Loss of control and collision with terrain
Airbus Helicopters AS 350 FX2, C-FBLW
TRK Helicopters Ltd.
Smithers, British Columbia, 82 nm NW
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 16 March 2016, at 1618 Pacific Daylight Time, the TRK Helicopters Ltd. Airbus Helicopters AS 350 FX2 helicopter (registration C-FBLW, serial number 2955) departed from the base of a ski run approximately 82 nautical miles northwest of Smithers, British Columbia, on a day visual flight rules flight to the base camp (located approximately 7 nautical miles south-southeast of the ski run), with the pilot and 6 passengers on board. Approximately 1 minute after takeoff, while operating at low altitude, the pilot initiated a descent into a ravine. During the descent, the helicopter's airspeed increased rapidly. Moments later, the helicopter abruptly rolled to the right, pitched up, and collided with terrain on a steep snow-covered slope. There were no injuries, and all 7 occupants egressed the aircraft. The helicopter was substantially damaged. There was no post-impact fire and the emergency locator transmitter did not activate.
Le présent rapport est également disponible en français.
1.0 Factual information
1.1 History of the flight
On 16 March 2016, at 1618,Footnote 1 the TRK Helicopters Ltd. Airbus HelicoptersFootnote 2 AS 350 FX2Footnote 3 (registration C-FBLW, serial number 2955) departed from the base of a ski run approximately 82 nautical miles (nm) northwest of Smithers, British Columbia, on a day visual flight rules flight to the base camp (approximately 7 nm south-southeast of the ski run). On board the aircraft were the pilot and 6 passengers (1 ski guide and 5 skiers). The occurrence flight was to be the last flight of the day. The intended route was along the Skeena River back to base camp. This was the same route flown by the pilot earlier that day.
After takeoff, the pilot initially flew at about 150 feet above ground level, then descended lower, in close proximity to the treetops, as the helicopter approached a small ridgeline. As the helicopter crossed the ridgeline, the pilot lowered the aircraft's nose to a nose-down attitude of approximately 20° and descended into a ravine.
During this manoeuvre, approximately 10 seconds before impact, the helicopter's airspeed increased rapidly from 120 to 132 knots indicated airspeed (KIAS).Footnote 4 At the same time, vertical flight loads decreased to approximately 0g,Footnote 5 and the helicopter's vertical speed reached a descent rate greater than 5000 feet per minute.Footnote 6
As the helicopter approached the rising terrain on the other side of the ravine, approximately 3 seconds before impact, the pilot applied aft cyclic control stick and attempted to turn left, away from the terrain ahead. However, the pilot was unable to move the cyclic control stick to the left. The helicopter then pitched up and, as it did so, its main rotor became aerodynamically overloaded and over-sped, activating the helicopter's main rotor high-rpm (revolutions per minute) warning horn. It experienced an uncommanded roll to the right and entered an uncontrolled descending right turn, which continued through approximately 180° of heading change (Figure 1 and Figure 2).
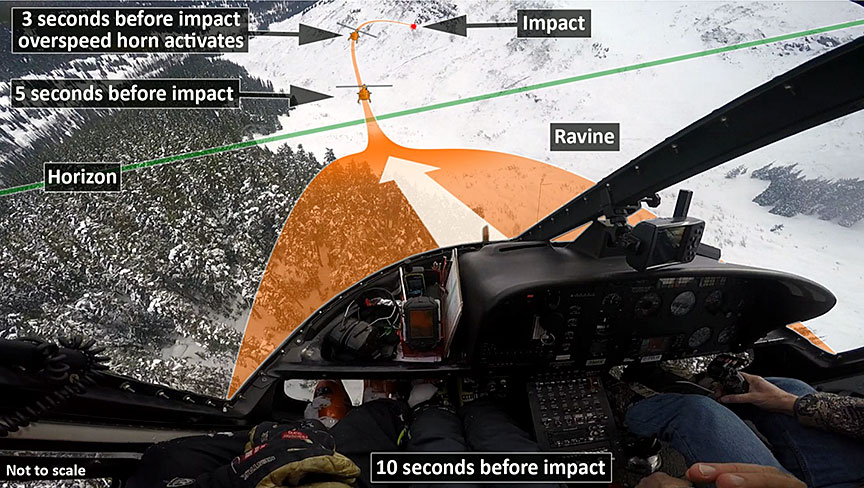

Just prior to impact, the pilot increased the helicopter's collective control in an attempt to reduce the helicopter's rate of descent. The helicopter struck the snow-covered slope of the ravine at an elevation of about 3100 feet above sea level, in a right-banked attitude, at approximately 25 KIAS.
The helicopter's main rotor blades cut a swathe through the snowpack on the aircraft's left side and continued to turn until the pilot shut down the engine and applied the rotor brake.
There were no injuries. Given the steep, downhill slope on the helicopter's right side, all 7 occupants egressed from the left side of the helicopter, after the main rotor stopped turning (Figure 3 and Figure 4).


1.2 Injuries to persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 0 | 0 | – | 0 |
| Serious | 0 | 0 | – | 0 |
| Minor/none | 1 | 6 | – | 7 |
| Total | 1 | 6 | – | 7 |
1.3 Damage to aircraft
The helicopter was substantially damaged.
1.4 Other damage
Not applicable.
1.5 Personnel information
1.5.1 General
| Pilot licence | Commercial pilot licence (CPL) – aeroplane and CPL – helicopter |
|---|---|
| Medical certificate issue date | 17 November 2015 |
| Total flying hours | 14 000 |
| Flight hours on type | 600 |
| Flight hours in the last 7 days | 12.1 |
Records indicate that the pilot was certified and qualified for the flight in accordance with existing regulations. The pilot held a commercial pilot licence for helicopters and airplanes, with a multi-engine land and sea rating. He had accumulated over 14 000 total flight hours in various airplanes and helicopter models. His previous flight experience also included the ownership of a flight school, and experience as a helicopter flight instructor.
Since joining TRK Helicopters Ltd., the pilot had flown about 600 flight hours in AS 350–series helicopters. The pilot had flown about 12 hours in the last 7 days after returning to work from a 21-day period during which he did not fly. There was no indication that fatigue played a role in this occurrence.
1.5.2 Training records
The investigation did not have access to detailed training records for the pilot. However, the pilot completed initial AS 350 training, including ground school in 2013. The training included ground instruction related to AS 350 hydraulic servo transparency.Footnote 7 The initial training course did not include flight exercises related to servo transparency.
In 2015, the manufacturer published an in-flight procedure to be used by approved training organizations for the "demonstration of servo transparency."Footnote 8 This document repeated content that was originally published in a 2012 Operational Evaluation Board report. However, there is no regulatory requirement for the student to carry out the exercise and experience servo transparency and the recovery procedure.
The pilot's most recent flight training had taken place on 20 May 2015. The training was completed on the Bell 206 helicopter.
1.6 Aircraft information
1.6.1 General
| Manufacturer | Airbus Helicopters |
|---|---|
| Type, model, and registration | AS 350 FX2, C-FBLW |
| Year of manufacture | 1996 |
| Serial number | 2955 |
| Certificate of airworthiness / flight permit issue date | 14 March 2014 |
| Total airframe time | 19 091.1 hours |
| Engine type (number of engines) | Honeywell LTS 101-700D-2 (1) |
| Rotor type | Semi-rigid, 3-bladed |
| Maximum allowable gross weight | 4961 pounds (2250 kg) |
| Recommended fuel type(s) | Jet A |
| Fuel type used | Jet A |
Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. The helicopter had no known deficiencies before the flight and was being operated within its load and centre-of-gravity limits. At the time of the occurrence, the helicopter was approximately 139 pounds below the maximum gross weight of 4961 pounds, and the centre of gravity was at the forward limit.
1.6.2 AS 350 hydraulic system
1.6.2.1 General
To reduce pilot workload, Airbus Helicopters uses hydraulically boosted flight controls on the AS 350 helicopter type. Under normal operating conditions (i.e., within the approved flight envelope), the AS 350's single hydraulic system, as installed on the occurrence helicopter, is designed to "give a very light control load on the cyclic stick, collective lever, and tail rotor pedals."Footnote 9 This is accomplished through the use of "irreversible hydraulic systems, which isolate the pilot from the aerodynamic forces of the main rotor by the use of servos."Footnote 10 However, the maximum available hydraulic power is limited by design, to protect the airframe against overstress if the approved flight envelope is exceeded. In the event of a hydraulic failure, the pilot is alerted by a red warning light and an aural alarm (horn).Footnote 11
Airbus Helicopters offers a duplicated hydraulic system, consisting of 2 independent hydraulic pumps attached in parallel that deliver pressure to the servos. The servos in this system are equipped with integrated load sensors that activate the LIMIT warning light when a pre-determined limit is exceeded, to ensure that the main rotor is not overloaded.
The dual hydraulic system is an option available on the AS 350 B3. Since 2009, this option has been installed on all AS 350 B3 helicopters delivered in North America. It is not a feature of the single hydraulic systems installed on the AS 350 B2s or the modified AS 350 involved in this occurrence. A duplicated hydraulic system cannot easily be installed retroactively on the single hydraulic system versions of the AS 350.Footnote 12
1.6.2.2 Servo transparency
According to Airbus Helicopters, the phenomenon of servo transparency can occur "during excessive maneuvering of any single hydraulic system equipped helicopter, if operated beyond its approved flight envelope."Footnote 13 The manufacturer does not consider servo transparency a failure of the system, but a limitation of all single hydraulic systems. Unlike in the case of a hydraulic system failure, there is no visual or aural indication to alert the pilot that the hydraulic system is approaching servo transparency.
A number of accidents involving servo transparency on AS 350–series helicopters have occurred (Appendix A). Due to concerns that operators and pilots did not fully understand servo transparency, on 04 December 2003, Eurocopter published 2 service letters as reminders to operators and pilots of the phenomenon of servo transparency. One service letter (No. 1648-29-03) concerned AS 350–series helicopters (Appendix B) and the other (No. 1649-29-03) concerned Colibri (EC120B) series helicopters. In 2006, the information contained in service letter No. 1648-29-03 was incorporated into the AS 350 BA Flight Manual (Appendix C). It is unknown whether the contents of the service letter, or the applicable section of the flight manual, were covered during the pilot's initial training on the AS 350.
Both the flight manual and the service letter concerning AS 350–series helicopters describe servo transparency as something that "occurs smoothly and is not dangerous, if properly anticipated by a pilot during an abrupt or excessive high load maneuver such as a high positive g-turn or pull-up."Footnote 14 Exceeding the approved flight envelope with excessive manoeuvring increases the risk of servo transparency, as do the following factors:
- high airspeed;
- high collective pitch input (i.e., high power or high torque);
- high gross weight;
- high g-loads; and
- high-density altitude (increasing altitude, temperature, or humidity).Footnote 15 Footnote 16
As described in the service letter, servo transparency occurs when the aerodynamic forces on the main rotor system, due to a combination of the factors listed above, exceed the opposing servo forces. This causes the excess aerodynamic forces to be transmitted back through the cyclic and collective controls. The service letter explains that, on AS 350‑type helicopters (clockwise main-rotor rotation, as viewed from above), the right servo receives the highest load when manoeuvring (retreating blade). Therefore, servo transparency causes the cyclic to move aft and to the right, and the collective pitch to decrease. This results in the helicopter pitching up and rolling to the right.
The corrective action required to counter these control inputs (i.e., applying left cyclic) may, if a pilot is not familiar with servo transparency, give the impression that the flight controls are jammed, when in fact the pilot can overcome the roll forces. If the severity of the manoeuvre is not reduced, the aircraft will continue to pitch up and roll right. The severity of the excess control feedback is proportional to the severity of the manoeuvre. Although servo transparency is often abrupt and surprising to the pilot, "the phenomenon normally lasts less than 2 seconds since the resultant aircraft reaction helps to reduce the factors that contribute to the severity of the maneuver and of the servo transparency."Footnote 17 In particular, the rapid loss of airspeed due to the pitch-up, combined with the down collective input, quickly reduces the aerodynamic forces that lead to servo transparency.
The flight manual limitations section states, "Continued operation in servo-transparency (where force feedback are [sic] felt in the controls) is prohibited."Footnote 18 According to the AS 350 flight manual and the service letters, the pilot's first reaction to control forces feedback (i.e., potential servo transparency conditions) should be to immediately reduce the severity of the manoeuvre.Footnote 19 The pilot should follow the control movement and allow the collective pitch to decrease (monitor main-rotor rpm at very low pitch) to reduce the overall load on the rotor system, and smoothly counteract the right cyclic tendency to prevent an abrupt left cyclic movement as hydraulic assistance is restored.Footnote 20 The flight manual also instructs pilots to, in a "maximum power configuration, decrease collective pitch slightly before initiating a turn, as in this manoeuvre power requirement is increased."Footnote 21
Service letter No. 1648-29-03 concludes by stating,
Footnote 22In 1985, the manufacturer completed a series of test flights to explore the points where servo transparency occurs. A series of graphic plots based on these data were developed to predict the g-load values for the onset of servo transparency based on given weights, density altitudes, and speeds.Footnote 23 These points were documented in certification flight test report H/EV 17.530.
In addition, the manufacturer has previously indicated that servo transparency cannot occur with a torque lower than 50%, it is very unlikely to occur below a speed of 100 knots, and it can occur at g-loads as low as 1.5g, depending on aircraft weight and speed, as well as on atmospheric conditions.Footnote 24 This information is not included in the flight manual, nor does the flight manual provide specific parameters on the interaction of the factors in the list above and how they can contribute to the onset of servo transparency.
In an effort to identify any systemic issues related to the guidance available to operators and pilots, the TSB investigation examined the guidance as it relates to servo transparency scenarios that may be encountered. This included consideration of a straight-ahead pull-up, as seen in this occurrence, or a pull-up with left or right roll. It has previously been established that servo transparency, when encountered in a left-hand turn, is mainly self-correcting, as described in the flight manual. Given that the tendency of the helicopter is to roll right when servo transparency is encountered, there is a greater risk that the helicopter will reach higher degrees of right bank when servo transparency is encountered in a straight-ahead or right-roll scenario. In particular, servo transparency is far riskier if it occurs in a right-hand turn at low altitude, because it results in further right roll at the same time as the collective pitch lever decreases.
According to the Accident Investigation Board Norway (AIBN), the information currently found in the flight manual is
Footnote 25As a result of these concerns, the AIBN issued the following recommendation:
Footnote 26A similar recommendation was issued by the United Kingdom's Air Accidents Investigation Branch (AAIB) in April 2009 following the investigation of an accident involving an AS 350 manoeuvring at high speed and low height:
Footnote 27In its response to the AAIB, Airbus Helicopters (then known as Eurocopter) did not agree with this recommendation. The rationale provided was that "the Flight Manual is sufficiently explicit in its presentation of the servo transparency phenomenon […]."Footnote 28 The manufacturer also indicated that it did not agree with the warning proposal in Safety Recommendation 2008-067.Footnote 29
The manufacturer therefore did not take action to address the safety recommendations of the AIBN and the AAIB.
In addition to the 2003 service letters published by Eurocopter, the Federal Aviation Administration (FAA) issued Special Airworthiness Bulletin (SAIB) SW‑04‑35 on 19 December 2003. SAIB SW-04-35 included references to Eurocopter service letters No. 1648-29-03 and No. 1649-29-03, and stated that some operators and pilots may not understand servo transparency. The SAIB repeated most of the information in Eurocopter service letter No. 1648-29-03.
On 14 May 2007, the Australian Civil Aviation Safety Authority issued Airworthiness Bulletin 27-008, Issue 1, "Eurocopter Flight Control Servo Transparency," which repeated the information in the FAA's SAIB SW-04-35.
The investigation determined that the occurrence pilot was not aware that servo transparency could be encountered below the never-exceed speed (VNE). The pilot had previously encountered momentary stiffening of the controls, but assumed that the helicopter had to remain controllable at speeds up to VNE in order to meet certification requirements. The occurrence pilot did not fully understand the contribution of other factors to servo transparency, even at speeds below VNE.
1.7 Meteorological information
Weather at the time of the occurrence consisted of broken cloud cover, no precipitation, a temperature of about −5 °C, and light winds. The investigation determined that the density altitude was approximately 1000 feet at the time of the occurrence.
1.8 Aids to navigation
Not applicable.
1.9 Communications
Not applicable.
1.10 Aerodrome information
Not applicable.
1.11 Flight recorders
The helicopter was not equipped with a flight data recorder or a cockpit voice recorder, and these were not required by regulation.
The helicopter was equipped with a Garmin GPSMAP 296 global positioning system (GPS) that incorporated a data recording capability. The GPS data was downloaded at the TSB Engineering Laboratory. Using the GPS data, the investigation determined that a vertical acceleration of 1.5g to 1.8g was applied 3 seconds before impact, when the pilot attempted to avoid the terrain on the other side of the ravine.
The helicopter was equipped with a SkyTrac DSAT-300 satellite tracking unit, which provides for automatic position reporting.
1.11.1 On-board recordings and flight data monitoring
The occurrence flight was captured on 2 personal in-flight videos. The investigation was able to determine, using these 2 videos, that the indicated airspeed was significantly lower than the actual airspeed throughout most of the flight.Footnote 30
During the initial cruise portion of the flight, the indicated airspeed was constant at about 55 knots, which was up to 60 knots less than the airspeed estimated based on the GPS data. After a short period, while the helicopter was stable in cruise flight, the indicated airspeed abruptly increased to approximately 75 knots, which was up to 35 knots less than the estimated value derived from the GPS data. When the pilot initiated the descent into the ravine, the indicated airspeed first rapidly increased to about 100 knots, then to about 135 knots, becoming more consistent with the airspeed value estimated from the GPS data. The speed discrepancy was likely due to fouling of the pitot-static system because of snow.
A detailed summary of the flight instrument information for the last 20 seconds of the flight is outlined below.
| Seconds before impact | Torque (%) |
Rotor rpm |
Indicated airspeed (knots) |
GPS airspeed (knots) | Roll (degrees) |
Pitch (degrees) |
Altimeter (feet) |
Descent (ft/min) |
|---|---|---|---|---|---|---|---|---|
| 20 | 81 | 385 | 72 | 112 | NV* | NV | 3600 | 0 |
| 18 | 81 | 385 | 71 | 112 | 20R** | −4 | 3600 | 0 |
| 16 | 80 | 385 | 75 | 113 | 20R | −4 | 3600 | 0 |
| 14 | 80 | 390 | 75 | 113 | 20R | −5 | 3600 | 0 |
| 13 | 80 | 390 | 92 | 114 | 20R | −5 | 3600 | −300 |
| 12 | 80 | 390 | 98 | 115 | 20R | −5 | 3600 | −500 |
| 10 | 69 | 390 | 102 | 118 | 20R | −20 | 3600 | −700 |
| 9 | 64 | 390 | 115 | 119 | 10R | −23 | 3500 | −1000 |
| 8 | 64 | 390 | 130 | 120 | 5R | −25 | 3400 | −1400 |
| 7 | 72 | 385 | 130 | 124 | 5R | −22 | 3300 | −2300 |
| 6 | 79 | 385 | 132 | 130 | 10R | −19 | 3250 | −3000 |
| 5 | 80 | 385 | 132 | 137 | 10R | −10 | 3100 | −3000 |
| 4 | 66 | 390 | 132 | 141 | 10R | −10 | 3000 | −3000 |
| 3 | 50 | 390 | 130 | 141 | 30R | NV | NV | NV |
| 2 | NV | NV | NV | NV | NV | NV | NV | NV |
| 1 | 12 | 370 | 98 | NV | 30R | NV | NV | −3000 |
* NV: not visible
** R: right
The investigation determined that the occurrence pilot had previously encountered airspeed indication anomalies similar to those noted above, following a snow landing, as was the case on the occurrence flight. The pilot's previous experience was that the airspeed indications would return to normal within a couple of minutes, possibly due to a temporary accumulation of snow in the static port located on the underside of the helicopter.
The 2 in-flight videos did not meet the definition of an on-board recording under the Canadian Transportation Accident Investigation and Safety Board Act, as it pertains to aviation:
Footnote 31However, the in-flight videos did provide vital information for the analysis of the occurrence flight.
In 2013, following its investigation into a loss-of-control / in-flight breakup occurrence in March 2011 northeast of Mayo, Yukon,Footnote 32 the TSB found that, if cockpit or data recordings are not available to an investigation, the identification and communication of safety deficiencies to advance transportation safety may be precluded.
In the preamble to its recommendation, the Board stated that
Canadian Aviation RegulationsThe Board acknowledged that issues would need to be resolved to facilitate the effective use of recordings from lightweight flight recording systems, including integration of this equipment in an aircraft, human-resource management, and legal issues, such as restrictions on the use of cockpit voice and video recordings.
Nevertheless, given the potential of this technology, combined with flight data monitoring (FDM), to significantly improve safety, the Board believed that no effort should be spared to overcome these obstacles. Therefore, the Board recommended that
the Department of Transport work with industry to remove obstacles to and develop recommended practices for the implementation of flight data monitoring and the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems.
Transportation Safety Recommendation A13-01
TC has undertaken the following actions to address the safety deficiency identified in Recommendation A13-01, regarding the installation of lightweight flight recording systems by commercial operators not currently required to carry these systems:
- In 2013, after conducting a risk assessment to evaluate alternate approaches to FDM, TC informed the TSB that it supported Recommendation A13-01. In 2015, TC informed the TSB that it intended to revisit this risk assessment.
- In 2013, TC informed the TSB that it would develop an advisory circular outlining recommended practices for FDM programs.
- In 2013, TC informed the TSB that it would incorporate its analysis and review of Recommendation A13-01 into its planned assessment for cockpit voice and flight data recorders, which was scheduled to begin in 2014–2015.
- In 2014, TC informed the TSB that it would consider adding FDM principles in future regulatory initiatives and amendments.
- In 2015, TC informed the TSB that it would prepare an issue paper on the use of FDM, providing factual information on FDM, including its benefits, costs and challenges.
However, due to other commitments, TC did not initiate its work for any of these undertakings.
In February 2018, TC conducted a focus group with the industry to assess the challenges and benefits associated with the installation of lightweight flight recording systems on aircraft, which are not currently required to carry these systems.
However, until the focus group reaches conclusions as to the challenges and benefits associated with the installation of lightweight flight recorders in aircraft not currently required to carry them, and TC provides the TSB with its plan of action moving forward following those conclusions, it is unclear when or how the safety deficiency identified in Recommendation A13-01 will be addressed. The Board is concerned that few concrete actions have been taken to address Recommendation A13-01 and that this will result in protracted delays as observed on numerous other recommendations.
Therefore, the Board is unable to assess the response to the recommendation.
The benefits of lightweight recorders were also identified by the AIBN, which called lightweight flight recorders "a major step forward that could, to a great extent, meet the need of safety investigation authorities."Footnote 33 Following an investigation into an AS 350 B3 accident, the AIBN issued Recommendation SL 2012/10T:
Footnote 34On 03 April 2017, in response to 12 safety recommendations issued by 7 safety investigation authorities, EASA published Notice of Proposed Amendment 2017-03: In-flight recording for light aircraft. The notice proposes that lightweight flight recorders be made mandatory for some categories of commercially operated light aeroplanes and light helicopters. It also proposes promoting voluntary installation of such equipment for all other light aeroplanes and light helicopters, and for all balloons.
As of October 2017, the Notice of Proposed Amendment was in the consultation phase, with a decision scheduled for the last quarter of 2018.Footnote 35
1.12 Wreckage and impact information
The investigation found no pre-existing defects, and all damage, deformations, and fractures were determined to be the result of the collision with the hillside. The impact forces were attenuated by the deep snowpack, the spreading and deformation of the landing gear skids, and the deformation of the seats. The tail boom showed buckling and creasing at its point of attachment to the rear airframe. The underside of the helicopter was crushed and deformed from the impact with the snow. The main rotor and drivetrain system had made contact with the hillside; the 3 blades were slightly scored and bent, and 2 of them were split at the trailing edge from compression forces. All drive components could be rotated by hand. The engine remained operating throughout the flight and on the ground after impact; an over-torque event coincident with the collision was recorded on the Aerodyne engine-monitoring system. The flight control hydraulic system components were removed for further analysis.
All hydraulic system components were examined for continuity and integrity at the component manufacturers' facilities in England and France, and found to be within service limits.
1.12.1 Emergency locator transmitter
The occurrence helicopter was equipped with an Artex Aircraft Supplies Inc. (Artex) 406-MHz emergency locator transmitter (ELT) (part number 453-6604, serial number 188-08306).Footnote 36 The ELT did not activate at the time of impact. The ELT was sent to the TSB Engineering Laboratory for further analysis. The investigation determined that the ELT transmitted properly when the selector switch was set to ON, but did not activate under specified g-load, as intended, when the selector switch was set to ARM.
Unless the Minister of Transport authorizes otherwise, regulationsFootnote 37 require aircraft to be maintained in accordance with a maintenance schedule that conforms to the Aircraft Equipment and Maintenance Standards. These standards include the annual performance testing of ELTs and a test of the automatic activation system.Footnote 38
In this occurrence, the Minister had not authorized the operator to deviate from the maintenance schedule. Annual performance testing was carried out on the occurrence aircraft's ELT on 10 December 2015; no deficiencies were noted.
Artex's periodic maintenance inspection procedures for the g-switch check include:
Activate the ELT by using a rapid forward (i.e., throwing) motion, in the direction of the arrow on the ELT label, followed by a rapid reversing action.
Verify activation by listening for the aural sweep tone on the receiver.
Reset the ELT by toggling the control switch to the "ON" position and then back to the "ARM" position.Footnote 39
The g-switch must activate for the ELT to be deemed serviceable.
Further analysis of the occurrence ELT revealed that the ELT's 2-position inertial switch (i.e., g-switch) (part number 2014-20-000), supplied by Select Controls Inc. in September 2008, was seized. The g-switch is an air-damped, linear type of switch. It is composed of a gold-plated brass ball and a silver spring inside of a tubular brass casing. On impact, the force exerted on the mass of the ball is designed to compress the spring and cause it to touch a contact point.
In the case of the occurrence ELT, it was determined that the ball's vibrations wore away the gold plating, with the resulting debris causing a black powder-like residue to accumulate. This, in turn, made the ball stick and rendered the ELT unserviceable. However, it was also determined that, even if the ELT had been serviceable, it may not have activated: the helicopter collided with deep snow, which would likely have attenuated impact forces to a level below what was required to activate the ELT.
In addition to the g-switch, the occurrence ELT model has a 5-axis g-switch module installed. This module requires a minimum force of 12g along any of the 5 axes to activate the ELT.Footnote 40 However, impact forces in the deep snow would likely have been attenuated to a level below what was required to activate this secondary g-switch module.
During the course of the investigation, the supplier of the g-switch confirmed that the switch may stick momentarily due to vibrations that cause the gold plating on the inside of the casing and ball to deteriorate and form a powder-like residue, as the ELT ages, especially in high-vibration environments. As a result, for ELTs that have been in service for 5 to 7 years, the g-switch supplier recommends that the g-switch be tested every 4 months, or replaced. For ELTs that have been in service for 7 to 9 years, the g-switch should be tested every 3 months, or replaced. For ELTs that have been in service for 10 or more years, the g-switch should be replaced.
Based on recommendations made by the g-switch supplier, 1 ELT manufacturer using the same style of g-switch issued a service bulletin to address the issue (Appendix D). The g-switch supplier then discussed those recommendations with another ELT manufacturer. That ELT manufacturer also published a service bulletin outlining those recommendations (Appendix E). Artex became aware of potential g-switch issues from the field in 2011, and introduced a modified design with an upgraded, hermetically sealed g-switch for the Artex ME 406 ELT that was approved by the FAA in 2013. In addition, all Artex component maintenance manuals were updated to call for the replacement of the legacy g-switch with the new g-switch upon any service event, including battery replacement, which is every 5 years. All subsequent Artex products use this new g-switch.
1.12.1.1 Previous occurrences involving stuck g-switches
Two previous TSB investigationsFootnote 41 found that stuck Select Controls Inc. g-switches (part number 2014-1-000) prevented the ELT from activating following an occurrence. In both instances, wear on the ball and casing resulted in the accumulation of a black powder-like residue that caused the ball to stick, rendering the ELT unserviceable.
1.13 Medical and pathological information
Not applicable.
1.14 Fire
There was no fire.
1.15 Survival aspects
The passengers had received a briefing given by both the pilot and the ski guide for operations in and around the helicopter. All passengers were wearing ski helmets as well as seat restraints with shoulder harnesses. The ski guide was wearing a seat restraint with a shoulder harness, but was not wearing any head protection. The pilot was wearing a helmet, a lap belt, and a shoulder harness.
Following the impact with terrain, some passengers initially attempted to egress before the main rotor had stopped turning; however, the ski guide intervened and the occupants then waited until the main rotor had stopped turning. All occupants then exited from the left-hand side of the helicopter.
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP065/2016 – ELT Analysis
- LP066/2016 – Video Analysis
- LP125/2016 – Performance Analysis
- LP126/2016 – Hydraulic System Examination
1.17 Organizational and management information
1.17.1 TRK Helicopters Ltd.
TRK Helicopters Ltd. operates under CARs Subpart 702, Aerial Work, and Subpart 703, Air Taxi Operations, using Robinson R44, Bell 205, Bell 407, and Airbus Helicopters EC 120 B, EC 130 B4, AS 350, and AS 355 helicopters from its main base at Langley Regional Airport (CYNJ), British Columbia.
TRK Helicopters Ltd. does not have a safety management system (SMS), nor is it required by regulation to have one.
1.17.2 Transport Canada oversight of TRK Helicopters Ltd.
In January 2016, TC conducted a program validation inspection (PVI)Footnote 42 of TRK Helicopters Ltd. The PVI activities were limited to reviewing previous findings of non-compliance with regulations, and the systems in place for tracking lapses, remediation, and follow-up actions or corrective action plans. The PVI did not consist of hazard assessments or reviews of pilot training records, maintenance activities, or training gaps.
1.18 Additional information
Not applicable.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
There was no indication that a system malfunction contributed to this accident. This analysis will focus on the design characteristics of the AS 350 hydraulic system, and how control inputs during the final seconds of the flight resulted in servo transparency. The analysis will also discuss some safety deficiencies related to certain emergency locator transmitter (ELT) g-switches, as well as highlight the role that personal video recordings played in this investigation.
2.1 Servo transparency
The hydraulic system on the AS 350 helicopter is designed to reduce the force required to fly the aircraft and to isolate the pilot from these forces. However, a design limitation of the system may result in servo transparency during excessive manoeuvring under certain combinations of high airspeed, high collective pitch input, high gross weight, high g-loads, and high-density altitude, even when the helicopter is being operated within the approved flight envelope. When this happens, the forces increase to the point where they exceed the capability of the hydraulic system, and those forces are transmitted back to the pilot in the form of uncommanded aft and right cyclic inputs.
In this occurrence, all of the risk factors except high-density altitude were present, causing the aerodynamic loads on the main rotor to exceed the capability of the hydraulic system. This resulted in servo transparency, which caused the helicopter to pitch up and roll to the right, in close proximity to the snow-covered slope. Although the self-correcting tendency of the aircraft (i.e., the pitching-up that resulted in decreased airspeed and therefore reduced aerodynamic loads) allowed the pilot to regain hydraulic system assistance, it was too late for the pilot to recover before the impact with the snow-covered terrain. The AS 350 hydraulic system experienced servo transparency due to the combination of a high-power descent near the never-exceed speed (VNE) and a 1.5g to 1.8g vertical acceleration near maximum gross weight.
There have been a number of accidents in the past involving servo transparency on AS 350–series helicopters. In 2003, the manufacturer issued a service letter to address concerns that operators and pilots did not fully understand the phenomenon of servo transparency. The service letter described it as something that was not dangerous if properly anticipated during abrupt or aggressive manoeuvres.
In this occurrence, the pilot did not fully understand the factors that increase the risk of servo transparency or that it could be encountered at airspeeds below VNE. As a result, the pilot placed the helicopter in a flight regime, at low height, that included 4 of the 5 factors that increase the risk of servo transparency. The pilot placed the helicopter in a flight regime that resulted in servo transparency at a height from which the pilot was unable to recover before the impact with the snow-covered terrain.
Aside from cautioning against exceeding the approved flight envelope and prohibiting continued operation in servo transparency, the AS 350 flight manual lacks details about this phenomenon. Although Airbus Helicopters has previously established the combinations of g-loading, power, weight, speed, and density altitude that are likely to result in servo transparency, none of that information is included in the AS 350 flight manual.
As well, other investigation agencies have recommended that Airbus Helicopters modify the flight manual to add a warning about the inherent risks associated with servo transparency in a right turn at low height, but the manufacturer has not acted on those recommendations. The most comprehensive source of servo-transparency information that the manufacturer has produced—and made available to operators and pilots—is a 2003 service letter with general information about the factors that increase the phenomenon's risk of occurring. However, the flight manual was updated in 2006 to reflect the key information from the 2003 service letter.
2.2 Emergency locator transmitter g-switches
The single-axis g-switch seized because of undetected wear over time. This rendered the ELT unserviceable. Although this did not play a role in the outcome of the accident, it highlights a potential risk within the transportation system.
The supplier of the g-switch recommended inspection and replacement procedures, which have been adopted by some ELT manufacturers. As demonstrated by this occurrence, some ELT manufacturers have not adopted the g-switch supplier's recommended inspection and replacement schedule, nor are they required by regulation to do so.
In this particular occurrence, the internal failure of the ELT went undetected prior to the accident. If ELT manufacturers do not follow recommended inspection and/or replacement schedules provided by sub-component suppliers, there is an increased risk that the ELT will fail.
2.3 On-board recordings and data monitoring
The personal video recordings played a critical role in identifying safety deficiencies in this occurrence. Although they do not meet the definition of an on-board recording under the Canadian Transportation Accident Investigation and Safety Board Act, their role in this investigation does underscore the value of recordings as a means of advancing transportation safety. In particular, they can be used reactively, to identify safety deficiencies that played a role in an aviation occurrence, or proactively, as part of a flight data monitoring program with the potential to prevent accidents from occurring.
Recognizing these important benefits, the TSB issued Recommendation A13-01, calling for Transport Canada to work with industry to implement flight data monitoring and lightweight flight recording systems in commercial aircraft. If this recommendation is adopted, and concrete action is taken, it has the potential to enhance transportation safety significantly on multiple levels.
To date, Transport Canada has not yet taken specific action to address the safety deficiency identified in Recommendation A13-01. As a result, the risks associated with the safety deficiency identified in Recommendation A13-01 will persist.
3.0 Findings
3.1 Findings as to causes and contributing factors
- The AS 350 hydraulic system experienced servo transparency due to the combination of a high-power descent near the never-exceed speed and a 1.5g to 1.8g vertical acceleration near maximum gross weight.
- The pilot placed the helicopter in a flight regime that resulted in servo transparency at a height from which the pilot was unable to recover before the impact with the snow-covered terrain.
3.2 Findings as to risk
- If emergency locator transmitter manufacturers do not follow recommended inspection and/or replacement schedules provided by sub-component suppliers, there is an increased risk that the emergency locator transmitter will fail.
4.0 Safety action
4.1 Safety action taken
4.1.1 TRK Helicopters Ltd.
The operator, TRK Helicopters Ltd., stated that its training curriculum has been amended to emphasize emergency procedures related to hydraulic system failures and the conditions that increase the risk of servo transparency.
4.1.2 Airbus Helicopters
Airbus Helicopters has begun developing flight data monitoring systems with an affiliate company, Appareo Systems, which provides lightweight on-board flight data recording units.
Airbus Helicopters also stated that it is revising the AS 350–series advanced training syllabus, as well as considering the inclusion of a video presentation of the servo transparency phenomenon and its appropriate response in flight.
This report concludes the Transportation Safety Board of Canada's investigation into this occurrence. The Board authorized the release of this report on . It was officially released on .
Appendices
Appendix A – Previous occurrences involving servo transparency on AS 350–series helicopters
| Agency | Date of occurrence | Occurrence number and summary |
|---|---|---|
| U.S. National Transportation Safety Board | 2001-10-19 | FTW02FA017 – The pilot initiated a descending right‑hand turn at about 200 feet above ground level, at an airspeed of 115 to 120 knots. During the turn, the pilot realized the turn was too steep and tried to shallow the turn; however, the cyclic would not move and the helicopter subsequently collided with the ground. There were 2 fatalities. |
| U.S. National Transportation Safety Board | 2004-12-14 | LAX05FA053 – While manoeuvring for landing, the pilot was unable to move the cyclic and the helicopter collided with the ground. The report refers to the phenomenon of servo transparency. There was 1 fatality. |
| Transportation Safety Board of Canada | 2007-07-23 | A07W0138 – The pilot encountered servo transparency during a sudden, high-speed descent. The pilot had received training to recognize servo transparency; however, the pilot was not able to apply this training during the actual event. The pilot was unable to recover prior to the impact with terrain. There was 1 fatality. |
| U.K. Air Accidents Investigation Branch | 2007-09-15 | EW/C2007/09/06 – It is probable that, at some stage, the pilot manoeuvred the helicopter at maximum performance, whether to ensure terrain avoidance and/or to arrest the descent, or for some other reason. This would have made a servo transparency encounter more likely. There were 4 fatalities. |
| Accident Investigation Board Norway | 2011-07-04 | SL2012/13 – Abrupt manoeuvring may have led to an encounter with servo transparency at a height from which the pilot was unable to recover before the impact. The report includes a detailed description of servo transparency. There were 5 fatalities. |
| Swiss Transportation Safety Investigation Board | 2013-07-01 | No. 2265 – The report states that the accident is attributable, with a high likelihood, to a loss of control by the pilot after the onset of servo transparency during a right turn in close proximity to terrain, and the subsequent collision of the helicopter with the ground. There was 1 fatality. |
Appendix B – Eurocopter service letter No. 1648-29-03


Source: Eurocopter, Lettre-Service No. 1648-29-03 (04 December 2003), Hydraulic Power System: Servo Transparency.
Appendix C – Flight manual information on servo transparency

Appendix D – ACK Technologies Inc. Service Bulletin SB E-01.8

Appendix E – Narco Avionics Inc. Service Bulletin No. ELT 910 No. 2
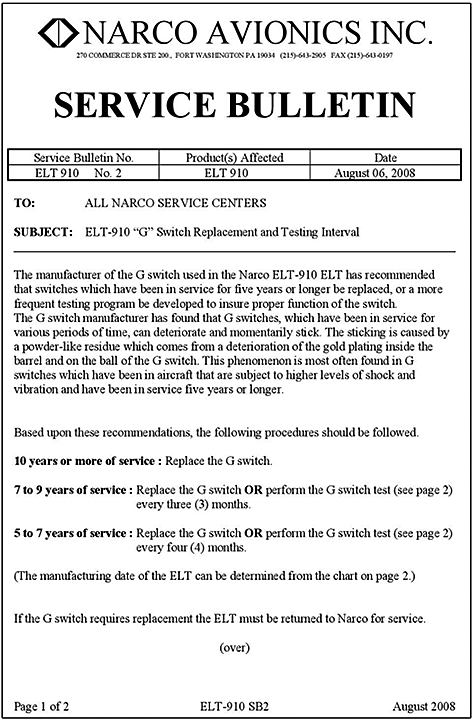

Source: Narco Avionics Inc., Service Bulletin No. ELT 910 No. 2 (06 August 2008), ELT-910 "G" Switch Replacement and Testing Interval.