destroyed. The cabin sustained substantial impact damage, particularly on the left side of the fuselage. The fuel cell was punctured during the impact sequence and was leaking. The main-rotor head was intact, with its 2 rotor blades still attached. Both main-rotor blades sustained minor damage consistent with low NR, indicating that no power was being produced at the time of impact.
The tail-rotor was intact. One blade was straight with no damage to its skin. The other blade had sustained impact damage and was bent in 2 locations. The damage observed on both tail-rotor blades was consistent with low tail-rotor rpm, indicating that no power was being produced at the time of impact.
Continuity among the engine, transmission, and tail-rotor assembly was verified. The investigation determined that there had been flight-control continuity before the accident.
There were no visible ground scars.


1.12.2 Fuel system and engine component testing
During the TSB’s post-accident examination of the helicopter, 10 USG of uncontaminated fuel consistent with type Jet A fuel were recovered from the damaged fuel cell.
Following the occurrence, the fuel boost pumps and fuel quantity indicating systems were tested by the TSB. Both of these systems were found to be fully operational, with no abnormalities noted.
The starter-generator and the voltage regulator were tested by the TSB. Both of these systems were found to be operational, with no abnormalities noted that would have rendered the electrical system incapable of operating.
A post-accident examination of the engine found no mechanical issues that would have resulted in the deceleration. Fuel was found throughout the engine fuel system. All components tested met the required specifications, with no abnormalities noted.
The caution system warning-light panel was sent to the TSB laboratory for light bulb filament analysis. It was concluded that the rotor-low-rpm warning lights and the fuel pump warning lights were probably not illuminated at the time of impact. It could not be conclusively determined whether the engine-out warning lights were illuminated.
The caution circuit breaker was substantially damaged during the impact sequence. The position and functionality of the circuit breaker could not be determined.
1.13 Medical and pathological information
The investigation determined that there were no indications that the pilot’s performance was degraded by physiological factors. A flight duty analysis was completed for the pilot and fatigue was determined not to be a factor in this occurrence.
1.14 Fire
There was no post-impact fire.
1.15 Survival aspects
1.15.1 Helmets
In this occurrence, only the pilot was wearing an aviation helmet, which had deep scratches consistent with the helmet striking the helicopter structure and trees. The surveyors were not equipped with helmets, nor were they required to be by regulation.
1.15.2 Seat belts and crew harnesses
The pilot and surveyors were secured by the available 4-point harnesses. None of the occupants’ restraint harnesses failed. However, the front-left surveyor’s inboard lap-belt attachment fitting and anchor point pulled free from the mounting structure during the impact and breakup sequence.
1.15.3 Emergency locator transmitter
C-GHHU’s 406-MHz ELT activated upon impact. The ELT was secured to C-GHHU by a hook‑and‑loop fastener. It stayed intact and secured to the mounting tray during the impact sequence, remained serviceable, and was effective in transmitting the distress signal to the JRCC.
However, there have been a number of occurrences in which ELTs have not remained intact and secured to the mounting tray. TSB Recommendation A16-07 was issued as a result.Footnote 30
1.15.4 Satellite global positioning system tracking unit
The SATCOM GPS tracking unit used for flight following was effective in providing Ridge Rotors with the coordinates of the accident site. The company was able to quickly dispatch C-GKMS to the location of the occurrence involving C-GHHU.
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP215/2016 – Annunciator Panel Analysis
- LP310/2016 – Fuel Quantity Indicator Analysis
- LP272/2017 – Fuel Tank Unporting Analysis
1.17 Organizational and management information
1.17.1 General
Ridge Rotors is a Transport Canada–approved commercial air operator that has been in operation since 2004, conducting flight operations under CARs subparts 702 (Aerial Work) and 703 (Air Taxi Operations). It is based out of Blue Ridge, Alberta, the location of its company headquarters. Its operational base is at Tumbler Ridge, British Columbia, with a satellite base at Charlie Lake, British Columbia.
At the time of the occurrence, Ridge Rotors operated 1 Aerospatiale AS 350 B-2, 3 Robinson R44 helicopters, and 4 Bell 206B helicopters, including the occurrence aircraft. A 5th Bell 206B helicopter was registered, but not yet operational. Contracted TC-approved maintenance organizations perform maintenance on the helicopters.
1.17.1.1 Aerial work
The MPBS was being conducted by Ridge Rotors under CARs Subpart 702 (Aerial Work). The nature of aerial work, and the operating capabilities of helicopters, involve a variety of low-level operations.
Under CARs Subpart 702, there are no minimum operational altitude requirements for aircraft operating outside of built-up areas or carrying an external load. As a result, aircraft engaged in Subpart 702 operations are permitted, by regulation, to fly as low as they deem operationally necessary.Footnote 31
The low-flying operations conducted by Ridge Rotors were in compliance with the CARs and with the company operations manual. The surveyors were required to be on board; they performed an essential function in MPBS operations.
1.17.1.2 Ridge Rotors Inc. fuel planning and record keeping
A review of company documentation showed that it was common practice to conduct survey flights of more than 3 hours between refuelling stops. It was not uncommon for survey flights to land with 10 USG of remaining fuel. The journey logbook for C-GHHU showed 10 occasions in the 3 weeks prior to the accident when the helicopter was operated with multiple flight legs lasting over 3 hours.
The investigation determined that company pilots were using several different fuel‑burn rate estimates for flight operations, ranging from 23 to 30 gallons per hour (GPH). As previously stated, the flight-planning form filled out for the accident flight reflected a fuel‑burn rate of 26 GPH.
The Ridge Rotors operations manual describes general company refuelling procedures. The procedures direct the pilot to confirm that fuel gauges and tank levels are checked against the fuel pump meter to ensure that the right quantity of fuel has been loaded. The manual does not contain any procedures to record the fuel load for each helicopter.
The investigation could not determine the actual fuel load on board C-GHHU prior to departure, or its burn rate, because multiple helicopter fuel loads were recorded as single entries in the fuel logs, located at the Ridge Rotors fuel cache sites. Ridge Rotors’ practice was to record a series of flights in 1 aircraft journey log entry. Fuel-loading data was not recorded in the aircraft journey logbooks. This practice was compliant with CARs section 605.94.
1.17.1.3 Safety management at Ridge Rotors Inc.
When implemented properly, a safety management system (SMS) provides a framework for companies to manage risk effectively and make operations safer. Because Ridge Rotors is a CARs subparts 702 and 703 operator, the company was not required to have a TC‑approved SMS. The company does, however, have a system to manage safety, as well as a health and safety policy.
The Ridge Rotors safety management manual describes 2 hazard and risk identification processes. The first is the informal hazard and risk finding process. This process is not established as a specific procedure but is informal and ongoing, and consists of reviewing activities, procedures, and safety-relevant behaviour. The second is the formal hazard and risk identification process, which is documented on risk management worksheets and is conducted when changes are made to company structure, procedures, or key personnel, and/or when negative trends in safety performance are discovered.Footnote 32
The hazards of low‑altitude flight manoeuvres in aerial surveying and engine failure in flight were addressed by this formal hazard and risk identification process. The hazards were discussed in terms of their causes, control and recovery strategies, implementation and effectiveness.
The health and safety policy states in part that flight safety must be maintained by
[r]eporting of incidents and analysis of these to prevent [their] recurrence. All employees are encouraged to think pro-actively about safety and bring forward any ideas or recommendations for the improvement of safety.Footnote 33
The investigation was not able to determine if any safety concerns regarding low‑level flying had been reported within the company prior to the accident.
The last TC program validation inspection (PVI) of the company had been carried out on 25 January 2011. TC identified 2 minor administrative findings. When the PVI was conducted, Ridge Rotors’ helicopter fleet consisted of 5 aircraft of 3 types. In the period between the PVI and this accident, the size of the fleet increased to 8 helicopters.
TC planned to conduct a PVI on Ridge Rotors during the 2016–2017 fiscal year. However, at the time of the occurrence, the PVI had not been conducted.
1.17.2 TSB Watchlist
Safety management and oversight will remain on the TSB Watchlist until
|
The Watchlist identifies the key safety issues that need to be addressed to make Canada’s transportation system even safer.
Safety management and oversight is a Watchlist 2016 issue. As this occurrence demonstrates, some transportation companies are not managing their safety risks effectively, and many are not required to have formal safety management processes in place. TC oversight and intervention have not always been effective at changing companies’ unsafe operating practices.
All transportation companies are responsible for managing safety risks in their operations. Some companies consider safety to be adequate as long as they comply with regulatory requirements, but regulations alone cannot foresee all risks unique to a particular operation. That is why the TSB has repeatedly emphasized the advantages of having an SMS, an internationally recognized framework to allow companies to manage risk effectively and make operations safer.
Numerous recent TSB investigationsFootnote 34 into aviation occurrences have found that the operators involved did not manage safety risks effectively, either because they were not required to have an SMS or because the SMS had not been effectively implemented. The TSB has also issued several recommendations about SMSs and oversight.Footnote 35
1.17.3 TSB Recommendation A16-12
Ridge Rotors is a CARs subparts 702 and 703 operator and, as such, did not require a TC‑approved SMS; however, operators have an obligation to adequately manage safety risks. Compliance with regulations can only provide a baseline level of safety for all operators in a given sector. Since regulatory requirements cannot address all risks associated with a specific operation, companies need to be able to identify and address the hazards specific to their operation.
TSB accident investigations have emphasized the need for operators to be able to manage safety effectively. More than 10 years after introducing the first SMS regulations for CARs Subpart 705 operators and the companies that perform maintenance on those types of aircraft, SMS implementation has stalled. While many companies have recognized the benefits of having an SMS and voluntarily begun implementing one within their organization, CARs subparts 702, 703, and 704 operators are still not required by regulation to have an SMS, which equates to approximately 90% of all Canadian aviation certificate holders. As a result, TC does not have assurance that these operators are able to manage safety effectively.
Therefore, the Board has recommended that
the Department of Transport require all commercial aviation operators in Canada to implement a formal safety management system.
TSB Recommendation A16-12
TC’s response to Recommendation A16-12 (September 2016) was as follows:
Transport Canada agrees in principle with the recommendation. […]
TC will address this recommendation in two ways. First, by continuing to promote voluntary adoption of a safety management system among the balance of commercial air operators. To support this, the department will publish updated guidance material aimed at smaller sized-operations this year. Secondly, over the next year and a half, the department will be reviewing the policy, regulations and program related to safety management systems in civil aviation. The expected outcome of the review is a determination on the scope, regulatory instrument, applicability and oversight model.
In response to Recommendation A16-12, TC published Issue No. 02 of Advisory Circular 107-002, Safety Management System Development Guide for Smaller Aviation Organizations, on 02 September 2016. This document is provided to help small-sized aviation enterprises implement an SMS. However, the Board was unable to assess TC’s response to Recommendation A16-12 (November 2016), as there was no clear indication as to what actions will be taken by TC once the review is complete. TC has not indicated whether it intends to initiate a rule-changing process to require all commercial aviation operators to implement a formal SMS.
1.18 Additional information
Not applicable.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
2.1 Introduction
The examination of the helicopter, as well as the data collected during the investigation, indicated that there were no mechanical issues that would have resulted in the engine flame‑out and subsequent crash. There was no indication that physiological factors, including fatigue, had played a role in the accident. Therefore, the analysis will focus on the operational and organizational factors that contributed to the accident.
2.2 Fuel quantity
The exact quantity of fuel on board C-GHHU at the time of the occurrence could not be determined, because the fuel cell was punctured during the impact sequence and there was a lack of detailed fuelling records maintained by Ridge Rotors Inc. (Ridge Rotors).
It is probable that C-GHHU departed Whitecourt Airport, Alberta (CYZU), with 86 U.S. gallons (USG) of fuel and, based on Rolls‑Royce engine performance ratings (see Table 5, in Section 1.6.4) and adjusted for flight at 3900 feet above sea level, burned 27.2 USG per hour. This would result in a fuel quantity of 14 to 21 USG at the time of the accident (see Table 6, in Section 1.6.6).
2.2.1 Ridge Rotors Inc. fuel policies and procedures
Ridge Rotors did not have a policy in place for helicopters to land with a specified minimum quantity of fuel to ensure appropriate safety margins to prevent the unporting of boost pumps. It was common practice at Ridge Rotors to land with 10 USG of fuel. This amount of fuel is compliant with the minimum required by the Canadian Aviation Regulations (CARs).
However, the rotorcraft flight manual (RFM) states that a pilot should land as soon as practical when the low fuel light illuminates (when there are 20 USG remaining), meaning that “[e]xtended flight beyond nearest approved landing area is not recommended.” Although C-GHHU was not fitted with this system, the caution applied. Ridge Rotors did not consider this caution, as C-GHHU was not equipped with the low fuel light. The RFM also states that the unusable fuel becomes 10 USG when 1 or both boost pumps are inoperative.Footnote 36
If the RFM is not consistent with respect to cautions related to fuel quantities, there is a risk that the helicopter will be operated at fuel levels that could be conducive to engine flame-out.
Ridge Rotors did not have a detailed method of recording the amount of fuel being loaded onto the helicopters. Often, more than 1 helicopter was being refuelled at the same time and only the total amount of fuel dispensed was being recorded as a single entry. Compounding this issue was the recording of several daily flight sectors in 1 entry in the aircraft journey log.
Due to the limitations of this practice, it was not possible to accurately determine the amount of fuel being consumed and the length of each flight. If operators do not maintain detailed refuelling and flight-time records, there is a risk that flights will be continued with low fuel states, increasing the risk of accidents.
2.3 Pilot decision making
When C-GHHU arrived at the rest break area, the fuel state was likely 21 to 29 USG (see Table 6, in Section 1.6.6). The helicopter spent 20 minutes on the ground, after which the fuel state at the time of departure was likely 18 to 26 USG. The pilot continued the survey rather than flying directly to the fuel cache at Fox Creek Airport (CED4). It is likely that Ridge Rotors’ practice of regularly operating with less than 20 USG of fuel influenced the pilot to continue the survey flight rather than proceed to the refuelling location.
2.4 Engine flame-out
The Bell 206B helicopter’s fuel system can be susceptible to unporting when operating with less than 20 USG and acceleration forces are present. The TSB laboratory conducted further analysis of potential unporting at various fuel levels. With 10, 15, and 20 USG of fuel in the tank, the minimum lateral acceleration required for the fuel displacement to cause fuel unporting would be 0.12g, 0.21g, and 0.32g, respectively. These forces can be due to turbulence or pilot flight control inputs. The greatest susceptibility occurs when 1 or both of the boost pumps are inoperative. The manufacturer states that, in these circumstances, 10 USG are unusable.
In this occurrence, it is likely that the acceleration forces in the turn that resulted in the interruption of fuel flow were brief, given that fuel was found throughout the engine fuel system in the post‑accident examination.
While the helicopter was making a left turn, it is likely that acceleration forces caused 1 or both of the boost pumps to unport. The introduction of air into the combustion chamber interrupted fuel flow, resulting in an engine flame-out.
The engine relight system installed in C-GHHU was designed to activate when N2 decreased below 96%. When the engine flamed out, N2 would have decreased and conditions allowing the engine relight system to activate the igniter would have been met. The engine relight system in C-GHHU was not armed at the time of the accident. The system control switch was in the OFF position, so the engine igniter was not able to activate.
The engine relight system was off at the time of the occurrence, preventing the system from automatically attempting an engine relight following the engine flame-out.
2.5 Checklists
2.5.1 Checklist modification
Ridge Rotors had modified the Bell 206B helicopter checklist without consulting Bell Helicopter Textron Inc. This consultation is not required by regulation. Unlike the optional warning-horn mute switch, the use of the caution circuit breaker required the pilot to complete an extra checklist item to reset the system prior to takeoff. Any checklist item has the potential to be missed, which may create a hazard. In this occurrence, it is likely that the circuit breaker was not reset prior to liftoff, even though the company checklist required that the circuit breakers be engaged. If operators modify checklists without consulting the manufacturer, there is a risk that hazards will inadvertently be introduced into flight operations.
Because the helicopter was not equipped with a warning-horn mute system, the company had adopted a procedure to silence the rotor-low-revolutions per minute horn during start‑up and shutdown. This procedure involved pulling the caution circuit breaker during shutdown.
2.5.2 Checklist usage
Prior to departure from CYZU, the pilot had 2 opportunities to confirm that all circuit breakers were in and closed. The first opportunity was during the engine-start procedure and the second opportunity was during the control and engine checks. As a result, rotor-low warning and engine failure caution lights were not available to the pilot. It could not be determined whether this influenced the pilot’s response to the engine failure.
2.6 Risk mitigation for low‑altitude operations
The mountain pine beetle survey technique requires the helicopter to be operated for significant periods of time at low altitudes and speeds. If helicopter operations are conducted outside of the safe area depicted on the height/velocity diagram, there is a risk that pilots will not be able to complete emergency landings successfully.
Ridge Rotors was not required to have a Transport Canada–approved safety management system. The company did, however, have a system to manage safety, as well as a health and safety policy. Its system to manage safety included a formal risk management process that was applied to the hazards identified by the company. There was no information provided to the investigation to show implementation dates and follow-up dates associated with the risk assessments. Ridge Rotors safety management did not use a thorough risk analysis process to address the hazards and risks associated with this type of survey flying. Consequently, some available defences were not used, including the following:
- modifying observation techniques to allow for a higher altitudes
- using the engine relight system
- raising awareness in flight operations about the increasing risk of engine flame-out at fuel quantities below 20 USG
If companies do not use thorough risk analysis processes, there is a risk that mitigation strategies for operational hazards will not be employed.
2.7 Dual flight controls
The flight was conducted with the 2nd set of flight controls (dual flight controls) installed in the front left seat position. The pilot allowed the surveyor in the front left seat to follow the pilot on the flight controls while the aircraft was en route to the survey area. When C-GHHU departed the rest break area, after the surveyors had switched seats, the other surveyor followed the pilot on the flight controls until the start of the survey.
2.8 Survivability
The occupants’ injuries indicate that the deceleration forces were largely survivable. The fatal injuries received by the surveyor in the front left seat resulted from trees penetrating the helicopter cockpit during the impact sequence.
It is likely that the pilot’s helmet prevented a serious or fatal head injury. The use of the 4‑point seatbelt harnesses also helped prevent injury.
The ability of the surveyor in the rear right seat to contact emergency responders on a cellphone contributed to a timely rescue. The company’s use of a satellite tracking service also helped the rescue efforts.
In addition, the emergency locator transmitter activated on impact, which alerted the appropriate joint rescue coordination centre and facilitated the locating of the accident site. Despite having a hook-and-loop fastener, the emergency locator transmitter remained secured in its mounting tray, allowing it to activate.
3.0 Findings
3.1 Findings as to causes and contributing factors
- Ridge Rotors Inc. did not have a policy in place for helicopters to land with a specified minimum quantity of fuel to ensure appropriate safety margins to prevent the unporting of boost pumps.
- It is likely that Ridge Rotors Inc.’s practice of regularly operating with less than 20 U.S. gallons of fuel influenced the pilot to continue the survey flight rather than proceed to the refuelling location.
- While the helicopter was making a left turn, it is likely that acceleration forces caused 1 or both of the boost pumps to unport. The introduction of air into the combustion chamber interrupted fuel flow, resulting in an engine flame-out.
- The engine relight system was off at the time of the occurrence, preventing the system from automatically attempting an engine relight following the engine flame‑out.
3.2 Findings as to risk
- If the rotorcraft flight manual is not consistent with respect to cautions related to fuel quantities, there is a risk that the helicopter will be operated at fuel levels that could be conducive to engine flame-out.
- If operators do not maintain detailed refuelling and flight-time records, there is a risk that flights will be continued with low fuel states, increasing the risk of accidents.
- If operators modify checklists without consulting the manufacturer, there is a risk that hazards will inadvertently be introduced into flight operations.
- If helicopter operations are conducted outside of the safe area depicted on the height/velocity diagram, pilots risk not being able to complete emergency landings successfully.
- If companies do not use thorough risk analysis processes, there is a risk that mitigation strategies for operational hazards will not be employed.
3.3 Other findings
- It is likely that the pilot’s helmet prevented a serious or fatal head injury.
4.0 Safety action
4.1 Safety action taken
4.1.1 Transport Canada process inspection of Ridge Rotors Inc.
Following the accident, Transport Canada (TC) conducted a reactive process inspection (PI) of Ridge Rotors Inc. (Ridge Rotors) in September and October 2016. TC identified 6 minor findings of non-compliance in the following areas:
- pilot training program
- weight and balance program
- maintenance control system
- quality assurance program and training
On 27 October 2016, corrective action plans (CAPs) were submitted to address the findings of non-compliance. All CAPs were approved by TC. An on-site inspection to verify that the CAPs are being followed is scheduled for fall 2017, and a program validation inspection is planned for March 2018.
4.1.2 Ridge Rotors Inc.
Ridge Rotors now requires the auto relight system to remain on during all phases of flight. This change has been incorporated into the company’s standard operating procedures, and pilots have been trained accordingly.
4.1.3 Transportation Safety Board of Canada
On 31 January 2018, the TSB issued a safety advisoryFootnote 37 to Bell Helicopter Textron Inc. The advisory stated in part that
without consistent guidance from the RFM [rotorcraft flight manual] regarding operations at and below 20 USG, pilots may continue flight below 20 USG without appreciating the increased risk of unporting as fuel levels decrease. As such, Bell Helicopter may wish to consider amending the rotorcraft flight manual to include a 20 USG caution regardless of whether the FUEL LOW caution light is installed.
This report concludes the Transportation Safety Board of Canada’s investigation into this occurrence. The Board authorized the release of this report on . It was first released on .
Correction
The Factual information section of the report has been amended as follows:
- The last paragraph of Section 1.6.3, Fuel system, has been amended to include the unusable fuel quantity of 1.06 U.S. gallons (USG).
- The fourth paragraph of Section 1.6.3.1, Fuel boost pumps and potential for engine flame-out, has been amended to clarify that flight with both boost pumps inoperative is not authorized. The manufacturer specifies that if 1 or both of the fuel boost pumps become inoperative during flight, the unusable fuel is 10 USG.
- The end of the fourth paragraph of Section 1.6.3.1, Fuel boost pumps and potential for engine flame-out, has been amended to state that the manufacturer confirmed that, given a sufficiently low fuel level, it is possible to unport even with 2 functional boost pumps while in uncoordinated flight or out-of-trim conditions.
- A new paragraph has been added to the end of Section 1.6.3.1, Fuel boost pumps and potential for engine flame-out, to state that the TSB laboratory conducted further analysis of potential unporting at various fuel levels. Table 4 was added to show these results.
- A new paragraph has been added to the end of Section 1.6.4, Aircraft performance, to clarify the specific fuel consumption numbers for flight conditions at a density altitude of 3900 feet above sea level (ASL).
- Table 5 (labelled Table 4 in the initially released report) indicated a Cruise B (75%) fuel burn rate of 28 USG per hour. The table has been corrected to show the specific fuel consumption numbers for flight conditions at a density altitude of 3900 feet ASL, which equated to a fuel burn rate of 27.2 USG per hour.
- Section 1.16.1, TSB laboratory reports, has been amended to include laboratory report LP272/2017 – Fuel Tank Unporting Analysis.
- The second paragraph of Section 1.17.1.3, Safety management at Ridge Rotors Inc., indicated in the initially released report that the Ridge Rotors safety management system manual described an informal hazard and risk identification process. The report has been amended to clarify that the company has 2 hazard and risk identification processes.
The Analysis section of the report has been amended as follows:
- The second paragraph of Section 2.2, Fuel quantity, indicated in the initially released report that, at the time of the accident, C-GHHU had a fuel quantity of 12 to 21 USG. The report has been corrected to reflect the changes made to Table 5 (labelled Table 4 in the initially released report), which show the specific fuel consumption numbers for flight conditions at a density altitude of 3900 feet ASL, which resulted in a fuel quantity of 14 to 21 USG at the time of the accident.
- The second paragraph of Section 2.2.1, Ridge Rotors Inc. fuel policies and procedures, indicated in the initially released report that although C-GHHU was not fitted with the low fuel warning light, the caution to land as soon as practical remained. The report has been corrected to show that the caution applied.
- The third paragraph of Section 2.2.1, Ridge Rotors Inc. fuel policies and procedures, indicated in the initially released report that it is important for operators to understand the limitations of the Bell 206B helicopter fuel system and risks associated with flights conducted with less than 20 USG of fuel remaining. The report has been corrected to reflect that if the rotorcraft flight manual (RFM) is not consistent with respect to cautions related to fuel quantities, there is a risk that the helicopter will be operated at fuel levels that could be conducive to engine flame-out.
- Section 2.4, Engine flame-out, has been amended to state that the TSB laboratory conducted further analysis of potential unporting at various fuel levels.
- The second paragraph of Section 2.6, Risk mitigation for low‑altitude operations, indicated in the initially released report that there was no information provided by Ridge Rotors to show implementation dates and follow-up dates associated with the risk assessments. The report has been corrected to reflect that there was no information provided to the investigation to show implementation dates and effectiveness verification dates associated with the risk assessments.
The Findings section of the report has been amended as follows:
- Finding as to risk No. 1 indicated in the initially released report that if operators do not observe the minimum fuel quantities recommended in the RFM, there is a risk that the helicopter will be operated at fuel levels conducive to engine flame-outs. The report has been amended to reflect that if the RFM is not consistent with respect to cautions related to fuel quantities, there is a risk that the helicopter will be operated at fuel levels that could be conducive to engine flame-out.
The Safety action section of the report has been amended as follows:
- Section 4.1.3, Transportation Safety Board of Canada, has been added to state that on 31 January 2018, the TSB issued a safety advisory to Bell Helicopter Textron Inc.
This correction was approved by the Board on ; the corrected version of the report was released on .
Appendices
Appendix A – Bell 206B helicopter fuel system

Source: Bell Helicopter Textron Inc., 206B Pilot Ground and Flight Procedures, Revision 3‑1‑2003, p. 5‑1, with TSB annotations
Appendix B – Height/velocity diagram

Bell Helicopter Textron Inc., Bell Model 206B Rotorcraft Flight Manual, BHT-206B-FM-1, Revision B‑51 (02 July 2009), p. 3-4, with TSB annotations