Collision with terrain
Air Canada
Airbus Industrie A320-211, C-FTJP
Halifax/Stanfield International Airport
Halifax, Nova Scotia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
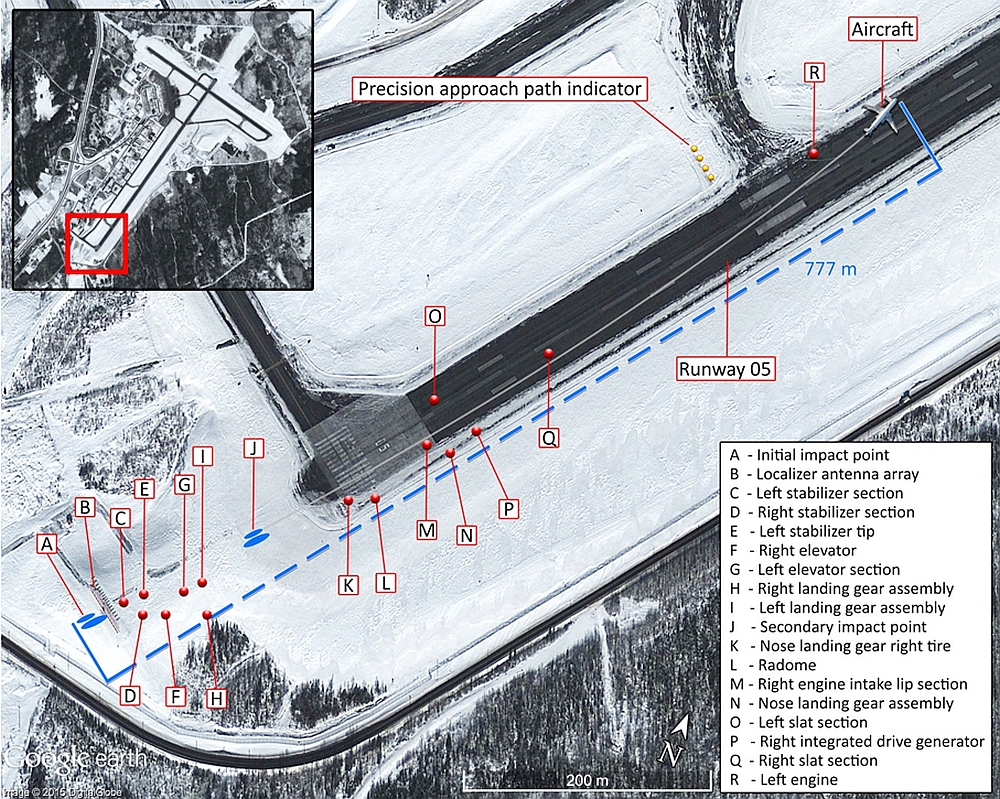
On 29 March 2015, an Air Canada Airbus Industrie A320-211 (registration C-FTJP, serial number 233), operating as Air Canada flight 624, was on a scheduled flight from Toronto/Lester B. Pearson International Airport, Ontario, to Halifax/Stanfield International Airport, Nova Scotia, with 133 passengers and 5 crew members on board. At approximately 0030 Atlantic Daylight Time, while conducting a non-precision approach to Runway 05, the aircraft severed power lines, then struck the snow-covered ground about 740 feet before the runway threshold. The aircraft continued airborne through the localizer antenna array, then struck the ground twice more before sliding along the runway. It came to rest on the left side of the runway, about 1900 feet beyond the threshold. The aircraft was evacuated; 25 people sustained injuries and were taken to local hospitals. The aircraft was destroyed. There was no post-impact fire. The emergency locator transmitter was not activated. The accident occurred during the hours of darkness.
Ce rapport est également disponible en français.
1.0 Factual information
1.1 History of the flight
The International Civil Aviation Organization's (ICAO's) Annex 13 to the Convention on International Civil Aviation requires States conducting accident investigations to protect cockpit voice recordings.Footnote 1 Canada complies with this requirement by making all on-board recordings—including cockpit voice recorders (CVRs)—privileged in the Canadian Transportation Accident Investigation and Safety Board Act. While the Transportation Safety Board of Canada (TSB) may make use of any on-board recording in the interests of transportation safety, it is not permitted to knowingly communicate any portion of an on-board recording that is unrelated to the causes or contributing factors of an accident or to the identification of safety deficiencies.
The reason for protecting CVR material lies in the premise that these protections help ensure that pilots will continue to express themselves freely and that this essential material is available for the benefit of safety investigations. The TSB has always taken its obligations in this area very seriously and has vigorously restricted the use of CVR data in its reports. Unless the CVR material is required to both support a finding and identify a substantive safety deficiency, it will not be included in the TSB's report.
To validate the safety issues raised in this investigation, the TSB has made use of the available CVR information in its report. In each instance, the material has been carefully examined in order to ensure that it is required to advance transportation safety.
An Air Canada Airbus Industrie (Airbus) A320-211, operating as Air Canada flight 624 (AC624), was on a scheduled flight from Toronto/Lester B. Pearson International Airport (CYYZ), Ontario, to Halifax/Stanfield International Airport (CYHZ), Nova Scotia, with 133 passengers and 5 crew members on board.
The instrument flight rules flight was planned to take 2 hours and 09 minutes at 455 knots true airspeed and at a cruise altitude of flight level 350.Footnote 2 The planned alternate airport was Montréal/Pierre Elliott Trudeau International Airport (CYUL), Quebec.
Before departure, Air Canada dispatch provided the flight crew with an operational flight plan that included forecasted and observed weather information for CYHZ, CYUL, and the Greater Moncton Roméo LeBlanc International Airport (CYQM), New Brunswick. The forecast for CYHZ was wind 350° true (°T) at 15 knots with gusts at 21 knots, visibility ½ statute mile (sm)Footnote 3 in moderate snow and drifting snow, and temperature −5 °C.
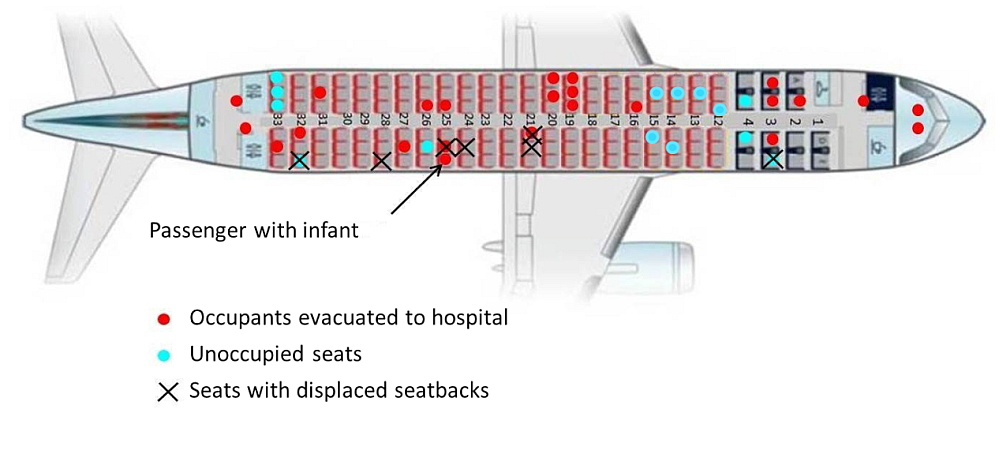
Before departure, the cabin crew conducted a passenger safety briefing, which included instructions for an emergency evacuation and the locations of the 4 cabin doors and the 4 over-wing exits. In the event of an emergency, passengers were directed to leave their carry-on baggage and to follow the emergency lighting along the aisle to the nearest exit. The cabin crew also briefed the passengers seated adjacent to the over-wing exits on how to open these exits should they hear the command to evacuate. A passenger with an infant was briefed on how to hold the infant for takeoff and landing and on the recommended bracing position. Passengers were also instructed to review the safety-features cards located in the seatbacks.
AC624 was airborne at 2205 on 28 March 2015.Footnote 4 The captain occupied the left seat and was the pilot flying (PF), while the first officer occupied the right seat and was the pilot monitoring (PM). This was the first time these pilots had flown together.
During the climb, the flight crew discussed amending the planned alternate airport to CYQM, as this change would allow more time to hold at CYHZ if landing were delayed to wait for the weather to improve. Based on the weather forecast and the notices to airmen (NOTAMs), the flight crew determined that they would conduct the localizer (LOC) approach to Runway 05 in Halifax (Appendix A).Footnote 5
While in cruise, the flight crew calculated the cold temperature corrections for the Split Crow final approach fix (FAF) crossing altitude, the minimum descent altitude (MDA), and the missed approach altitude. It was determined that the FAF crossing altitude would be 2200 feet above sea level (ASL), based on the published altitude of 2000 feet plus a cold temperature correction of 200 feet. The MDA was calculated at 813 feet ASL, based on the published MDA of 740 feet ASL plus a cold temperature correction of 23 feet, plus 50 feet added to the corrected MDA, as required by Air Canada's Flight Operations Manual (FOM).Footnote 6 The flight crew calculated a flight path angle (FPA) based on the temperature-corrected FAF. The calculation was based on the published vertical descent angle of −3.08° obtained from the Jeppesen approach chartFootnote 7 (Appendix A) and Air Canada's Airbus A320 Quick Reference HandbookFootnote 8 for a final calculated FPA of −3.5°.
At about 2256, Air Canada dispatch provided the flight crew with weather updates and advised that, at 2230, an Air Canada flight had landed in CYHZ on Runway 05 after carrying out a missed approach due to insufficient visibility.
The flight crew performed the go-around briefing and repeatedly reviewed the weather conditions at CYHZ. Based on the published runway conditions and the reported winds, and in accordance with the Quick Reference Handbook, they determined that the conditions were suitable for the aircraft to land.
At 2311, the flight crew received the 2300 METAR,Footnote 9 which reported visibility of ¼ sm with heavy snow. According to Air Canada's operations specification (OPS Spec), the flight crew can attempt an approach past the FAF when visibility is reported to be at or greater than ½ sm. The flight crew planned to hold at CYHZ either until the weather improved and an approach could be attempted or until they reached the minimum fuel required to divert to the alternate airport.
At 2321, about 2 minutes after the flight was cleared to descend to flight level 290, the flight crew carried out the approach briefing for a non-precision LOC approach to Runway 05, followed by the pre-descent checklist. These briefings included the corrected altitudes and amended FPA. The approach was to be coupled–selectedFootnote 10 with a manual landing.
During the descent, the flight crew discussed the holding requirements and then contacted the CYHZ terminal controller to request a hold at CETTY.Footnote 11 At 2325, the terminal controller cleared AC624 for a hold at CETTY at 9000 feet ASL. The flight crew determined that there was sufficient fuel to remain in the hold until 0100 on 29 March.
At 2334, the flight crew contacted the CYHZ tower controller for an update on the weather and runway conditions. The tower controller advised that the reported visibility was still ¼ sm and that vehicles were continuing to remove snow from the runway. About 5 minutes later, the aircraft turned right from heading 110° to 325° magnetic (°M) to enter the hold at CETTY.
At 2343, the flight crew began the in-range checks, which included extending the landing lights to ON. The pilot flying (PF) subsequently indicated that he might want the landing lights selected OFF during the approach. The cabin crew then made a passenger announcement, which included instructing passengers to stow their carry-on baggage, put their seatbacks upright, and fasten their seatbelts. The cabin crew subsequently confirmed that these actions had been taken.
At 0000 on 29 March, there was a tower controller shift change.
At about 0007, the PF indicated that, if the weather did not improve within about the next 20 minutes, the flight would have to divert to CYQM.
At 0009, the terminal controller contacted AC624 and provided the latest METAR, which indicated visibility of ⅛ sm, winds of 360°M at 20 knots, gusting to 25 knots, in heavy snow and drifting snow, and vertical visibility of 300 feet (Appendix C). Four minutes later, the tower controller contacted AC624 to advise that the report of ⅛ sm visibility had been incorrect and that the actual visibility was ¼ sm, although the tower controller reported being able to see about ½ sm.
At 0016, the tower controller advised the flight crew of a special weather observation (SPECI) issued at 0013, which included the information that visibility was ½ sm in snow and drifting snow and that vertical visibility was 300 feet. Based on the improvement in visibility to the required minimum, the flight crew determined that they would continue and carry out an approach to Runway 05.
At 0016, the terminal controller cleared AC624 to the intermediate fix ODKAS, 11.6 nautical miles (nm)Footnote 12 from the runway, and cleared the flight to descend to 4000 feet ASL. AC624 was then cleared for the straight-in LOC approach via ODKAS and was advised that there was no change in weather and runway conditions from those previously reported. The flight crew continued the approach and, at about 0022, the landing lights were selected OFF, which turned the lamps off.
Less than a minute later, AC624 contacted the tower to confirm that the runway lights were on setting 5. The tower controller, who was dealing with the snowplows on the runway and an aircraft taxiing for Runway 05, indicated that the lights were currently on setting 4, but would be on setting 5 in time for the landing.
At 0023, AC624 levelled off at 3400 feet ASL about 12 nm from the threshold. Once level, with the autopilot (AP) on and the flight director lateral mode selected to LOC (localizer track mode), the flight crew began to configure the aircraft for the descent with AP 1 and autothrust still engaged. The flaps were set to Flaps 1.
At 0024, approximately 11 nm from the runway threshold, the flaps were set to Flaps 2. The aircraft initiated a left turn to intercept, capture, and track the LOC.Footnote 13 During this time, the flight crew noted that the ground could be seen when looking straight down as well as when looking off on a slight angle.Footnote 14
At approximately 0026, about 8 nm from the runway threshold, the PF called for the landing gear to be extended and for the landing checks to be completed. The aircraft levelled off at 2200 feet ASL, the landing gear was extended, and the missed approach altitude was set. At about the same time, the tower controller requested that the snowplows vacate the runway.
At 0027, about 6.7 nm from the runway threshold, the flaps were set to Flaps 3 followed by Flaps full. The aircraft was fully configured for landing before the FAF.Footnote 15
About 2.7 nm from the FAF, using the vertical speed/flight path angle (V/S-FPA) knob on the flight control unit, the PF selected FPA mode; the aircraft was now being flown with the FPA selected to 0.0°.Footnote 16
At 0027, the PM began the countdown for the distance to the FAF, indicating 0.5, 0.4, then 0.3 nm. At 0.3 nm from the FAF, the PF rotated the V/S-FPA knob to select −3.5°. The tower controller cleared AC624 to land; the runway lights remained at setting 4.Footnote 17 The aircraft landing lights remained OFF, and the PM indicated that ground lighting was noted.
The aircraft started to descend about 0.2 nm from the FAF. The aircraft crossed the FAF at 2170 feet indicated altitude (Figure 1).
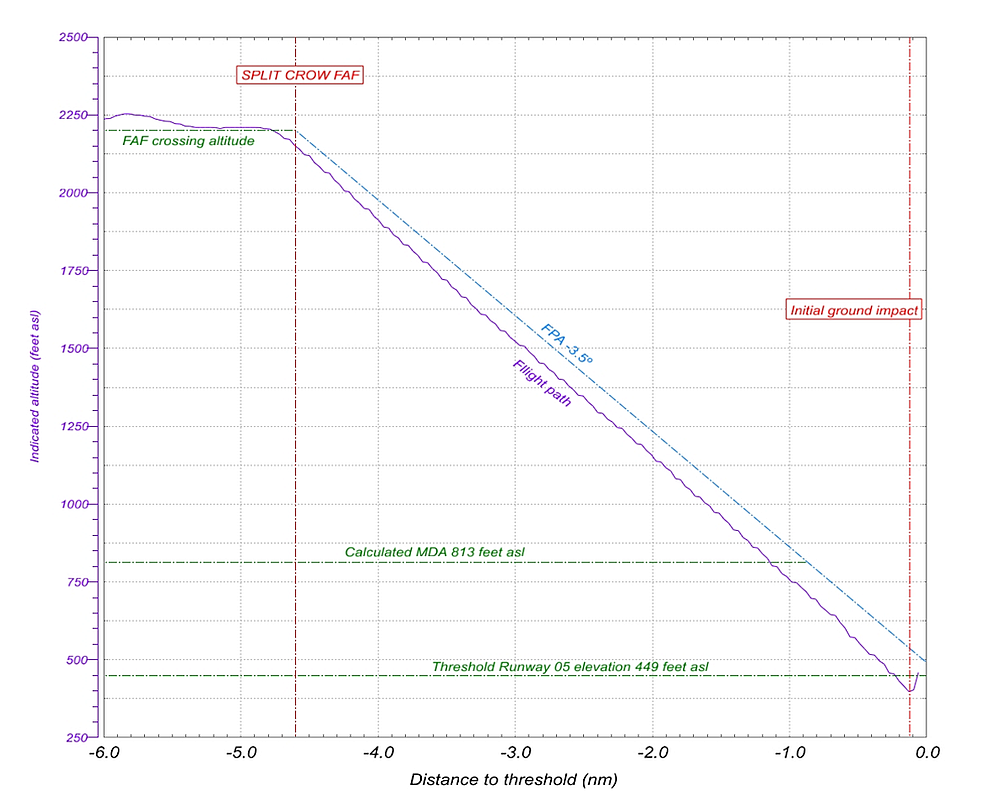
As the aircraft descended, the actual flight path diverged from the desired profile as a result of wind variations. The divergence continued to increase throughout the approach. The airspeed was constant, and the vertical descent speed ranged between 700 and 800 feet per minute (fpm).
At 0029:27, a radio altimeter automated audio call (automated call) of "400" was made, indicating that the aircraft was 400 feet above the terrain. Almost immediately after this call, the aircraft crossed the calculated MDA at 1.2 nm from the threshold. The PM observed some approach lights and called, "Minimum, lights only," when the aircraft was about 1.0 nm from the threshold. The PF immediately called, "Landing," and began to observe some approach lights. By this time, the aircraft had crossed the published MDA (740 feet ASL) and was 0.3 nm farther back than the published distance. The autopilot remained engaged as the aircraft continued descending, and there was no reduction in the descent rate.
When the aircraft was about 0.7 nm from the threshold, the flight crew had a conversation in which both confirmed they could see some approach lights. At this time, the aircraft crossed over a lighted facility.
At 0029:47, the landing lights were selected ON, followed in very quick succession by the PF disconnecting the autopilotFootnote 18 an automated call of "100," an automated call of "50," and the PM instructing to pull up. AC624 then severed the electrical power line that ran perpendicular to the runway,Footnote 19 causing a utility power outage at the airport terminal.
About 1 second before initial ground impact, the PF advanced the thrust levers to the takeoff go-around detent and pulled the side-stick to the full nose-up position. One of the left main tires contacted an approach light located 861 feet from the runway threshold. At 0030:00, the aircraft's main landing gear, aft lower fuselage, and left engine cowling struck the snow-covered ground on the south side of the embankment that sloped up toward the runway surface. The aircraft then struck the localizer antenna array and continued airborne before striking the ground twice more and then sliding along the runway. The aircraft came to rest about 1900 feet beyond the threshold. During these movements, the aircraft completely lost electrical power. The lights inside the cabin went off and the emergency lights activated automatically.
At 0030:16, the tower controller activated the crash alarm.
Although no evacuation order was given, passengers in rows 17 and 18 opened the 4 over-wing exits and began to exit the aircraft. The service director opened the forward left cabin (L1) door and directed the passengers to exit the aircraft.Footnote 20 The slides at the cabin door and the over-wing exits deployed when the exits were opened.
About 2 minutes after the crash alarm was activated, while passengers were completing the evacuation, firefighters with the airport emergency response services (ERS) arrived at the accident site, in accordance with the response requirements in the regulations.Footnote 21
All of the passengers had exited the aircraft within 5 minutes after it came to a stop, many wearing open-toed shoes, shorts, and t-shirts. Some passengers exited the aircraft with their carry-on baggage. All occupants were grouped about 200 m behind the aircraft. Occupants with more severe injuries sat in the emergency response vehicles. Some passengers, as well as the airport's emergency response duty manager, made telephone calls to the 911 emergency number.
At about 0042, the firefighters confirmed that all occupants had evacuated the aircraft and requested that transportation be provided to bring the aircraft occupants to a shelter. About 50 minutes after the aircraft had come to a stop, all of the remaining passengers were transported to an indoor holding area.
1.2 Injuries to persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | 0 | 0 | – | 0 |
| Serious | 1 | 0 | – | 1 |
| Minor | 4 | 20 | - | 24 |
| None | 0 | 113 | – | 113 |
| Total | 5 | 133 | – | 138 |
1.3 Damage to aircraft
The aircraft was destroyed.
1.4 Other damage
Before the initial impact, power lines across the approach path were severed and an approach light was damaged. The instrument landing system (ILS) localizer antenna structure was destroyed when it was struck by the aircraft. The soil adjacent to the runway where the aircraft came to rest was contaminated by a small amount of fuel, and the runway had multiple scrapes due to the aircraft and the left engine sliding along it.
1.5 Personnel information
1.5.1 Flight crew
| Captain | First officer | |
| Pilot licence type | Airline transport pilot licence (ATPL) | Airline transport pilot licence (ATPL) |
| Medical expiry date | 01 Feb 2016 | 01 Apr 2016 |
| Total flying hours | 11 765.8 | 11 300.0 |
| Flight hours on type | 5755.0 | 6392.0 |
| Flight hours in the last 7 days | 8.0 | 20.4 |
| Flight hours in the last 30 days | 22.6 | 45.4 |
| Flight hours in the last 90 days | 103.0 | 115.0 |
| Flight hours on type in the last 90 days | 103.0 | 115.0 |
| Hours on duty prior to the occurrence | 4.0 | 9.5 |
| Hours off duty prior to the work period | 21.0 | 12.9 |
The flight crew were certified and qualified for the flight in accordance with existing regulations.
1.5.1.1 Captain
The captain had over 9 years of experience at Air Canada and had flown as a first officer (FO) on the A320 for about 7 years before he had qualified as captain in 2013. As a captain, he had flown about 1200 hours as pilot-in-command.
During the 3 days before the accident, the captain had been working evening shifts. The captain had started work on 26 March on an evening flight, which had a duty day of 3 hours, followed by 17 hours off duty. On the evening of 27 March, the captain had worked a duty day of 4 hours, followed by 21 hours off duty, before reporting for duty on 28 March.
1.5.1.2 First officer
The FO had 15 years of experience at Air Canada and had flown as an FO on the A320 since being hired.
During the 3 days before the accident, the FO was off duty until the start of a pairing on 27 March. The FO had a duty day of 10 hours, followed by almost 13 hours off duty, and had been on duty for 9.5 hours when the accident occurred.
1.5.2 Cabin crew
The cabin crew, consisting of a service director and 2 flight attendants, were certified and qualified for the flight in accordance with existing regulations.
The service director had 10 years of experience at Air Canada, which included 5 years as a flight attendant and 5 years as a service director. The service director had completed the Air Canada Annual Recurrent Training (ART) in July 2014. The service director occupied an aft-facing jump seat at the L1 door and was responsible for both the L1 and R1 doors.
The first flight attendant, who was seated in an aft-facing jump seat at the L2 door, had 5 years of experience and had completed the ART in April 2014.
The second flight attendant, who was seated in a bulkhead-mounted forward-facing jump seat located in the aft aisle, had 2 years of experience and had completed the company's 3-week initial training course in May 2014.
1.6 Aircraft information
| Manufacturer | Airbus Industrie |
|---|---|
| Type, model and registration | Aeroplane, A320-211, C- FTJP |
| Year of manufacture | 1991 |
| Serial number | 233 |
| Certificate of airworthiness issue date | 15 October 1991 |
| Total airframe time | 75 103 hours |
| Engine type (number of engines) | Turbo fan, CFM56-5A1 (2) |
| Maximum allowable takeoff weight | 75 500 kg |
| Recommended fuel type(s) | Jet A, Jet A-1, Jet B |
| Fuel type used | Jet A |
1.6.1 General
The Airbus A320-211 is a twin-engine, narrow-body, single-aisle passenger transport aircraft. It has a retractable landing-gear system, which includes 2 main landing gear (MLG) and 1 nose landing gear.
The aircraft cabin was equipped with 5 retractable flight-attendant jump seats. Two wall-mounted aft-facing jump seats were located at the L1 door; a bulkhead-mounted, forward-facing jump seat was located in the aft aisle; and wall-mounted aft-facing jump seats were located on each side of the aft galley.
Overhead stowage bins were installed along the cabin sidewalls throughout the cabin seating area.
The aircraft was equipped with a Honeywell International Inc. (Honeywell) enhanced ground proximity warning system (EGPWS). Because the approach conditions did not exceed the boundaries of safe operation, the EGPWS did not provide a warning.
The aircraft was equipped with 2 survival-type (S-type) emergency locator transmitters (ELTs). The S-type ELT is crew-deployable and activates automatically when immersed in water. The S-type ELT can also be activated manually by a switch on the ELT itself. Because the aircraft location was known and emergency response was underway, there was no need for the crew to manually activate an ELT.
Records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. With the exception of an inoperable no. 2 air pack flow indication, which had been deferred in the defect logbook,Footnote 22 there were no reports of technical difficulties before the occurrence flight, nor was there any indication of a component or system failure during the flight. The weight and centre of gravity were within prescribed limits.
1.6.2 Airbus A320 systems and operation
The A320's primary flight display (PFD) presents aircraft flight parameters such as attitude, airspeed, and altitude. It also provides flight guidance information, such as the flight path vector, referred to as the "bird." The bird can be used as the flying reference and appears on the PFD as a green symbol resembling an aircraft (Figure 2).

The flight mode annunciator, which appears across the top of the PFD, is the primary indicator of the selection status of the flight control unit. The flight mode annunciator displays the autothrust mode, the vertical and lateral modes of the autopilot and flight director, and the approach capabilities, as well as the engagement status of the autopilot, flight director, and autothrust.
The flight control unit, which is the primary interface between the flight crew and the autoflight system for short-term selection (Figure 3), is located in the centre area of the glare shield. Flight crew operation of the flight control unit can modify any current flight parameters temporarily and can also select operational modes for the autopilots and flight directors. The specific mode is displayed on the flight mode annunciator portion of the PFD.
The flight control unit has 4 knobs (SPD-MACH [speed/Mach number], HDG-TRK [heading/track], ALT [altitude], and V/S-FPA [vertical speed/flight path angle]) for the manual selection of autoflight speed and of lateral and vertical modes. The knobs are pushed to switch that segment of autoflight guidance to managed mode, in which the flight management system (FMS) guides the aircraft along a programmed route and along vertical, lateral, and speed profiles.
Using the knobs, the flight crew can set the desired speed, heading/track, altitude, or vertical speed/FPA. The knob must be pulled to activate the selected guidance.
When rotated, the V/S-FPA selector knob (the knob to the far right in Figure 3) changes the vertical speed or FPA in the V/S-FPA window. Pulling the selector knob engages the V/S or FPA function; the aircraft is then guided along the selected vertical path. V/S or FPA is selected by pushing the HDG V/S–TRK FPA pushbutton.

1.6.3 Electrical power
During normal operation, 2 alternating current (AC) generators, one driven by each engine, supply aircraft electrical power. A third generator, driven by an auxiliary power unit, can replace either or both of the main AC generators at any time.
If all 3 of these generators fail to supply power and the aircraft speed is above 100 knots, a ram air turbine (RAT) extends automatically. The RAT powers an emergency generator by means of a hydraulic motor.
If all AC generation is lost, the system can transform direct current (DC) power from the aircraft's 2 main batteries into AC power by means of static inverters.
1.6.4 Cabin doors and over-wing exits
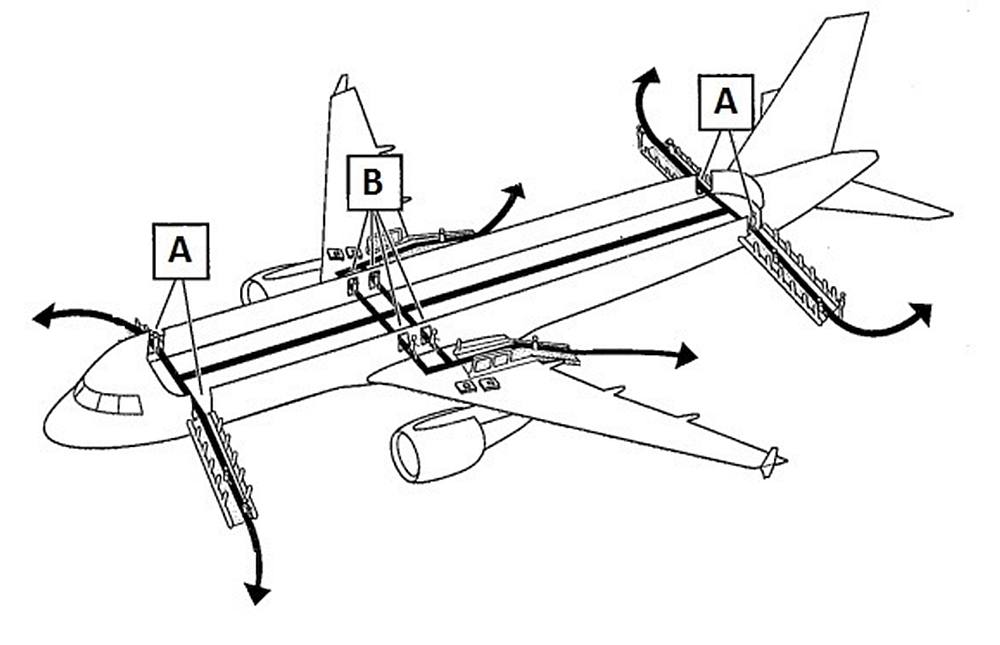
The cabin doors and over-wing exits are equipped with automatically inflating slides/rafts (hereafter referred to as slides). When a cabin door that is in the armed position is opened, the slide automatically inflates. When an over-wing exit is opened, the over-wing slide inflates automatically (Figure 4).
The cabin doors open outward and forward. During normal operation, when opened from the inside, the door is unlocked by moving the door control handle upward to the OPEN position. With the slide arming lever in the disarmed position, the door movement is dampened by a hydraulic actuator. With the slide arming lever in the armed position, such as when opening the door during an emergency, the actuator automatically opens the door to the locked position. A gust lock engages when the door is in the locked position.
A vertically oriented pushbutton releases the gust lock when pushed downward. Once the gust lock is released, the door is free to move. The pushbutton to release the L1 door gust lock is located on the door support arm, adjacent to the attendant station (Figure 5).

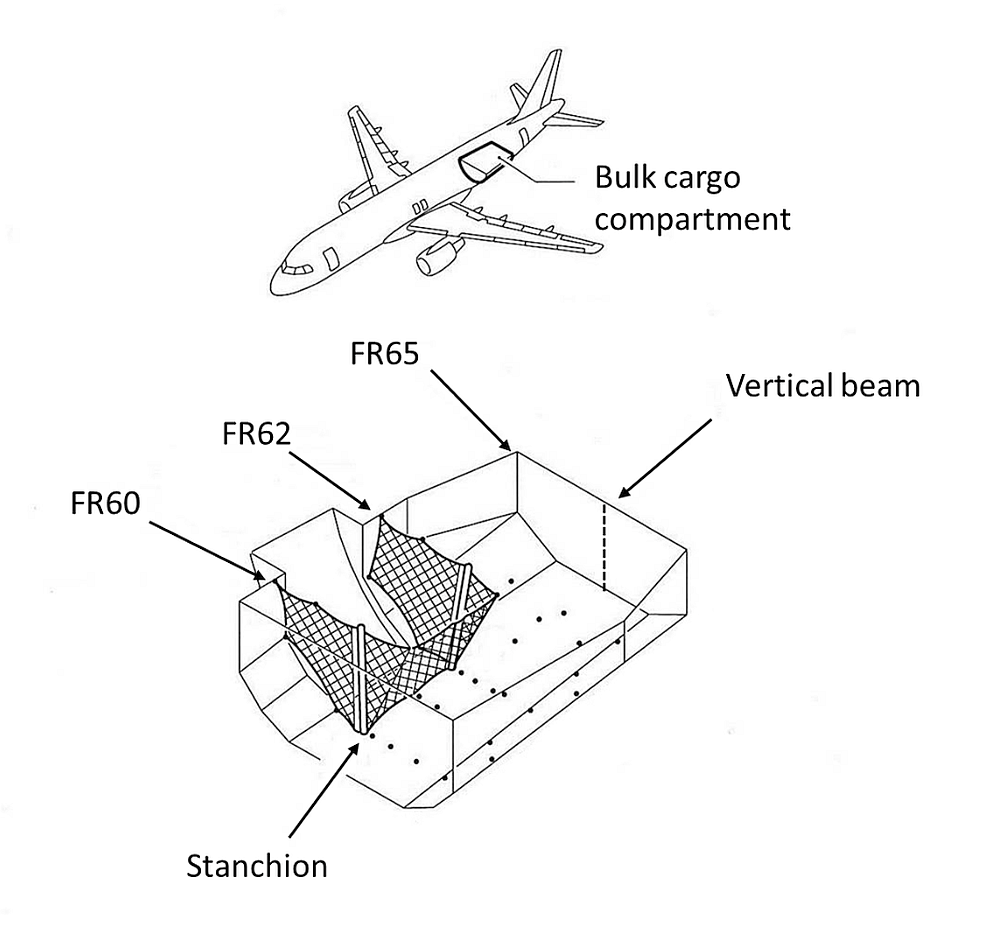
1.6.5 Bulk cargo compartment
The bulk cargo compartment is located below the cabin floor behind the aft cargo compartment and is accessed by a door on the right side of the fuselage. A divider net isolates the bulk cargo compartment from the aft cargo compartment, and a removable non-structural partition, located at frame (FR) 65, serves as the aft wall of the bulk cargo compartment. This partition incorporates a one-piece non-structural vertical beam installed between the cargo compartment floor and ceiling, on the aircraft's centre line.
Door nets are installed forward and aft of the bulk cargo compartment door, at FR60 and FR62. These nets have one-piece stanchions that extend between the cargo compartment floor and ceiling (Figure 6).
1.6.6 Passenger seats
The occurrence aircraft was configured with 14 business-class seats and 132 economy-class seats. The business-class seats consisted of double-seat units with 3 rows (rows 2 to 4) installed left of the centre aisle and 4 rows (rows 1 to 4) installed on the right. The economy-class seats consisted of triple-seat units installed on either side of the aisle in 22 rows (rows 12 to 33) aft of the business-class section.
During normal operation, the seatbacks in both business and economy class can be retained in the upright position or reclined rearward. The seatback-reclining mechanism incorporates a shear pin, which is designed to shear when the seatback is struck from behind. The shear pin will shear when about 190 pounds of force is applied at the top of the seatback in the forward direction. This force corresponds to an inertial load on the seatback of about 20g;Footnote 23 under this condition, the seat frame would also be damaged and deformed.
The shearing action allows the impact energy to dissipate, mitigating the risk of injury during an accident. Once the pin is sheared, the seatback is free to pivot about its hinge points.
1.6.7 Flight crew shoulder-harness assembly
The flight crew restraint system, consisting of the shoulder-harness assembly and lap belt, is designed to restrain the occupant of the seat during all flight attitudes and landings. The shoulder harness and belt come together at a rotary buckle; the lap belt can be used separately or with the shoulder harness.
The shoulder harness incorporates 2 straps, each connected to an emergency locking retractor (automatic inertia reel). A recoil spring within the inertia reel rolls up each strap onto the spool when the straps are not fastened to the buckle.
When the straps are fastened to the buckle, the inertia reels extend and retract the shoulder harness as required to allow unrestricted movement of the occupant. When a sudden acceleration force is applied to the shoulder harness, the inertia reel's locking mechanism activates. The locking mechanism incorporates a latch that pivots about a plastic flange directly attached to the spool. When the latch engages, it causes a load bar to lock the spool through a ratcheting mechanism, thereby preventing further movement of the strap. When the force is relieved, the inertia reel unlocks, allowing unrestricted occupant movement.
The maintenance manual for the restraint system provides procedures to evaluate the performance of the system when it is installed on an aircraft. According to these procedures, the restraint system should be inspected at intervals concurrent with the inspections of the on-aircraft seats.
The manual, which was not available to Air Canada, states that, when conducting a test to verify the inertia reel's ability to lock as a result of acceleration (a pull test), a minimum of 25% of the strap must be extended before accelerating the strap. This test is to be carried out 4 consecutive times to verify that the locking system functions correctly. Performing a pull test verifies that the shoulder harness is airworthy and capable of restraining the seat occupant when subjected to a sudden acceleration force, such as during an accident. If the inertia reel fails the test, then it is no longer serviceable and must be replaced.
When the shoulder harness is fully retracted, the strap interferes with the load bar and prevents it from engaging the ratchet. Once the strap has been extended by the required 25%, the load bar is free to engage the ratchet. Failure to extend the strap before a pull test will result in the flange and latch being subjected to excessive forces, normally absorbed through the load bar, which can result in the flange fracturing.
Air Canada standard operating procedures (SOPs) do not require flight crews to perform a pull test. The company's approved maintenance schedule includes an inspection of the restraint system of the flight crew seats at every A-Check (that is, at intervals of 600 to 750 flight hours). This requirement does not specify that a shoulder harness pull test be carried out as part of the inspection. The last inspection of the FO's restraint system had been carried out approximately 2 weeks before the accident; no discrepancies were noted.
Neither the Air Canada task cards, nor the Airbus maintenance task cards they are based on, specified a requirement to perform a pull test. However, Air Canada recognized the importance of the shoulder harness in restraining the seat occupant during an accident, and performed pull tests nonetheless. Air Canada did not know that the seatbelt was required to be tested from the 25% extended position and so, tested the harness in the fully retracted position.
In June 2014, the FO seat was installed in the occurrence aircraft after having been repaired at an approved facility. Although the seat manufacturer's maintenance instructions included a function test of the inertia reel, they did not state that a minimum of 25% of the strap was to be extended before performing the test.
1.6.8 Coffee-maker assemblies
On the occurrence aircraft, there were 3 coffee-maker assemblies (brewers) located side by side in the aft galley.
Each brewer slides into rails that are part of a permanently mounted base affixed to the aircraft structure. A locking device, which consists of a moveable lever and a locking pin, is incorporated in the brewer's housing. The locking device is spring-loaded to the open position. The lever incorporates a slotted track to which the upper end of the pin is attached.
When the lever is pushed, the upper end of the pin moves toward the lower portion of the track, and the pin is pushed through the brewer housing into a hole in the rail. When the upper end of the pin engages the detent at the end of the track, the pin is in the locked position and properly engaged in the rail. In this locked position, the lever is vertical and does not make contact with the brewer housing. The lever must be in the locked position for a coffee pot or teapot to be placed on the warming element. During normal operation, pots of coffee or tea are removed from the brewers for taxiing, takeoff, and landing.
Pulling the lever causes the upper end of the pin to move out of the detent. The spring then pushes the pin upward, which causes the lever to move toward the open position. When unlocked, the brewer is free to slide forward on its rails.
If the brewer is not correctly installed in its mounting base, the pin will contact the rail, preventing the lever from moving to the locked position. If excessive force is applied to the lever, or if the lever is struck by a hard object, then the lever will bend rearward.
The brewer manufacturer recommends periodic maintenance, which includes a general visual examination of the complete assembly. There is no specific requirement to verify that the locking mechanism operates correctly.
In 1992, the manufacturer of the brewer issued an optional service bulletin that provided information on modifying the brewer to incorporate a new locking lever. The new lever is retained in the locked position by means of a screw that is threaded into the housing. When the screw is in place, the lever cannot be opened. Air Canada did not incorporate this service bulletin, nor was it required to do so by regulation.
1.6.9 Passenger address system
The aircraft was equipped with a passenger address (PA) system that allowed flight personnel to make announcements to passengers in the cabin through loudspeakers. The PA system can be operated from the cockpit or from the flight attendant stations.
The PA system does not have an independent power supply that would allow for continued operation in the event of an emergency that causes a complete loss of electrical and battery power, nor is such a power supply required by regulation.
1.6.10 Cabin emergency lighting system
The aircraft was equipped with an emergency lighting system that automatically activates in case of a loss of electrical power. When activated, the marking system for the proximity emergency escape path is powered by an independent power supply (using internal batteries) for at least 12 minutes.
1.7 Meteorological information
1.7.1 General
Weather observations at Halifax are issued by NAV CANADA flight service specialists. The flight service specialist conducts hourly weather observations and, in the case of significant changes in weather conditions, releases special weather observations. To determine prevailing ground visibility at night, unfocused lights of moderate intensity at known distances are used for visibility markers.
1.7.2 Halifax weather forecasts received by the flight crew before departure
Air Canada dispatchers prepared the operational flight plan, including weather and NOTAM information, and provided it to the flight crew.
The METAR, issued 28 March 2015 at 2000 read: wind 360°T at 19 knots, with gusts at 26 knots, visibility 1½ sm in light snow and drifting snow, overcast cloud at 700 feet above ground level (AGL), temperature −4 °C, dew point −5 °C, and altimeter 29.60 inches of mercury (in. Hg).
The aerodrome forecast (TAF), issued 28 March 2015 at 1744, for the period of arrival was as follows: wind 010°T at 20 knots, with gusts at 30 knots, visibility ¾ sm in light snow and blowing snow, and vertical visibility 500 feet AGL; temporarily between 28 March 1800 and 29 March 0300: visibility 3 sm in light snow and blowing snow, and overcast cloud at 1000 feet AGL.
1.7.3 Halifax weather forecasts issued before departure
The METAR for CYHZ, issued 28 March 2015 at 2200 included the following: wind 350°°T at 15 knots, with gusts at 21 knots, visibility ½ sm in moderate snow and drifting snow, vertical visibility 200 feet AGL, temperature −5 °C, dew point −6 °C, and altimeter 29.62 in. Hg.
A TAF for CYHZ was issued on 28 March 2015 at 2038. Weather at the time of arrival was forecast as follows: wind 360°T at 20 knots, with gusts at 30 knots, visibility ¾ sm in light snow and blowing snow, and vertical visibility 500 feet AGL; temporarily between 29 March 0000 and 0500: visibility 3 sm in light snow, and overcast cloud at 1200 feet AGL.
1.7.4 Halifax weather forecasts issued while AC624 was enroute
The CYHZ METAR for 2300 was as follows: wind 350°T at 19 knots, with gusts to 27 knots, visibility ¼ sm in heavy snow, vertical visibility 200 feet AGL, temperature −6 °C, dew point −6°C, and altimeter 29.62 in. Hg.
At 2338, the CYHZ TAF was amended; for the period of arrival, it was as follows: wind 350°T at 20 knots, with gusts at 30 knots, visibility ¼ sm in moderate snow and blowing snow, and vertical visibility 200 feet AGL; between 29 March 0300 and 0400: visibility 2 sm in light snow and blowing snow, and overcast cloud at 1000 feet AGL.
The METAR at 0000, provided to the flight crew by NAV CANADA at 0009, was as follows: wind 340°T at 19 knots, with gusts at 25 knots, visibility ⅛ sm in heavy snow and drifting snow, vertical visibility 300 feet AGL, temperature −6 °C, dew point −7 °C, and altimeter 29.62 in. Hg. The 0000 METAR was subsequently corrected to a visibility of ¼ sm, and the information was provided to the flight crew by NAV CANADA at 0013.
A SPECIFootnote 24 for CYHZ, issued at 0013 and provided to the flight crew by NAV CANADA at 0015, was as follows: wind 350°T at 20 knots, with gusts at 26 knots, visibility ½ sm in moderate snow and drifting snow, vertical visibility 300 feet AGL, temperature −6 °C, dewpoint −7 °C, and altimeter 29.63 in. Hg.
1.7.5 Halifax weather forecasts issued after the accident
A weather observation taken at 29 March 0055 for CYHZ was as follows: wind 340°T at 22 knots, with gusts at 28 knots, visibility ¾ sm in light snow and drifting snow, broken cloud at 700 feet AGL, overcast cloud at 1000 feet AGL, temperature −6 °C, dew point −6 °C, and altimeter 29.62 in. Hg. This observation was not recorded as a SPECI since an updated METAR was being issued at 0100 (5 minutes later).
The 29 March 0100 METAR indicated wind 340°T at 21 knots, with gusts at 54 knots. The human weather observation system had recorded a gust at this speed. However, the wind and altimeter digital display system never indicated a gust greater than 40 knots. As well, the tower controller indicated that no gusts that strong had been registered. The flight service specialist suspected that the gust at 54 knots was erroneous and advised the technical operations supervisor. A SPECI was issued at 0114 that reported gusts to 33 knots.
1.8 Aids to navigation
Navigational aids serving the 4 available approaches at CYHZ include:
- area navigation (RNAV) for all 4 runways;
- category IIFootnote 25 ILS for Runway 23;
- non-directional beacon (NDB) and LOC for Runway 05; and
- category IFootnote 26 ILS and distance measuring equipment for Runway 14.
The occurrence aircraft was equipped with the appropriate navigational aids to conduct a LOC non-precision approach, and these aids were serviceable at the time of the accident.
1.9 Communications
No difficulties with the quality of radio transmissions were noted throughout the flight.
1.10 Aerodrome information
1.10.1 General
CYHZ has 2 asphalt runways: Runway 05/23 is 10 500 feet in length, and Runway 14/32 is 7700 feet in length.
Runway 05 is oriented 053°M and has an upslope throughout the touchdown zone. The threshold elevation is 449 feet ASL, and the highest elevation within the touchdown zone is 463 feet ASL.Footnote 27 The runway is serviced by a precision approach path indicator (PAPI) that projects a 3° slope and is suitable for aircraft with an eye-to-wheel height of 45 feet. The PAPI is located on the left side of the runway, approximately 1300 feet from the threshold.
Runway 05 is equipped with a high-intensity lighting system, which includes threshold, end, centre-line, and edge lighting, and a medium-intensity omnidirectional approach lighting system (ODALS) extending 1500 feet from the threshold (Appendix D).Footnote 28 The ODALS includes 5 lights spaced approximately 300 feet apart, which flash sequentially every second (60 times per minute). Runway 05 is not equipped with runway visual range (RVR) sensor equipment.
Runway 23 is equipped with centre-line lighting and centre-row high-intensity approach lighting extending 2400 feet from the threshold. It is also equipped with 2 RVR sensors: RVR A is located adjacent to the runway threshold, and RVR B is located approximately midway down the runway.
Runway 14 is equipped with a simplified short approach lighting system, with runway alignment indicator lights extending 2400 feet from the threshold. There is no centre-line lighting. Runway 32 is equipped with an ODALS.
1.10.2 Approach and runway lighting
1.10.2.1 General
High-intensity lighting systems have 5 intensity settings (1 through 5, with 5 being the brightest) and ODALS have 3 intensity settings (1 through 3, with 3 being the brightest).
According to NAV CANADA's Air Traffic Control Manual of Operations (ATC MANOPS),Footnote 29 when visibility is less than ½ sm at night, the high-intensity runway edge and centre-line lights should be at setting 4 and the ODALS should be at setting 3. When visibility is less than 1 sm at night, the runway edge and centre-line lighting should be at setting 3, and the ODALS at setting 3. The tower controller can select the brightness in accordance with ATC MANOPS or with pilot request.
According to Transport Canada's (TC's) Aerodrome Standards and Recommended Practices,Footnote 30 setting 5 of the high-intensity lighting system provides 100% of the required output and setting 4 provides 25% of the required output; setting 5 is thus 4 times brighter than setting 4.
The required output of setting 3 of the ODALS is more than 3 times greater than setting 2.
1.10.2.2 CYHZ lighting system
In 2007, the control tower at CYHZ was equipped with a system designed to provide control and monitoring of the airfield lighting through a touchscreen display. Preset brightness-setting buttons are used to switch multiple lighting circuits at the same time.
When the Runway 05 preset button for brightness setting 5, identified as "05/23 edge 5," was selected, the runway edge and centre-line lights and the ODALS were switched to their brightest setting, as required by ATC MANOPS.
When the Runway 05 preset button for brightness setting 4, identified as "05/23 edge 4," was selected, the runway edge and centre-line lights were switched to setting 4 and the ODALS were switched to setting 2. The investigation noted that this automatic selection was not in accordance with the ATC MANOPS requirement to have the ODALS on setting 3. This discrepancy was also noted on Runway 14/32.
Thus, the system to control the airfield lighting's preset selections for brightness setting 4 was not in accordance with the ATC MANOPS requirement for the ODALS to be at its brightest settings.
At the time of the occurrence, the PAPI was on setting 4 and had been on this setting since the morning of the previous day.Footnote 31
1.10.2.3 CYHZ lighting brightness estimates
TC has indicated that, based on the weather conditions at the time of the occurrence and the assumptions identified below, the high-intensity lights could theoretically be seen at about 0.97 nm at setting 4, and about 1.13 nm at setting 5. The ODALS could theoretically be seen at about 0.92 nm at setting 2, and about 1.08 nm at setting 3. These distances were calculated based on the following assumptions:
- the prevailing visibility of ½ sm can be used to define the transmissivity of the atmosphere available to the pilot landing on Runway 05;
- the transmissivity can also be applied to the slant visual range when the pilot is above the airport elevation; and
- the minimum illuminance for the pilot to just see the lights is that defined in the ICAO Aerodrome Design Manual, Part 4.Footnote 32
1.11 Flight recorders
The aircraft was equipped with a Honeywell solid-state digital flight data recorder (DFDR) (model SSFDR, part no. 980-4700-042, serial no. SSFDR-16686) and a Honeywell solid-state cockpit voice recorder (CVR) (model SSCVR, part no. 980-6022-001, serial no. CVR120-16303).
The DFDR records approximately 400 parameters and contained approximately 108 hours of flight data, covering the occurrence flight and 26 previous flights. The DFDR data were successfully downloaded.
The CVR had a recording capacity of 120 minutes, and its recorded data included the occurrence flight. The CVR memory was downloaded successfully and contained good-quality audio recording of the occurrence flight.
Electrical power to the CVR was lost at about the time of the second impact, and power to the DFDR was lost about 3 seconds later, when the no. 1 engine separated from the aircraft. The CVR did not have its own independent power supply, nor was such a power supply required by regulation.
1.11.1 Independent power source for cockpit voice recorders
In 1999, during its investigation into the September 1998 occurrence involving an in-flight fire leading to collision with water in Peggy's Cove, Nova Scotia,Footnote 33 the TSB found that one of the aircraft's shortcomings was the lack of a dedicated independent power supply to power the CVR in the event that normal aircraft power sources to the CVR were interrupted. Therefore, the Board recommended to both TC and the European Joint Aviation Authorities that
As of 01 January 2005, for all aircraft equipped with CVRs having a recording capacity of at least two hours, a dedicated independent power supply be required to be installed adjacent or integral to the CVR, to power the CVR and the cockpit area microphone for a period of 10 minutes whenever normal aircraft power sources to the CVR are interrupted.
Transportation Safety Recommendation A99-03
The TSB assessed TC's latest response to Recommendation A99-03 as follows:
The TSB made this recommendation over 15 years ago. In earlier responses, Transport Canada indicated it would amend the CVR regulations subject to harmonization with the FAA [Federal Aviation Administration] rules. The final FAA rule was issued in March 2008, stating that, by April 2012, the CVRs must have a 2-hour recording capacity. In September 2010, the TSB indicated that: "Given the protracted activities required to prepare an NPA [Notice of Proposed Amendment], receive approval through the CARAC [Canadian Aviation Regulation Advisory Council] process, and implement regulatory change, it would appear unlikely that TC can promulgate an amendment to the CARs [Canadian Aviation Regulations] that would match the FAA's implementation date of 07 April 2012."
In December 2012, Transport Canada assured the TSB that "…our commitment to respond to this recommendation remains a priority."
In its latest response [November 2015], Transport Canada indicates that it plans to pre-publish these regulations in the spring of 2016. It further explains its rationale for these delays. In the meantime, the CARs will continue to lack harmonization with both the FAR [Federal Aviation Regulations] requirement and the ICAO standard.
EASA [the European Aviation Safety Agency] reviewed its actions to date in response to Recommendation A99-03. The latest version of EASA rulemaking tasks RMT.0308 and RMT.0249 would indicate that implementation is now scheduled for 01 January 2019.
While Transport Canada's proposed measures are reasonable, the protracted delays are not.
Therefore, the assessment rating for this recommendation is changed to Unsatisfactory.Footnote 34
In October 2016, TC advised that the original Notice of Proposed Amendment had been replaced and that a new Notice of Proposed Amendment is expected to be published in the Canada Gazette, Part I in the summer of 2017.
If aircraft CVR installations do not have an independent power supply, additional, potentially valuable information will not be available for an investigation.
1.12 Wreckage and impact information
1.12.1 Impact
The force of the initial impact crushed sections of the lower aft fuselage and caused the lower portion of both main landing gear to fracture and separate. Each separated portion of the main landing gear struck the corresponding horizontal stabilizer, causing large sections of the stabilizers, as well as the left elevator, to detach. These fragments were found along the debris field before the location of the second impact.
After striking the ILS localizer antenna array, the aircraft continued airborne until the right engine and nose section struck the snow-covered ground. The right engine mounting pylon fractured; the separated engine was retained under the right wing. The nose landing gear collapsed rearward, and its lower portion fractured and separated.
The aircraft then bounced before contacting the runway. The left engine completely detached from the wing and came to rest on the left side of the runway. The aircraft stopped on the left side of the runway in a slight nose-up and left-bank attitude, on an approximate heading of 025°M (Figure 7).
1.12.2 Wreckage
1.12.2.1 General
The nose wheel well area was forced upward and rearward, buckling and fracturing many of the internal structural components. The fuselage sustained multiple dents, tears, and punctures, including a large hole located just forward of the aft pressure bulkhead, where the fuselage skin and internal structure had fractured when forced up and aft (Figure 8).

The flaps and slats were damaged, and the upper surfaces of both wings had punctures resulting from the impact of debris.
1.12.2.2 Electrical power
At the time of the initial impact, the aircraft electrical system was in the normal configuration and the auxiliary power unit was not operating.
Generator 2 stopped supplying power at the time of the second impact; generator 1 stopped supplying power when the no. 1 engine detached from the left wing. The RAT was partially deployed. Scrape marks on the hub and blades were consistent with deployment of the RAT while the fuselage was scraping along the runway.
Both main batteries were in their respective racks in the nose section of the aircraft, with no visible sign of damage.
Also in the nose section of the aircraft, extensive damage was noted on numerous electrical components, including crushed junction boxes and electrical components, electrical contactors broken from their sockets, bent wiring brackets, and severed electrical harnesses.
1.12.2.3 L1 door
No discrepancies were noted on the L1 door or its operating mechanism. In the locked position, the door was retained by the gust lock. When the gust lock release pushbutton was pressed, the door was released and moved freely.
1.12.2.4 Cabin floor
Four areas of the cabin floor were damaged: aft of the cockpit access door (between the forward lavatory and forward galley), forward of passenger seat 31D, forward of passenger seat 33D, and adjacent to the flight attendant's bulkhead-mounted, forward-facing jump seat.
The entire nose landing gear bay had extensive damage that caused the structure to be forced rearward and upward. The floor aft of the cockpit door was forced upward by displacement of a pulley resulting from this structural damage. The cockpit door frame was also buckled as a result of the floor having been pushed upward, thereby restricting the movement of the cockpit door (Figure 9).

Striking the snow-covered ground caused some of the aft lower fuselage stringers and formers to fracture and break, and caused the floor of the bulk cargo compartment to buckle and to be forced upward. The cabin floor was punctured forward of seats 31D and 33D when the stanchions of the forward and aft nets of the bulk cargo door were forced upward (figures 10 and 11).


The cabin floor was also punctured adjacent to the flight attendant's bulkhead-mounted, forward-facing jump seat when the FR65 vertical beam was forced upward (Figure 12).

Neither the net stanchions of the bulk cargo door nor the FR65 vertical beam were deformed.
1.12.2.5 Passenger seats
The examination noted that 7 seatbacks had been displaced forward beyond the upright position and were free to pivot about their hinge point. The seats were located on the right side of the aircraft in rows 3, 21, 24, 25, 28, and 32 (Figure 13).
All 7 seats involved had sheared shear pins. No damage or deformation of the seat frames was observed.
1.12.2.6 Flight crew shoulder-harness assemblies
No discrepancies were noted on the captain's shoulder-harness assembly.
Examination of the FO's right shoulder harness revealed that the inertia reel's plastic flange had fractured, preventing the latch from functioning as designed. The fracture would have prevented the automatic locking feature of the inertia reel from operating correctly. Without the locking feature, the occupant's right side would be unrestrained, even when a sudden acceleration force was applied to the shoulder harness.
The type of failure noted on the flange is consistent with the strap not being extended before carrying out a pull test.
The investigation could not determine when the inertia reel became unserviceable.
1.12.2.7 Coffee brewer
The centre coffee brewer had come free of its mounting rails during the impact sequence.
When the brewer was examined, it was noted that the moveable lever was bent rearward and the face of the lever had scratches consistent with an impact by a hard object. When the lever was pushed, it lodged against the brewer housing. Although the lever appeared to be in the locked position, the upper end of the pin had not engaged the detent, preventing the pin from fully extending into the rail. In this position, the slightest movement of the lever or jolting of the brewer was sufficient to cause the lever to move away from the brewer housing and to allow the spring to release the locking mechanism.
The investigation could not determine when the lever had been bent.
1.12.2.8 Passenger address system
No discrepancies were noted with the PA system during the flight. The loss of electrical and battery power due to the impact damage would have rendered the system inoperable.
1.13 Medical and pathological information
1.13.1 Obstructive sleep apnea
Obstructive sleep apnea (OSA) is a medical disorder characterized by partial or complete obstruction of airflow during sleep. This obstruction causes the individual to awaken for short periods in order to breathe, and leads to an abnormally low concentration of oxygen saturation in the blood, a condition known as hypoxemia. The fragmented sleep and hypoxemia can lead to impaired performance during wakefulness and are associated with increased risk of occupational and motor vehicle accidents.Footnote 35,Footnote 36 People with OSA are at high risk of excessive daytime fatigue and may be unaware of the frequent arousals and awakenings they experience during sleep.Footnote 37 If diagnosed, OSA can be effectively treated. Continuous positive airway pressure (CPAP) therapy is commonly used to treat those who have moderate-to-severe OSA.Footnote 38 However, poor compliance rates (between 30% and 50%) have been noted, resulting in OSA being less effectively treated in non-compliant patients.Footnote 39 The disorder is reliably linked to aeromedically relevant conditions such as hypertension, stroke, coronary artery disease, and diabetes.Footnote 40,Footnote 41
1.13.2 Transport Canada guidance for civil aviation medical examiners on obstructive sleep apnea
CARs Subpart 404 outlines regulations pertaining to flight crew medical requirements, and Subpart 424 contains the medical standards. Both Subpart 404 and Subpart 424 form part of TC's Handbook for Civil Aviation Medical Examiners.Footnote 42 None of these resources provide specific medical guidance to civil aviation medical examiners (CAMEs) regarding OSA. However, TC's mandatory training seminar for CAMEs includes a briefing from a consultant in sleep disorders on detection and management of OSA and other sleep disorders.
1.13.3 Transport Canada management of obstructive sleep apnea
1.13.3.1 General
TC relies on pilots who have been diagnosed with OSA to accurately report symptoms that interfere with their daily lives, such as ongoing daytime sleepiness.
It is the responsibility of the CAME to interview and perform a complete examination of all applicants. The CAME is usually the only person who physically examines the applicant and makes a recommendation for medical certification. TC considers the CAME to be the most important link in the medical certification process.
TC's Handbook for Civil Aviation Medical Examiners stipulates that, during the medical examination, there is a shared responsibility, with the onus on the applicant to report any symptoms and a requirement for the CAME to conduct a careful and thorough examination.
TC's protocol for the assessment of aeromedical risk in applicants who suffer from OSA is that a pilot is expected to report this medical condition and a CAME is expected to identify this medical condition on the Medical Examination Report.
The process to be followed by a regional aviation medical officer (RAMO) in determining whether OSA is managed effectively is not documented. Typically, applicants with OSA are asked to supply a consultation report from their attending physician. The report must include recent sleep studies and a formal assessment of daytime sleepiness, and must also comment on the applicant's tolerance of and response to treatment. However, the method and practice of OSA management is typically left up to the individual CAME and RAMO, and is based on what they know about OSA and what the pilot has reported to them.
Clinically significant OSA that is not adequately treated is not compatible with certification. Applicants with OSA that is adequately treated, such as with CPAP therapy, are deemed fit. Once an applicant is assessed as fit, ongoing surveillance is required; this includes a recent consultation report from the attending physician.
1.13.3.2 Canadian Railway Medical Rules
Subsection 4.9 - Severe Sleep Apnea of the Canadian Railway Medical Rules HandbookFootnote 43 describes a practical process to screen all employees who work in safety-critical positions for OSA and to ensure OSA is subsequently diagnosed and managed appropriately. According to the Guidelines, individuals with severeFootnote 44 OSA cannot be considered fit to work until the treating physician has provided written confirmation and appropriate data indicating that effective treatment has been achieved and that the individual is compliant with therapy.
For individuals prescribed CPAP therapy, adequate compliance is defined by at least two continuous weeks of compliance monitoring that demonstrates average CPAP usage (all days) of at least 5 hours per night. The primary care physician must also provide yearly written confirmation of such compliance monitoring. To carry out this monitoring, the Guidelines note that "CPAP machine data is easily downloadable for this purpose."
1.13.4 Federal Aviation Administration management of obstructive sleep apnea
In March 2015, the FAA issued new medical guidance to aviation medical examiners (AMEs) to address concerns about pilots flying with OSA. AMEs must now conduct OSA screening at the time of the physical examination, using the American Academy of Sleep Medicine guidance provided in the Guide for Aviation Medical Examiners.Footnote 45 Pilots who are at risk of OSA are issued a medical certificate and, shortly thereafter, receive a letter from the FAA's Federal Air Surgeon requesting that an OSA evaluation be completed within 90 days. Pilots who have been diagnosed with OSA according to clinical guidelines,Footnote 46 and who are undergoing treatment, are required to sign a Compliance with Treatment form and to send documentation of effective treatment to the FAA in order for the FAA to consider a special issuance of a medical certificate for the pilot. Documentation of effective CPAP treatment includes a copy of the cumulative annual CPAP machine usage report, which shows actual time that CPAP is used.Footnote 47
1.13.5 Australian Civil Aviation Safety Authority management of obstructive sleep apnea
The Australian Civil Aviation Safety Authority provides designated AMEs with detailed guidelines on the symptoms, contributing factors, and effects of OSA through its Aviation Medicine website. OSA-related guidance describes the approach to medical certification that these examiners are expected to take for pilots diagnosed with OSA, as well as a risk assessment protocol for when and how to investigate for OSA during the certification process. A pilot with OSA is certified as medically fit only when treatment has been demonstrated to be effective through the CPAP machine usage reports and by polysomnography.Footnote 48
1.13.6 United Kingdom's Civil Aviation Authority management of obstructive sleep apnea
The UK's Civil Aviation Authority publishes guidance material that instructs AMEs to immediately declare a pilot who has been diagnosed with OSA as medically unfit. One of the acceptable medical treatments for OSA is CPAP therapy. The organization instructs the pilot that the CPAP machine should be used for at least 5 hours per night and for 6 nights per week. It must also be used during the sleep period just before a flight. CPAP machine usage reports, and any clinical reports, should be assessed by the aviation medical examiner. The CPAP machine usage report should be submitted to the aviation medical examiner together with copies of the pilot's flying logbook for the same period to demonstrate compliance with CPAP therapy.
1.13.7 Air Canada management of obstructive sleep apnea
Section 4.12 of Air Canada's FOM provides basic information on the physiological factors that underlie fatigue and on personal (both preventive and operational) alertness strategies. The FOM includes a paragraph on sleep disorders:
A range of physiological sleep disorders also can disturb the quantity and quality of sleep, and subsequently can degrade waking performance and alertness. Although about one third of adults report a sleep disturbance, this figure is conservative considering that sleepers often are unaware of these disturbances. One example of a common disorder is sleep apnea, characterized by breathing pauses during sleep that cause the sleeper to awaken repeatedly to resume breathing. A cardinal symptom of sleep apnea is snoring (although there are other causes for snoring besides sleep apnea). Sleep apnea is an example of a sleep disorder that is a well-documented health risk and can significantly reduce waking alertness and performance. Evaluation and treatment for sleep disorders are available at accredited sleep disorders clinics.Footnote 49
The fatigue-management training module mentions OSA and recommends that flight crew members consult an aviation medical examiner if a sleep disorder is suspected.
1.13.7.1 Captain
In January 2009, the captain was diagnosed with OSA. The captain did not report experiencing any daytime sleepiness to the sleep specialist consulted at the time. Although the specialist did not recommend that the captain stop flying, the specialist prescribed CPAP therapy to control the OSA. The captain advised Air Canada of the OSA diagnosis and prescription for CPAP therapy. Air Canada subsequently informed the TC RAMO in February 2009. Air Canada advised the captain to continue with his flying duties, and TC approved the captain to continue with flying duties.
At the request of TC, a follow-up sleep evaluation to determine whether the CPAP therapy was an effective treatment for the captain's OSA was conducted in February 2010. The evaluation determined that CPAP therapy was effective at treating the captain's OSA.
In April 2010, the TC RAMO and the consulted sleep specialist reviewed the captain's OSA diagnosis. The specialist reiterated that the captain should continue with his flying duties without any restrictions being placed on his licence. TC subsequently deemed the captain medically fit and no restrictions related to OSA were placed on his licence.
The captain continued to report this medical condition during subsequent medical examinations, and the CAME identified this medical condition on the medical examination report. However, although TC had an ongoing surveillance protocol for OSA, it made no further requests for a consultation report from the captain's attending physician. Because the captain did not report any ongoing difficulties with daytime sleepiness, TC concluded that the OSA was managed effectively and approved the captain to continue with his flying duties.
Between 2010 and 2015, the captain regularly followed up with the sleep specialist. During this period, the captain experienced some difficulties using CPAP therapy and rarely used it.
1.13.8 Fatigue
The test of influence of fatigue is conducted to understand whether the actions of a person are consistent with what is known about human performance in a state of fatigue. The investigation conducted a thorough fatigue analysis that included the captain's OSA, the flight crew's work–rest history, circadian rhythm timing, and the crew's management of the flight and evaluation of their options. Given that the captain rarely used CPAP therapy, he would have been at risk of fatigue related to chronic sleep disruption caused by his OSA. However, there was no indication that fatigue played a causal or contributory role in this occurrence.
1.14 Fire
Not applicable.
1.15 Survival aspects
1.15.1 Occupant injuries
The seating positions of occupants who were evacuated to the hospital with injuries are shown in Figure 13.
1.15.1.1 Crew injuries
The captain had a minor head injury consistent with hitting the glare shield. The FO had a head injury and a serious injury to the right eye, consistent with the FO's upper body twisting to the left before striking the glare shield. The glare shield had corresponding dents from the head impacts.
The flight attendant seated next to the L2 door sustained a shoulder injury as a result of being hit by the coffee brewer. The injury did not prevent the flight attendant from performing assigned duties.
1.15.1.2 Passenger injuries
Most of the passengers' injuries were consistent with their having jackknifed at the lap belt and flailing forward due to longitudinal forces, then striking either the back of the forward seat or another surface, or both. Injuries to hands and wrists were consistent with passengers attempting to hold on to the backs of the forward seats or placing their hands forward as a means of bracing themselves.
The passenger with the infant held the infant with both arms; both the passenger and the infant had injuries consistent with hitting the back of the seat in front.
1.15.2 Child-restraint systems
No child restraint systems were used onboard the aircraft, nor was their use required by regulation.
In 2015, following its investigation into the December 2012 low-energy rejected landing and collision with terrain in Sanikiluaq, Nunavut (TSB Aviation Investigation Report A12Q0216), the TSB found that infants and children who are not properly restrained are at risk of injury and death, and may cause injury or death to other passengers in the event of an accident or turbulence. It further concluded that, if new regulations on the use of child-restraint systems are not implemented, then lap-held infants and young children are exposed to undue risk and are not provided with a level of safety equivalent to that for adult passengers. Therefore, the Board recommended that
The Department of Transport work with industry to develop age- and size-appropriate child restraint systems for infants and young children travelling on commercial aircraft, and mandate their use to provide an equivalent level of safety compared to adults.
Transportation Safety Recommendation A15-02
The TSB assessed TC's latest response to Recommendation A15-02 as follows:
In its response, Transport Canada indicated that it will take a threefold approach to address this recommendation and reduce the risk to which infants and young children are exposed when travelling by air.
In the short term, Transport Canada issued an exemption to increase the range of child restraint systems accepted for use on Canadian aircraft. In the medium term, TC is planning a public awareness campaign in the summer/fall 2016 timeframe on the risks to which children are exposed while travelling on commercial aircraft. In the longer term, during fiscal year 2016/2017, Transport Canada will initiate an in-depth regulatory examination of the issue and outline its plan to consult industry stakeholders.
The Board is encouraged to note that Transport Canada has started taking action, while initiating an in-depth review to address the safety deficiency. However, the Board also notes that ICAO has published guidance to regulators on implementing regulations for child restraint systems. The availability of this material may be useful in accelerating the regulatory examination. Although Transport Canada's proposed actions in the medium and long term may have some benefits, the TSB cannot evaluate if these actions will provide specific solutions that will ensure infants and young children are provided a level of safety comparable to adults.
Therefore, the response to Recommendation A15-02 was assessed as Satisfactory Intent.Footnote 50
1.15.3 Passenger safety and emergency information
The Air Canada safety-features card, located in seatbacks, depicted that passengers were not to take personal belongings in the event of an evacuation, and included a pictogram showing brace positions, including the brace position while holding an infant.
1.15.3.1 Carry-on baggage
In this occurrence, some passengers exited the aircraft with their carry-on baggage, although they were advised not to by the cabin crew during the pre-departure passenger safety briefing and after the aircraft had come to a stop. The safety-features card also depicts that carry-on baggage is not to be taken when evacuating during an emergency.
The TSB has investigated a number of accidents in which passengers retrieved their carry-on baggage during an evacuation. In 2007, following its investigation into the August 2005 overrun occurrence at Toronto Lester B. Pearson International Airport, Ontario,Footnote 51 the TSB found that, during the emergency evacuation of the aircraft, many passengers took their carry-on baggage with them, despite specific instructions to the contrary being repeatedly shouted to them by the flight attendants. In view of the requirement to exit rapidly, especially when an aircraft is on fire, this action presented a significant risk to their safety. The consequences could include impeding an orderly and timely evacuation, damaging an evacuation slide, and increasing the risk of injury.
Research into other accidents involving emergency evacuations revealed that passengers insisting on retrieving their carry-on baggage during an emergency evacuation was not unique to this accident, but was rather widespread. Research has also demonstrated that, in a heightened state of fear, individuals have difficulty understanding and adhering to instructions given. Furthermore, in some aircraft, safety-features cards for the passengers do not provide any direction to leave carry-on baggage behind during an evacuation. Without prior instructions or guidelines concerning the dangers of attempting to take their carry-on baggage during an evacuation, passengers are likely to do so, increasing the potential for injury. The Board believes that any measure that would raise passengers' awareness about the hazards of attempting to take carry-on baggage with them during an emergency evacuation would mitigate the risks. Informing passengers during emergency (safety) briefings of the prohibition against evacuating with carry-on items during an emergency would complement any existing measures to increase the efficiency and effectiveness of an emergency evacuation. Therefore, the Board recommended that
The Department of Transport require that passenger safety briefings include clear direction to leave all carry-on baggage behind during an evacuation.
Transportation Safety Recommendation A07-07
The TSB assessed TC's latest response to Recommendation A07-07 as follows:
TC's latest response indicates that it is persuaded that AC 700-012: Passenger Safety Briefings is having the desired effect. TC does not categorically state that all major carriers have implemented AC 700-012 to provide passengers with the instruction to leave baggage behind in the event of an emergency. Rather, its response indicates that an adequate number of carriers are providing this safety information to their passengers.
TC appears satisfied with these results and the ongoing willingness of operators to voluntarily include this safety information in their passenger briefings. Consequently, it plans no regulatory action that would require operators to provide this information to passengers as stated in Recommendation A07-07. The action taken to date will reduce but not substantially reduce or eliminate the safety deficiency.
The response to Recommendation A07-07 is considered Satisfactory in Part.
No further action is planned by TC, and continued reassessment will not likely yield further results.
The deficiency file is assigned a Dormant status.Footnote 52
In October 2015, the United Kingdom's Civil Aviation Authority issued Safety Notice 2015/006, Management of Cabin Baggage in the Event of an Aircraft Evacuation. The purpose of the notice was to make operators aware of the need to manage passenger behaviour so that passengers do not attempt to take their carry-on baggage with them during an aircraft evacuation. The notice states:
Evidence from evacuations of aeroplanes since 2013 has shown that significant numbers of passengers attempt to take hand baggage with them when evacuating an aircraft. Such passenger behaviour can present a significant hindrance to egress, injury to other passengers and damage to evacuation slides.Footnote 53
The notice also indicated that, in spite of current practices, pre-departure safety briefings that include instructions to leave carry-on baggage behind in the event of an evacuation, and the pictorial information included on the safety-features card, some passengers appear not to assimilate or not to heed such information and remain unaware of its significance to their, and their fellow passengers', overall safety.
1.15.3.2 Brace position
Aircraft occupants can significantly increase their chance of survival and lower their risk of injury by assuming an appropriate brace position, which involves placing the body against the surface it is most likely to strike during impact in order to reduce impact forces and subsequent injuries. Bracing essentially reduces the extent of body movement (flailing) in the event of an impact or sudden deceleration. By leaning on a surface or bending over their legs, passengers are protected from hitting their heads on a hard surface. Thus, the purpose of instructing passengers to assume the brace position is to reduce injuries during impact, increasing the chances of survival.Footnote 54
Air Canada's pre-departure safety briefing did not include an explanation or demonstration of the brace position(s), nor was such an explanation required by regulation. Passengers are instructed to review the safety-features cards, which contain pictograms of brace positions. Air Canada's safety briefings and procedures for passenger safety were consistent with the majority of the CARs 705 operators and met regulatory requirements.
If passengers are provided with specific and unambiguous information, then they will be more likely to behave accordingly in the event of an accident. However, caution must be exercised regarding how much information is provided at one time, since too much at once could negatively affect retention of critical information. Therefore, some information is provided in a briefing before departure, some information is covered in the safety-features card, and additional information is provided when required.
When cabin crews have the opportunity to prepare passengers and the cabin for an emergency, Air Canada's procedures require that they provide passengers with an emergency briefing that includes an explanation of the brace position. Passengers are then required to practise the position, and the cabin crew visually confirm that passengers have adopted the correct position.
Research shows that the word "brace" is poorly associated with passengers' understanding of the correct brace position to adopt in the event of an impact. Directional instructions such as "bend over" and "heads down" are more likely to yield the desired behaviours.Footnote 55
In an emergency in which the cabin crew does not have an opportunity to prepare, such as this occurrence, Air Canada's procedures require the cabin crew to give or shout an oral command to "bend over, keep your head down."
Pre-departure and landing briefings, the safety-features card, and signage aim to convey safety and emergency information to passengers. However, passengers typically pay little attention to the pre-departure briefings and to the safety-features cards.Footnote 56 A study by the U.S. National Transportation Safety Board (NTSB), Survivability of Accidents Involving Part 121 U.S. Air Carrier Operations, 1983 Through 2000, found that 68% of passengers do not read the safety-features cards.Footnote 57 A 2006 study by the Australian Transportation Safety Bureau, Public Attitudes, Perceptions and Behaviours Towards Cabin Safety Communications, found that 65% of passengers do not read the card.Footnote 58
In this occurrence, throughout the impact sequence, some of the passengers adopted a brace position either on their own or in response to hearing the shouted command, "Bend over, keep your head down." Some passengers did not adopt the brace position because they did not hear the shouted command. Others did not know how to properly brace themselves because they had not read the safety-features card.
Because no emergency was expected, the passengers and cabin crew were not in a brace position at the time of the initial impact. Most of the injuries sustained by the passengers were consistent with not adopting a brace position.
1.15.4 Evacuation
During the impact sequence, a number of oxygen masks fell from stowage and a number of overhead stowage bin doors opened uncommanded, allowing carry-on baggage to fall into the cabin. The service director and off-duty Air Canada flight attendants who were in transit shouted to passengers to keep their heads down and to bend forward. Some passengers managed to brace themselves by bending over or holding on to the back of the seat in front of them, or both.
Once the aircraft came to a stop, the cabin crew instructed passengers to leave their carry-on baggage behind. No smoke, mist, or fumes were observed in the cabin. After the L1 door had been opened and the evacuation had started, the door reportedly began to slide back at some time during the evacuation. The flight and cabin crews both completed several checks inside the cabin to ensure that no passengers remained before exiting the aircraft themselves.
1.15.5 Planned or prepared emergency landing
In a planned or prepared emergency landing, the cabin crew prepares the passengers by providing a briefing. The briefing includes, in part, the following information:
Just before landing, you will hear the command "Brace for Landing". When you hear this command, brace immediately and stay braced until we stop completely.
There are two ways to brace. The first way is to bend forward and place your hands and arms against the chairback in front of you. Press your head against your forearms.
The second way is to bend forward, wrap your arms under or behind your legs or grasp your ankles. Press your face into your lap.
Practice the brace position most comfortable for you now.
Just after landing when you prepare to evacuate, you must leave all your personal belongings behind, including purses and briefcases. Cabin baggage will slow the evacuation and can damage the slides.
Review the procedures we have just explained.Footnote 59
During the brace-position portion of the briefing, the flight attendants demonstrate the first brace position. They also verify that the passengers practise adopting the correct position.
1.15.6 Minimum number of flight attendants
From 22 August 2014, a TC-approved exemption was in place for CARs 705.104; this exemption authorized Air Canada to operate its Airbus 319, 320, and 321 and Embraer 190 fleets with at least 1 flight attendant for each unit of 50 passenger seats (a 1:50 ratio) that is installed on the same deck of the aeroplane.Footnote 60
This exemption required the airline to include, during initial training and the ART, drills of methods to open both exits and to manage passenger flow at more than 1 exit if a flight attendant is responsible for opening more than 1 exit. This dual-exit drill includes steps to systematically open both doors. As part of their responsibilities, flight attendants need to continuously monitor the evacuation flow.
The dual-exit drill was imposed to close a gap that TC had identified in the existing training and also to address NTSB recommendation A-92-071. The NTSB had recommended that the FAA require flight attendant training to include drills on methods to open exits and manage flow at more than 1 exit if procedures require a flight attendant to be responsible for opening more than 1 exit. Before this drill was implemented, cabin crews were trained that they could leave their door/exit and open the opposite door/exit when the evacuation flow was too slow.
Although Transport Canada required the dual-exit drill to be implemented in the training, it did not require all cabin crew to receive the training before an organization implemented the 1:50 ratio.
Air Canada began operating with the 1:50 ratio before incorporating the dual-exit drill into its ART as of April 2015. At the time of the accident, neither the service director nor the flight attendants had received the dual-exit drill training, nor were they aware of the requirement for such training in order for Air Canada to operate with the exemption allowing 1 flight attendant for each unit of 50 passengers.
In June 2015, CARs 705.104 was superseded by CARs 705.201, Minimum Number of Flight Attendants, to allow CARs Subpart 705 operators to operate with a ratio of 1 flight attendant per 50 configured passenger seats. The conditions requiring the dual-exit drill and demonstration of an evacuation are included in the amended regulations. The European Union and the U.S. operate with the 1:50 ratio.
1.15.7 Transport Canada: What to wear on the plane
TC's web page What to wear on the planeFootnote 61 provides information to passengers on what to wear for safe travel, particularly when they may have to go outdoors during a typical Canadian winter. What to wear on the plane notes that, in the unlikely event that the aircraft is evacuated, passengers should avoid wearing shorts or skirts when travelling. It also notes the need to keep footwear on during the flight because, in an emergency, finding shoes will not be a priority. Lack of footwear can create problems for passengers, particularly if they try to walk through jet fuel (which may be on fire), broken glass, or sharp metal fragments without shoes to protect their feet. If passengers do not dress appropriately for safe travel, they risk being unprepared for adverse weather conditions during an emergency evacuation.
1.16 Tests and research
1.16.1 TSB laboratory reports
The TSB completed the following laboratory reports in support of this investigation:
- LP061/2015 - DFDR [digital flight data recorder] Download and Analysis
- LP071/2015 - NVM [non-volatile memory] Recovery - EGPWS [enhanced ground proximity warning system]
- LP072/2015 - NVM Recovery - CPAP
- LP073/2015 - Site Survey Report
- LP076/2015 - Coffee Maker Restraint Examination
- LP086/2015 - Shoulder Harness Assembly Examination
- LP094/2015 - Photo Collection
- LP110/2015 - Analysis of Material Transfer
1.17 Organizational and management information
1.17.1 Air Canada
1.17.1.1 General
Air Canada operates under the requirements of CARs Subparts 705 and 573. It is the holder of an air operator certificate and is an approved maintenance organization. The company also holds Part 145 approval from EASA by complying with the Agreement on Civil Aviation Safety Between Canada and the European Community.
The company provides domestic flight services as well as both scheduled and non-scheduled international flight services from Canada and abroad. Air Canada's fleet consists of approximately 200 aircraft of various types, including Boeing 787, 777, and 767; Airbus A330, A321, A320, and A319; and Embraer E190.
Air Canada is Canada's largest air operator, with approximately 27 000 employees, including approximately 2000 maintenance personnel, various technical experts employed to support the operation, 6650 cabin safety personnel, and 3200 pilots.
The following Air Canada documents are available to flight crew:
- The TC-approved Aircraft Operating Manual (AOM),Footnote 62 which contains the SOPs, is based on information about the operational, technical, procedural, and performance characteristics of the aircraft in the Air Canada Flight Crew Operating Manual (FCOM).Footnote 63 Flight crews use the AOM for all aircraft operations.
- The FOM contains information that applies to all flight operations, except when superseded by an AOM.
- The Flight Crew Training Manual (FCTM) is designed as a reference document to provide pilots with practical information on how to operate the Airbus aircraft.
Air Canada has a TC-approved safety-management system (SMS) and has incorporated the SMS into its existing manuals.
1.17.1.1.1 Cabin crew training
The cabin crew ART verifies competency in safety, security, and emergency procedures for all aircraft types in Air Canada's fleet. Crew resource management training is also provided to foster effective communication, cooperation, and coordination.
Any cabin crew member can initiate an evacuation in a life-threatening or a catastrophic event.Footnote 64 In an emergency evacuation, the primary objective is to evacuate passengers and crew in the safest and most rapid manner.Footnote 65 To minimize evacuation time, all serviceable and unobstructed exits must be used to maintain a balanced flow of evacuating passengers.
The ART is scenario-based and, since not all possible scenarios could be covered, cabin crews are trained to assess, adapt, and act on the particular situation. The Air Canada cabin crew training does not include a scenario in which passengers initiate an over-wing evacuation, nor does it cover assessment of the risks involved in deployment of the rear slides when there are passengers outside of the aircraft. Therefore, to effectively deal with these 2 situations, a cabin crew would need to adapt their actions so that they respond appropriately to the hazards they face.
In this occurrence, the L1 door was serviceable and unobstructed, there was no fire or other life-threatening hazard, and passengers were exiting through the over-wing exits. The service director assessed the evacuation flow as good and determined that there was therefore no need to open the R1 door.
The flight attendants stationed in the rear of the aircraft noted no life-threatening hazards. Because no evacuation order had been given, and deplaned passengers and firefighters were observed walking near the rear of the aircraft in an area where the deployment of the rear slides may have created additional hazards or risks, the flight attendants determined that there was no requirement to open the L2 and R2 doors.
The flight attendant training standards recognize that the PA and interphone are tools for relaying safety information and, if used correctly and effectively, these tools increase the probability that a message will be received and understood. At Air Canada, flight crew are to initiate an evacuation by calling "Evacuate! Evacuate!" over the PA system. However, if the PA system is inoperative, the flight crew can use the interphone or give verbal instructions to the service director.
In this occurrence, the flight crew had suffered head injuries and were disoriented when the aircraft came to rest. Therefore, they did not immediately communicate with the service director. When the flight crew regained their awareness, the PF attempted to contact the service director; however, the PA and interphone systems were not operational. At this time, the evacuation was already under way.
1.17.1.1.2 Flight crew training
Flight crew training at Air Canada is carried out under the advanced qualification program (AQP). TC defines the AQP as
A voluntary program and alternative method of training, evaluating and qualifying flight crewmembers, instructors and evaluators, that uses a systematic methodology for developing proficiency-based training and evaluation programs in lieu of traditional training programs.Footnote 66
Instead of traditional pilot proficiency checks, the AQP involves specific validation sessions that provide scenario-based training, allowing for a more realistic training experience that more closely resembles line flying. The AQP focuses heavily on crew resource management, including threat-and-error management, in which potential hazards are analyzed and appropriate steps are taken to avoid, trap, or mitigate threats and errors before they lead to an undesired aircraft state.
To follow the AQP program requirements, Air Canada works on a continuing qualification cycle of 32 months. The pilots perform training in the simulator every 8 months, with evaluation every 16 months. Under the AQP, pilots are to carry out training on LOC approaches once every 32 months. The captain had completed LOC training in February 2014, and the FO had completed LOC training in November 2013.
1.17.1.2 Stable approach
According to TC, an approach is considered stable if it meets the air operator's criteria for such an approach.
The most recent FOM at the time of the occurrence explained Air Canada's stable approach policy as follows:
Air Canada's Stable Approach Policy is built around an Arrival Gate concept whereby a flight shall not continue the approach unless the required criteria for each Arrival Gate are met. There are two Arrival Gates for every approach; the first is the FAF (or FAF equivalent), the second Arrival Gate is at 500 feet AGL (or 100' above minimums, whichever is higher). A Go-around is mandatory if the criteria for each Arrival Gate is not met.
For non-precision approach, at the first Arrival Gate (FAF), the aircraft must be on the inbound course and on the descent profile defined by the FPA, the vertical speed, or the flight management guidance system.
No flight shall continue an approach past the FAF Arrival Gate unless it is being flown in a way that ensures the Stable Approach Criteria will be met by the 500 foot Arrival Gate.Footnote 67
At the second gate (500 feet AGL or 100 feet above the MDA), no flight shall continue unless the following stable approach criteria are metFootnote 68:
- Flaps and landing gear are in the landing configuration; and
- Landing Checklist completed; and
- Indicated airspeed with plus 10 knots to −5 knots of target airspeed (Airbus-target airspeed is Ground Speed Mini when active); and
- Thrust stabilized, usually above idle, to maintain the target approach speed along the desired flight path; and
- Established on the correct vertical approach path and where applicable, remaining within ½ scale deflection of the guidance used for an instrument approach or, for a visual approach, established on the correct approach slope as indicated by visual approach slope indicators (i.e. VASIS [visual approach slope indicator system], PAPI or HGS [head-up guidance system]); and
- Rate of descent not in excess of 1000 fpm unless required to maintain the published constant descent path (e.g. glideslope, VASIS, calculated descent rates, etc.). If an approach requires a rate of descent greater than 1000 fpm, a special briefing should be conducted; and
- Established on the correct lateral approach path and where applicable, remaining within ½ scale deflection of course deviation indications for VOR [very high-frequency omnidirectional range], localizer approaches and five degrees of track for NDB [non-directional beacon] approaches.Footnote 69
Air Canada considers an aircraft to be on the correct vertical approach path when the flight crew has selected the correct FPA, in accordance with the SOPs. Given that the above criteria were met, AC624 was considered to be on a stable approach.
1.17.1.3 Approach procedures
The AOM and FCTM outline non-precision approaches and provide guidance on how to perform them. A coupled–selected approach is required for a LOC approach. When conducting a LOC approach, the lateral guidance is coupled to a LOC (autopilot directed by ground-based aids), and the vertical guidance is selected by the crew (autopilot directed by pilot-selected commands).
The methods to fly a coupled–selected approach are as follows:
- AP [autopilot] should be engaged in LOC/FPA modes
- Use FD [flight director] referenced to the Flight Path Vector
- Select appropriate raw data on ND [navigation display] for monitoring tracking and descent
- Use A/THR [autothrust]
- Use managed speedFootnote 70
When determining the flight path angle for the vertical guidance, pilots use the vertical descent angle (VDA) that is published on the applicable Jeppesen chart. The VDA defines the flight profile in which the aircraft will cross the runway threshold about 50 feet AGL.
On a non-precision approach, once the flight crew has established visual contact with the runway environment and the autopilot has been disconnected, the PF manually flies the aircraft using visual cues to determine its lateral and vertical position relative to the runway. Air Canada training and pilot experience both reinforced the knowledge that there may be a need to make minor corrections to the flight path to ensure the aircraft maintains a stable approach and crosses the threshold at the correct height to ensure landing in the touchdown zone.
According to the FCTM, for a coupled–selected approach, the FPA should be preset on the flight control unit. A smooth interception of the final approach path can be achieved by pulling the FPA selector knob when the aircraft is 0.3 nm before the FAF. The requirement to preset the FPA before pulling the selector knob is not specified in the AOM's SOPs.
During a non-precision approach, when the aircraft reaches the MDA, a PM is required to make a call of "Minimums" followed by either "No contact," "Lights only,"Footnote 71 or "Runway in sight." The response by a PF is to call either "Go-around, flaps" or "Landing." Air Canada does not provide any specific training on or definition of what "Lights only" entails.
When a PM calls, "Lights only," a PF expects that the PM has acquired visual references in order to continue with the approach. The typical response is for the PF to call, "Landing," and to continue with the approach.
In accordance with the AOM section 1.01.22, Autoflight limitations, at the MDA, when the required visual conditions are met to continue the approach, the autopilot must be disconnected.
During the occurrence flight, the autopilot was not disconnected until the aircraft reached 484 feet ASL, about 23 seconds after passing the calculated MDA of 813 ASL, which did not conform with an aircraft flight manual limitation, CARs 602.07(a), or Air Canada's SOPs.
1.17.1.4 Approach monitoring guidance
The Air Canada FCTM indicates that the flight crew should monitor the aircraft's position along the vertical flight path while conducting a non-precision approach, by referring to the distance indicated on the distance measuring equipment, the altimeter reading, and the time.
The SOPs state that the appropriate raw data on the navigational displayFootnote 72 should be selected for monitoring the tracking and the descent. As well, the flight crew should use the bird in the PFD as the flying reference.
The FCTM states, in a supplementary information flying reference,
even if the bird indicates that the aircraft is flying the correct flight path angle and track, this does not necessarily mean that the aircraft is on the correct final path.Footnote 73
Although the Air Canada FCOM identifies the requirement to monitor and adjust the position and flight path, pilots do not have access to this document as a reference. Pilots refer to Air Canada's SOPs; however, these do not provide direction on monitoring the vertical flight path when the FPA guidance mode is engaged, nor is such monitoring taught in training (Table 4).
| Air Canada SOPs | Air Canada FCOM* |
|---|---|
| At 0.3 NAUTICAL MILES prior to FAF, or descent point if other than FAF, if vertical guidance selected FPA................................PF..............SET Do not use the Vertical Deviation on the PFD. Set charted FPA to follow the published descent profile, taking into account the minimum altitudes. Use radio navaid raw data to monitor the lateral navigation during a conventional NPA. Note: For RNAV (GPS) approaches the descent point may differ from the FAF (prior or after the FAF). Approach charts provide the appropriate descent location, altitude and flight path angle. |
At 0.3 nm from the Final Descent Point: FPA selector.................................................PULL FPA MODE...............................CHECK ENGAGED ‐ Check NAV FPA, TRK FPA or LOC FPA is engaged. POSITION/FLIGHT PATH....MONITOR/ADJUST GO AROUND ALTITUDE................................... SET ‐ Set when below the go around altitude to avoid unexpected altitude capture. FLIGHT PARAMETERS.............................MONITOR ‐ Crosscheck distances versus altitudes as published on the charts. ‐ If approaching on a conventional radio NAVAID procedure, monitor the lateral and vertical guidance using raw data. |
* The information in the Air Canada FCOM table is identical to that in the Airbus FCOM
In accordance with CARs 705.09 and TC's Air Carrier Inspector Manual,Footnote 74 TC reviewed and approved both Air Canada's AOM and SOPs. During this process, TC did not identify the discrepancy between the Air Canada documents and the Airbus documents.
In early 2014, NAV CANADA and Jeppesen introduced a distance/altitude table on selected charts (Figure 14). According to the Canada Air Pilot general pages (CAP GEN), this table "lists a series of distances from a specified location and the appropriate altitude that equates to the constant descent angle at that distance."Footnote 75
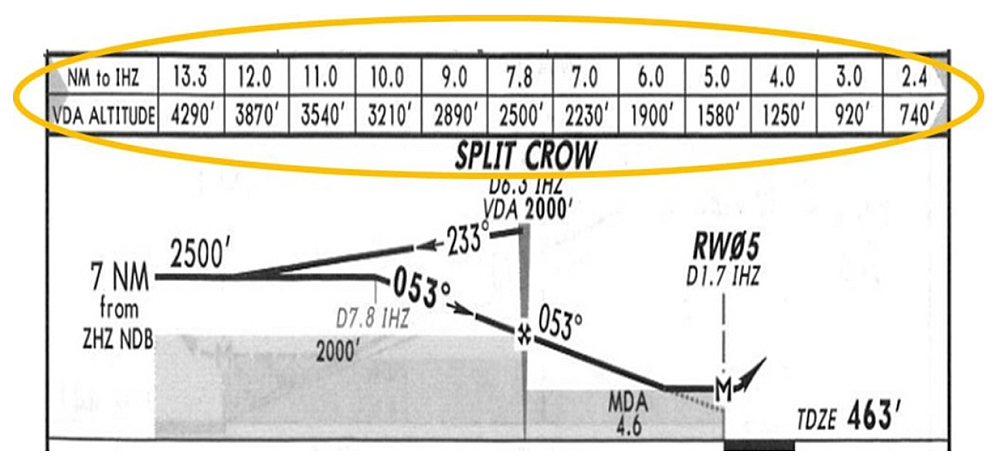
At Air Canada, the use of the distance/altitude table on the Jeppesen chart as a monitoring tool is not cited during pilot training for LOC/non-precision approaches.
1.17.1.5 Transport Canada oversight
TC expects companies to proactively manage the safety of their operations so that risks are managed to acceptable levels, and to have programs in place to ensure continued compliance with all regulatory requirements. TC's surveillance program is designed to evaluate whether an aviation company has implemented appropriate and effective systems; specific systems-based surveillance inspections are conducted at intervals that are based on risk indicators. The program is targeted toward key systems that are determined by certificate type and by whether the company is required to have an SMS. The surveillance program is based on a systemic approach to managing risk, and in principle, may focus on any process required by regulation.
The TSB reviewed the surveillance activities carried out by TC and the company's responses during the 2 years leading up to the occurrence.
In September/October 2013, TC had carried out an assessment of Air Canada, which included all components of SMS and EASA Supplement requirements. The assessment had concluded that Air Canada had the capability to maintain compliance with the CARs. The assessment report had identified 12 findings, described as minorFootnote 76 to moderateFootnote 77 and related to the SMS, including missing AQP training summary sheets for initial training of several newly hired pilots. All of the findings were addressed in the company's corrective action plan, which TC accepted in December 2014.
In 2014 and 2015, TC carried out 4 process inspections on Air Canada's flight operations department, as well as numerous other surveillance activities, such as monitoring the company's AQP, pilot training, and approved-check-pilot program. No majorFootnote 78 findings were noted.
1.18 Additional information
1.18.1 Stabilized constant descent angle approach
A non-precision approach is an approach that uses lateral guidance but no vertical guidance. Therefore, before the MDA, flight crews may need to make minor flight path adjustments to correct for any vertical deviations from the intended descent profile. Transport Canada notes that
The need for a stabilized final approach during non-precision approaches (NPAs) has been recognized by the ICAO CFIT [controlled flight into terrain] Task Force as an aid to prevent CFIT accidents.Footnote 79
The stabilized constant descent angle (SCDA) technique involves intercepting and maintaining a constant angular descent profile from the FAF to a reference datum above the runway threshold (typically 50 feet). The descent is therefore flown at a constant angle and a constant rate of descent, requiring no configuration change. When using the SCDA technique, upon reaching the MDA, the flight crew decides either to continue on the constant angle to land if the required visual references are in sight, or to execute a missed approach if visual conditions are not imminent.
The SCDA technique requires no specific aircraft equipment other than that specified by the title of the non-precision approach procedure. Pilots can fly suitable non-precision approaches with a SCDA using basic piloting techniques. The benefits of the SCDA technique have been demonstrated and validated by TC and several international organizations.
According to Transport Canada Aeronautical Information Manual (TC AIM), the "SCDA is considered a form of ICAO's continuous descent final approach (CDFA). In the interest of respecting terminology already in use in the Canadian civil aviation industry and standardization with NAV CANADA charting, the [SCDA] terminology has been adopted."Footnote 80
In July 2014, NAV CANADA published approach charts that include constant descent angleFootnote 81 information in a tabular form and in the profile view. NAV CANADA determined the constant descent angle and procedure altitudes using normal trigonometric functions, without accounting for the curve of the earth. A 50-foot threshold crossing height and the threshold elevation are normally used when making these calculations.
1.18.2 Flight path angle guidance mode
The Airbus FPA guidance mode is a selected vertical mode that guides the aircraft to fly an FPA target and that can be used for approach. The FPA is the angle between horizontal and the total velocity vector of the aircraft. Therefore, the FPA guidance mode does not provide fixed vertical guidance with any reference to a ground-based aid, such as glideslope or ILS approach.
When flying with the FPA guidance mode, external perturbations, such as wind variations or turbulence, can cause the aircraft to move away from the selected FPA initial approach path. If these perturbations result in momentary changes to the aircraft's vertical trajectory,Footnote 82 then the autopilot will recover the selected FPA, effectively paralleling the initial trajectory (Figure 15).

If the perturbations cause the aircraft to move below the initial approach path, then once the autopilot captures the selected FPA, the aircraft will continue to descend, but on a flight path that is below and parallel to the initial approach path. If these perturbations continue throughout the descent and the flight crew makes no adjustments to recover the initial approach path, then the altitude discrepancy between the initial and actual flight paths will continue to increase, resulting in the aircraft flying below the published approach vertical profile. This actual flight path will result in a low indication on the airport's approach slope indicators. A go-around must be initiated unless the flight crew estimates that only small corrections are necessary to rectify minor deviations from stabilized conditions.
The Airbus FCOM does not offer guidance on how to make adjustments to the FPA; for example, it does not indicate how large the adjustment should be or for how long the adjustment should be made in order to return an aircraft to the selected flight path. For a flight in FPA guidance mode, Air Canada's practice was that, once the aircraft was past the FAF, the flight crews were not required to monitor the aircraft's altitude and distance from the threshold, nor to make any adjustments to the FPA.
According to Airbus SOPs, the FPA guidance mode should be selected (by selecting TRK/FPA or "bird" with the HDG V/S-TRK FPA pushbutton) and the descent angle set before 0.3 nm from the final descent point. At 0.3 nm from the final descent point, the flight crew should pull the VS/FPA knob to begin the descent.
Air Canada's practice was that, once the aircraft was in level flight before the FAF, the pilot pulled the V/S-FPA knob and selected the angle to 0.0, then flew the aircraft in that mode. At 0.3 nm from the FAF, the pilot then selected the appropriate angle for descent.Footnote 83
1.18.3 Cold temperature correction
Pressure altimeters are calibrated to indicate true altitude under international standard atmosphere (ISA)Footnote 84 conditions (referred to as a standard day). Any deviation from a standard day results in an erroneous reading on the altimeter. If the temperature is lower than ISA, the true altitude will be lower than the indicated altitude. Although there is no regulatory requirement to do so, temperature corrections for cold weather should be added to the published altitudes on instrument approach charts to ensure obstacle clearance, since the altimeter displays will read incorrectly in these temperatures.
The parameters computed by the Airbus air data inertial reference unit are barometric and ISA-referenced. When the atmosphere differs from ISA conditions, the altitude and FPA computed by the air data inertial reference unit, and the associated indications on the PFDs (altitude, vertical deviation, etc.), are inaccurate. Therefore, an aircraft conducting a non-precision approach must be operated at an indicated altitude that is corrected to compensate for the effect of cold temperature, and the FPA, which is the published vertical descent angle, must be adjusted to compensate for the temperature-corrected indicated altitude.
In 2009, while working with Air Canada, TC identified a discrepancy involving all Airbus A320, A330, and A340 series aircraft when a non-precision approach was carried out in cold temperatures. When the cold temperature corrections were applied to the FAF altitude and the aircraft was flown with the FPA selected to the published vertical descent angle, the aircraft's position did not accurately correspond to the published distances and altitude. Since the Airbus FCOM did not include any applicable procedures, TC required Air Canada to work with Airbus to develop a procedure so that, when a cold temperature correction is applied to a FAF altitude, the FPA can be adjusted to compensate for the corrected altitude.
In April 2010, Airbus published a Temporary Revision to the FCOM Standard Operating Procedures, Non-Precision Approaches.Footnote 85 Although this revision, which introduced an FPA correction chart for cold weather operation, provided additional guidance, it did not take into account Air Canada's procedure for rounding up the correction altitudes. Therefore, Air Canada decided to develop its own procedures for adjusting the FPA when cold temperature corrections had been applied to the FAF altitude. This method was accepted by TC, and, in early 2011, Air Canada's Airbus A320 Quick Reference Handbook was revised to include the FPA and chart of approach altitude corrections for cold temperatures.Footnote 86 The chart was designed to identify the applicable altitude correction (in 100-foot increments) to be added to the FAF and the degree correction to be added to the FPA based on the approach altitude height above the aerodrome and the temperature in degrees Celsius. The Quick Reference Handbook also includes a chart for the cold temperature corrections for the MDA. The investigation determined that the FPA calculated by the flight crew was in accordance with the Quick Reference Handbook.
1.18.4 Required visual references
Section 100.01(1) of the CARs defines required visual reference as follows:
In respect of an aircraft on an approach to a runway, means that portion of the approach area of the runway or those visual aids that, when viewed by the pilot of the aircraft, enable the pilot to make an assessment of the aircraft position and rate of change of position, in order to continue the approach and complete a landing.Footnote 87
This information is also found in the TC AIM (section GEN 5.1), and in the CAP GEN.
The TC AIM, the CAP GEN, and the Air Canada FOM all list the following 10 items, of which pilots should see at least 1 in order to continue an approach to a safe landing and to meet the requirements for required visual reference:
- the runway or runway markings;
- the runway threshold or threshold markings;
- the touchdown zone or touchdown zone markings;
- the approach lights;
- the approach slope indicator system;
- the runway identification lights;
- the threshold and runway end lights;
- the touchdown zone light;
- the parallel runway edge lights; or
- the runway centre line lights.
The Air Canada FOM did not identify that the required visual reference should enable the pilot to assess aircraft position and rate of change of position in order to continue the approach to a landing.
1.18.5 Visual cues
Visual illusions result from an absence of, or an alteration in, visual references, which modifies a pilot's perception of his/her position relative to the runway threshold. Visual illusions affect perception of heights, distances, and/or intercept angles.Footnote 88
During the visual segment of an approach at night, the visual cues that may be used to assess aircraft vertical position and its rate of change relative to the runway environment include the following:
- position of the runway environment lights in the aircraft windscreen and the rate/direction of any change in the position of the runway lights;Footnote 89
- aspect ratio of the runway edge lights to the runway end/threshold lights;Footnote 90
- linear perspective (degree of convergence) of the parallel lines of runway edge lights;Footnote 91 and
- amount of space the pilot sees between the individual runway edge lights.Footnote 92
Visual approach aids (such as PAPI lights) can be used to supplement these cues. In this occurrence, the flight crew did not see the PAPI lights during the approach.
As an aircraft moves beyond the MDA, it is expected that visual cues associated with the runway environment will become increasingly visible to the flight crew and will assist with assessment of the aircraft position and rate of change of position in relation to the runway.
Approaching a runway that has even a small uphill slope can create an illusion that the aircraft is too high. When visibility is poor, runway environment visual cues become visible to the flight crew later in the approach sequence than they would under good viewing conditions. When these visual cues are eventually acquired, there is less time available to recognize and identify them as well as to understand their configuration in order to effectively judge aircraft position and movement relative to the runway.
1.18.6 Effect of falling snow
The movement of snowflakes at night against a black background provides strong signals to a pilot's peripheral vision that are difficult for the visual system to ignore. Depending on the density of the snowflakes and the level of forward lighting from the aircraft, the light back-scattered by snowflakes makes it more difficult for a pilot to detect and discriminate among lights in the visual environment than if there were no snow. Because of this, landing lights and strobe lights are typically not used when flying through snow, cloud, fog, or haze.
1.18.7 Cultural lighting on approach to Runway 05
At the time of the occurrence, the approach to Runway 05 had few sources of cultural lighting. The most notable source was a facility located directly under the flight path, about 4000 feet from the threshold. The facility's overhead yard lights illuminated an area about 500 feet by 225 feet.
1.18.8 Information processing
Pilots operate in a complex environment in which there are multiple sources and types of information to monitor. When pilots receive information about the environment that fulfils their expectations, they tend to react quickly and in an error-free manner. However, when they receive information that is contrary to their expectations, their reactions will be slower and may be inappropriate.Footnote 93 A number of biases, including the following, are known to have an impact on how information is interpreted and attended to in complex environments:
- Expectation bias describes the fact that, when people expect one situation, they are less likely to notice cues indicating that the situation is not quite what it seems. Expectation bias is worsened when people are required to integrate new information that arrives piecemeal over time in incomplete, sometimes ambiguous, fragments.Footnote 94
- Plan continuation, a form of confirmation bias, is a "deep-rooted tendency of individuals to continue their original plan of action even when changing circumstances require a new plan."Footnote 95 Once a plan is made and committed to, it becomes more difficult for stimuli or conditions in the environment to be recognized as indicating change than if a plan had not been made. For a pilot to recognize and act on a reason to change the plan in a timely manner, a condition or stimulus needs to be perceived as sufficiently salient to require immediate action.
1.18.9 Cockpit automation
Automation incorporated into aviation has become one of the prime resources for critical decision making. A pilot's trust in an automated system develops with repeated exposure. The extent that an individual allows an automated system to perform and manage functions that he or she could also perform manually depends on the amount of trust he or she feels towards it. Further, the more trust operators have in an automated system, the less often they will monitor it.Footnote 96 Aircraft pilots' trust in on-board automated systems thus determines whether they will rely on, or override, a system.Footnote 97
Autopilot systems reduce pilot operational workload by freeing the PF from routine handling tasks, allowing more time and resources to assess the overall operational situation. Air Canada's AOM states:
as a matter of routine the automation should be engaged as soon as possible after take-off and, circumstances permitting, remain engaged to a late stage on the approach.Footnote 98
The A320's autopilot system can be used during most phases of flight, including an autoland, a system that fully automates the landing procedure of an aircraft's flight, with the flight crew supervising the process. Autoland is capable of putting the aircraft in the touchdown zone on an ILS/precision approach without control input from the flight crew.
The PF had carried out an autoland on Runway 23 at CYHZ 2 nights before the accident. In this occurrence, the aircraft was conducting a non-precision approach, for which autoland was not possible.
1.18.10 Reported visibility
Reported ground visibility may not be representative of flight visibility, which can change as aircraft descend from altitude. It is not uncommon for visibility ratings to show large fluctuations during periods of low visibility.Footnote 99
RVR readings indicate "the maximum horizontal distance […], measured by an automated visual landing distance system […], at which the runway, or the lights or markers delineating it, can be seen from a point above its centreline at a height corresponding to the average eye level of pilots at touchdown."Footnote 100
As previously indicated, Runway 05 is not equipped with an RVR system. RVR readings for Runway 23 were not provided to the flight crew, and therefore they would not have been aware of the following information. In the 15 minutes leading up to the accident, the RVR readings for the midpoint of Runway 23 (RVR B) fluctuated between 1600 and 4000 feet. In the period from when the aircraft crossed the MDA to when the autopilot was disconnected, the RVR B readings fluctuated between 3500 and 4000 feet. These RVR values demonstrate how quickly visibility can fluctuate during periods of low visibility.
1.18.11 Operation specification – visibility limitations
An approach ban prohibits flight crew of aeroplanes operating in a commercial air service from continuing an approach past the FAF if the visibility is reported as below the limiting value during the approach.
In Canada, before 2006, the approach ban was imposed, with certain exceptions, only when RVR sensor equipment recorded values for the approach below category II minimums (that is, aeroplane RVR A 1200 feet/RVR B 600 feet).
Following several low-visibility accidents in the late 1990s, the TSB issued Recommendation A02-01 to TC to expedite the approach-ban regulations prohibiting pilots from conducting approaches in visibility conditions that are not adequate. In 2006, TC introduced new regulationsFootnote 101 for low-weather instrument approaches.
These regulations mainly affect commercial operators. A generic approach ban was introduced for commercial operators for all instrument approaches (category I precision, approach procedures with vertical guidance, and non-precision approaches) at a visibility value that is a function of the published Canada Air Pilot visibility for the approach procedure flown. This generic ban takes effect when the RVR, runway visibility, or ground visibility is reported to be below the RVR or visibility value corresponding to approximately 75% of the Canada Air Pilot published visibility specified for the procedure flown. This approach ban does not conform to internationally accepted safety regulations established by ICAO and civil aviation authorities around the world (such as FAA and EASA), which specify that, in order to conduct an instrument approach procedure, the actual visibility must be no less than the visibility specified on the approach.Footnote 102
Operators under CARs Subparts 703, 704, and 705 may be permitted to conduct instrument approaches at 50% of published visibility values if they meet specified conditions and are authorized by an OPS Spec. Air Canada had the specified OPS Spec. According to its Quick Reference Handbook, LOC approaches inside Canada were authorized in the following conditions:
- Autopilot and flight director are used to the minimum descent altitude.
- For reported visibility below ½ sm (2600 feet), the aircraft is captain-flown.
- For visibility below RVR ¾ sm (4000 feet), there is approach lighting (of any type) and low-, medium- or high-intensity runway lighting.
- Crosswinds are within AOM limits.
- Approach is straight-in.
The published visibility for the CYHZ LOC approach on Runway 05 is 1 sm. Therefore, in accordance with Air Canada's OPS Spec, the flight crew could carry out an approach with reported visibility of ½ sm.
Since 2006, when the generic approach ban and the OPS Spec came into effect, the TSB has not carried out an investigation in which the approach ban or OPS Spec were identified as causal or contributing factors in an occurrence.
1.18.11.1 Approach differences
When determining the published visibility, both the EASA and the FAA rules for approach minimums take into account the type of approach lighting system (ALS) installed on the runway.Footnote 103 The visibility published on the approach charts is the minimum visibility required to carry out an approach.
In the U.S., carrying out an approach onto a runway that is equipped with an ODALS, which is considered a basic ALS, requires a minimum visibility of ¾ sm (RVR 4000 feet).Footnote 104 To conduct an approach with a reported visibility of ½ sm (RVR 2400 feet), a runway would have to be equipped with an ALS that consists of high- or medium-intensity and/or flashing lights greater than 2400 feet in length.
In Canada, for a non-precision approach, the minimum visibility to carry out an approach under the OPS Spec does not take into account the type of ALS installed on the runway (Appendix D).
According to TC's TP308, Criteria for the Development of Instrument Procedures, for any non-precision LOC approach in Canada, the minimum altitude is 250 feet AGL, and the minimum published visibility is 1 sm (RVR 5000 feet).Footnote 105
On a standard 3° descent, an aircraft would reach 250 feet AGL about 3800 feet from the threshold. If the runway were equipped with an ODALS, then the aircraft would be about 2300 feet from the first light of the ODALS.
For the published LOC Runway 05 approach at CYHZ, an aircraft would reach the published MDA (277 feet AGL) about 4200 feet from the threshold, or about 2700 feet from the first light of the ODALS.
1.18.12 Runway 05 landing system
Halifax International Airport Authority (HIAA) has not received a request to perform a risk assessment from its stakeholders (NAV CANADA, air carriers, and pilots), nor has it received any information indicating that the safety of the runway is compromised with the type of landing system currently installed. Performing a risk assessment of the types of landing systems installed on runways is the responsibility of NAV CANADA, as it is the owner and operator of these systems.
In 1998, NAV CANADA conducted a feasibility analysis for the installation of an ILS on Runway 05 at CYHZ. The results indicated high installation costs for both localizer and glidepath equipment, with very little improvement in airport accessibility (less than 0.75%). In January 1999, the analysis results were presented at the Air Navigation System National Advisory Committee (ANSNAC), which stated that an ILS would be installed on a cost-recovery basis. However, no further action was taken because there was no agreement from customers to proceed on a cost-recovery basis.
NAV CANADA has indicated that risk is managed to an acceptable level for any approach type based on criteria such as
- the design, installation, and maintenance of all underlying navigation systems;
- the use of approved criteria in the design and maintenance of the procedures; and
- the associated aircraft and crew systems authorized to use the approach.
According to NAV CANADA, the decision to conduct an assessment of the type of landing system on a runway is based on the efficiency of aircraft operations related to airport accessibility and usability.
Although the number of aircraft movements on Runway 05 increased steadily between March 2014 and March 2015, "and it was the runway most frequently used during snow events in 2014",Footnote 106 NAV CANADA did not consider this a change in accessibility that would necessitate a review of the type of landing system installed on Runway 05.
NAV CANADA holds customer forums in which issues are raised by pilots and stakeholders. These forums include the Air Transport Operations Consultation Committee and ANSNAC meetings at the national level, and the Area Operations Consultation Meetings at the Flight Information Region level, all held biannually.
In addition to these consultation sessions, 8 other working groups, which meet monthly, report through a collaborative discussion and communication process. As well, NAV CANADA's Customer Service Centre provides customers with a single point of contact to express concerns or obtain answers to questions. According to NAV CANADA, from 1998 to the date of the occurrence, no formal request through any of the above venues, had been made to install an ILS on Runway 05 at CYHZ.
1.18.13 Airport utility power supply
Almost immediately following the utility power outage, the airport's 2 standby generators started and ran up to rated voltage and frequency. A reverse power fault on one of the generator voltage regulators caused one of the generators to stop producing power. Subsequently, an overload situation was experienced by the other generator. Approximately 10 minutes later, this generator initiated an emergency shutdown, which cut power to the terminal building.
The terminal building remained without power for approximately 1 hour. During this time, the airport operations' radio repeaters, which were interconnected by a network switch, and the landline telephone system did not function. Although the repeaters were wired to uninterruptible power supplies to provide a backup source of electrical power in case of an emergency, the network switch was not. Therefore, the complete radio network was unavailable throughout the electrical power outage. HIAA emergency response personnel used their simplex radio channel to communicate at the accident site. At approximately 0140, HIAA personnel restarted one of the generators, which then provided emergency power until utility power was restored at 0148.
About a month before the accident, work had been carried out on one of the generators by a technician certified by the original equipment manufacturer. Upon completion of the work, testing was conducted on both individual generators. These tests confirmed the voltage regulation of the generators as standalone units. However, testing to establish synchronization of the 2 generators and their connection to the terminal building load did not take place. After the accident, a check of the control circuitry was carried out, and it was noted that the wiring was not in accordance with the manufacturer's specifications. It was determined that a discrepancy in the standby generators' control circuitry caused the 2 standby generators to stop producing power.
The runway lighting system is backed up by a 500 kilowatt airfield generator, which has sufficient capacity to maintain all airfield electrical loads. The generator acts as the primary power source for category II operations and as an emergency backup generator if there is a utility power loss during category I operations.
At the time of the accident, the airport was not in category II operations, so the airfield generator was on standby. It took approximately 12 seconds for the airfield generator and associated circuitry to sense the utility power failure, start up, and provide emergency power to airfield lighting and navigational aids, which was in accordance with existing regulations.Footnote 107 The Runway 05 localizer operated without interruption, as it was supported by a battery-based uninterruptible power supply.
1.18.14 Emergency response plan
CARs 302.203 specifies the minimum elements that must be identified in an airport operator's emergency plan, including potential emergencies, organizations at the airport and in the community that are capable of providing assistance, other resources available at the airport and in the surrounding communities for use during emergency response, measures for dealing with adverse climatic conditions and darkness, and procedures to assist persons who have been evacuated.Footnote 108
The HIAA emergency response plan (ERP) identified organizations and their responsibilities; a concept of emergency operations; measures for protection of personnel, facilities, and equipment; and emergency preparedness. Although an ERP establishes procedures for potential emergencies at the airport, it is impossible to design procedures for every situation; therefore, the ERP in place may be adapted to suit the emergency at hand. The HIAA regularly conducts exercises in emergency preparedness, including a biannual telecommunications exercise, an annual study and tabletop exercise on various airport emergency scenarios, and a full-scale exercise (at least once every 2 years).
The ICAO manual on airport emergency planningFootnote 109 states that all transportation resources available at the airport, such as vans and buses, should be inventoried and included in the airport's ERP, notably for the transportation of uninjured passengers to a designated holding area. The ICAO manual also states that the airport authority, aircraft operator, or other predesignated agency can be made responsible for the transportation of the uninjured from the accident site to a designated holding area.
There is no CARs requirement that specifies who is responsible for providing transportation from an on-airport accident site to an emergency assistance centre. In Canada, this responsibility is assumed by the airport authority at some airports, whereas it is assumed by the airlines at other airports.
Air Canada's ERP for CYHZ indicated that the airline was responsible for the transportation of passengers from an accident site, and that this could be done in coordination with the airport authority. HIAA's ERP also indicated that it was the airline's responsibility to transport passengers from the accident site.
Air Canada's ERP did not identify the airport's Park'N Fly (PnF) mini-buses as transportation resources. The HIAA's ERP did not identify that the airport PnF mini-buses could be used to transport uninjured passengers, nor did it provide instruction on when and how to request and dispatch any transportation resources available at the airport. However, during the HIAA's emergency preparedness exercises, the HIAA's practice was to consider the use of the airport PnF mini-buses for this purpose.
1.18.15 Movement of passengers
HIAA has indicated that a request to dispatch non-emergency vehicles, such as the PnF mini-buses, would be made only after ERS has specified that an accident site is all clear and that all the passengers have been evacuated from the aircraft.
About 0043, after having been contacted by the ERS firefighters at the accident site, the duty manager contacted the airport security supervisor to make arrangements to dispatch the 4 PnF mini-buses to the accident site.Footnote 110 At the time of the occurrence, there was 1 PnF bus in service, 3 PnF mini-buses parked in the PnF parking lot, and no airport mobile patrol vehicles in service. Because the airport ground operations radio network was unserviceable, the security supervisor could not broadcast over the radio to all personnel at the same time, and had to make individual telephone calls.
Several cellphone calls were made between airport personnel to make arrangements for the 4 PnF mini-buses and patrol vehicles. The PnF bus in service was instructed to go to the south gate. Security personnel were instructed to mobilize 2 patrol vehicles and the 3 parked PnF mini-buses. Once mobilized, these vehicles were also to go to the south gate.
About 0100, the first airport patrol arrived at the gate. Because of the power outage, the gate had to be opened manually. About 2 minutes later, the patrol vehicle escorted a police vehicle to the accident site.
Just after 0105, the second patrol vehicle arrived at the gate and provided escort for 2 PnF mini-buses as well as several ambulances and police vehicles. The vehicles left as a convoy and, because the location of the accident site was not clearly identified, the convoy initially went to the south apron. After the accident location was clarified, the convoy was redirected and arrived at the accident site at about 0120. Driving conditions at the airport were hampered by the snow accumulation and by poor visibility due to the blowing snow.
1.18.16 Safety study of evacuations of large, passenger-carrying aircraft
In 1995, the TSB published A Safety Study of Evacuations of Large, Passenger-Carrying Aircraft.Footnote 111 Twenty-one occurrences involving emergency evacuations were reviewed. In 8 of the 21 occurrences, the aircraft's PA system was inoperable or inaudible following the accident. As a result, cabin crew or passengers did not hear the initial command to evacuate or other emergency instructions. As a result, these evacuations were delayed, placing the safety of passengers and crew at risk.
1.18.17 Previous accident involving frame 65 floor penetration
In January 2009, US Airways flight 1549, an Airbus A320-214 (N106US), experienced an almost total loss of thrust in both engines after encountering a flock of birds and was subsequently ditched on the Hudson River about 8.5 miles from LaGuardia Airport, New York City, New York.
The NTSB determined that, during the impact with the water, the FR65 vertical beam penetrated the cabin floor adjacent to the flight attendant's aft, direct-view jump seat, injuring the flight attendant seated there.Footnote 112
The NTSB made the following recommendation (Safety Recommendation A-10-092) to the EASA regarding the FR65 vertical beam installation:
Require Airbus to redesign the frame 65 vertical beam on A318, A319, A320, and A321 series airplanes to lessen the likelihood that it will intrude into the cabin during a ditching or gear-up landing and Airbus operators to incorporate these changes on their airplanes.
In response to this recommendation, Airbus implemented a design modification that included a redesign of the floor structure and replacement of the original one‑piece FR65 vertical beam with a new beam fabricated with a predetermined breaking point. In October 2014, EASA approved this modification for production A318, A319, A320, and A321 series aircraft. In December 2014, Airbus incorporated this modification on production aircraft (MSN 6408 and subsequent).
To address modifications for in‑service aircraft, Airbus issued Service Bulletin (SB) A320-53-1262 on 21 October 2015.
On 25 October 2016, EASA issued Airworthiness Directive 2016-0212, ATA 53 – Fuselage – Central Vertical Strut at Frame 65 – Modification. The Airworthiness Directive is effective as of 08 November 2016 and requires, within 72 months after the effective date, modification of the fuselage structure at FR65 in accordance with the instructions of Airbus SB A320-53-1262 Revision 01, SB A320-53-1333, or SB A320-53-1334, as applicable, depending on aeroplane configuration.
1.19 Useful or effective investigation techniques
Not applicable.
2.0 Analysis
The aircraft was certified, equipped, and maintained in accordance with regulations, and no discrepancies were noted that would have prevented it from operating normally. The flight crew were certified and qualified in accordance with regulations.
In an effort to understand why the accident happened, this analysis will focus on the events, conditions, and underlying factors that caused or contributed to the accident. This will include discussing approaches, training, and pilot decision making. In addition, evacuation and survivability issues will be presented, as well as medical conditions that may affect aviation safety.
2.1 Approach visibility limits
In Canada, the minimum visibility authorized by the operations specification (OPS Spec) for non-precision approaches does not take into account the type of approach lighting system (ALS) installed on the runway. However, both the European Aviation Safety Agency and the Federal Aviation Agency rules take into account the type of ALS installed on the runway when determining the minimum visibility for approaches.
Under the OPS Spec, an aircraft can carry out a non-precision approach onto a runway that has a published minimum visibility of 1 statute mile (sm), even if the reported visibility is ½ sm. Without an approach lighting requirement, in Canada this approach could be carried out with 1500 feet of approach lighting (that provided by an omnidirectional approach lighting system [ODALS]). By comparison, in the U.S., an additional 900 feet of approach lighting would be required to carry out the same approach. (The requirement is for 2400 feet of approach lighting when the visibility is ½ sm visibility.) This additional lighting would provide the flight crew with more visual cues, and these cues would be closer to the minimum descent altitude (MDA) point.
Reduced visibility can obscure visual references and reduce the time available for the flight crew to detect them. Considering that the purpose of the OPS Spec is to allow flight crews to carry out an approach in reduced visibility, a type of ALS that provides more visual cues over a longer distance would assist the flight crew in determining the aircraft position and rate of change of position.
If the type of approach lighting system on a runway is not factored into the minimum visibility required to carry out an approach, in conditions of reduced visibility, the lighting available risks being less than adequate for flight crews to assess the aircraft's position and decide whether or not to continue the approach to a safe landing.
2.2 Air Canada flight path angle training
The stabilized constant descent angle technique involves flying a constant descent angle so that the aircraft will cross the runway threshold at the correct height. This angle corresponds to the published vertical descent angle (VDA), which defines the flight profile in which the aircraft will cross the runway threshold about 50 feet above ground level (AGL) to ensure landing within the touchdown zone.
One way a pilot can verify the aircraft is on a flight profile consistent with the VDA is to monitor the aircraft's altitude and distance from the threshold. Since 2014, both NAV CANADA and Jeppesen have included a distance/altitude table on selected charts.
Air Canada's standard operating procedure and historical practice when flying in flight path angle (FPA) guidance mode was that once the aircraft was past the final approach fix (FAF), the flight crews were not required to monitor the aircraft's altitude and distance from the threshold or to make any adjustments to the FPA. This practice was not in accordance with Air Canada's and Airbus's flight crew operating manuals (FCOM).
Although TC reviewed and approved Air Canada's AOM and the SOPs, it had not identified the discrepancy between the Air Canada SOPs and the Airbus FCOM regarding the requirement to monitor the aircraft's vertical flight path beyond the final approach fix when the FPA guidance mode is engaged.
Flight crews select an FPA that corresponds to the published VDA, and the aircraft's autopilot system maintains the selected FPA. However, in the FPA guidance mode, the aircraft is susceptible to perturbations which, if not compensated for by manual corrections to the FPA, could alter the flight profile. If such perturbations are present during an approach and flight crews are following Air Canada's practice, flight crews could be unaware of their effect on the selected flight path.
If the actual flight path deviates from the selected flight path as defined by the published VDA, flight crews may have to make adjustments to the flight profile in order to safely continue on with the visual portion of the approach to touchdown. During a stable approach, these adjustments could be minor and may not be sufficient to result in a deviation from stable approach criteria.
2.3 Approach
During the occurrence flight, as per Air Canada's practice, once the FPA was selected and the aircraft began to descend, the flight crew did not monitor the altitude and distance from the threshold, nor did they make any adjustments to the FPA. The approach was considered stable and consistent with Air Canada's training. The flight crew did not notice that the aircraft had drifted below and diverged from the planned VDA flight profile, nor were they aware that the aircraft had crossed the minimum descent altitude further back from the threshold.
2.4 Visibility
2.4.1 Visual cues
Even in clear weather, judging an aircraft's position relative to the desired vertical flight path can be challenging during a night landing, particularly if there is minimal cultural lighting on the approach path to a runway.
During this occurrence, the visual cues that would have been available to the flight crew included the ODALS, the runway lights, and the precision approach path indicators. The reduced visibility would have diminished the ability of the flight crew to make use of these cues, either by obscuring them or by reducing the time that they were available. The blowing snow likely exacerbated this situation by momentarily or continuously obscuring some or all of the visual cues.
2.4.2 Visibility estimates
The flight crew recognized that having the approach and runway lights at their brightest selection would make it easier to acquire and maintain the visual cues necessary to conduct a safe landing. The flight crew requested, and the tower controller confirmed, that the runway lights would be on setting 5 for the landing. However, the approach and runway lights were not changed from setting 4 to setting 5; therefore, these lights were not at their maximum brightness setting during the approach.
The reduced visibility, exacerbated by the blowing snow and lack of cultural lighting along the flight path, would have made it difficult for the flight crew to assess the aircraft position and rate of change of position. The flight crew expected to see the approach and runway lights at their maximum brightness. However, the dimmer lights would have created the illusion that the aircraft was further from the threshold than it actually was. This may have led the flight crew to believe that there was more time available to assess the aircraft position in relation to the runway.
When the pilot monitoring called, "Lights only," the aircraft was about 1.0 nm from the threshold and about 0.35 nm (less than ½ sm) from the only lighted facility on the approach path.
During the approach, the ODALS were on medium setting and the runway lights were on setting 4. The visual cues that may have been available to the flight crew at the MDA can be estimated based on both the ½ sm reported ground visibility and the theoretical visibilities provided by TC.
Based on the reported visibility of ½ sm, the following visual cues may have been available to the flight crew:
- when the aircraft was at the calculated MDA: the lighted facility on the approach path;
- when the aircraft was about 3700 feet from the threshold and the flight crew discussed whether each had acquired the lights: the first 2 ODALS lights; and
- when the aircraft was about 2000 feet from the threshold and the autopilot system was disconnected: all of the ODALS lights and the first 3 pairs of runway edge lights.
Based on the theoretical data provided by TC, the following visual cues may have been available to the flight crew:
- when the aircraft was at the calculated MDA point: the first 3 ODALS lights;
- when the aircraft was about 3700 feet from the threshold and the flight crew discussed whether each had acquired the lights: all of the ODALS lights and about 10 pairs of the runway edge lights; and
- when the aircraft was about 2000 feet from the threshold and the autopilot system was disconnected: all of the ODALS lights and about 19 pairs of the runway edge lights.
With the runway lights and the ODALS on their maximum settings, using the theoretical data provided by TC at the calculated MDA, the flight crew may have been able to see all of the ODALS and at least the first 3 pairs of the runway edge lights.
In the 15 minutes leading up to the accident, the Runway 23 runway visual range (RVR) B values fluctuated above and below the last reported value for ground visibility. Since ground visibility may not be representative of flight visibility, the actual visibility for the flight crew at any point along the approach path cannot be known.
2.5 Decision to continue the approach
In understanding why the flight crew continued the approach and did not consider a go-around, it is important to consider that the flight crew was interpreting the available visual cues in the context in which they were presented.
Both flight crew members had detected ground lighting between the final approach fix and the MDA, which likely reinforced their expectation that they would acquire the required visual reference at the MDA and that a landing could be carried out successfully. As the aircraft reached the calculated MDA, both crew members observed some approach lights. These cues meet the criteria for required visual reference per the Air Canada Flight Operations Manual, the Transport Canada Aeronautical Information Manual, and the Canada Air Pilot general pages.
Having visually acquired a portion of the ALS at the MDA, the flight crew decided to continue the approach.
As an aircraft moves closer to the runway, it is expected that visual cues associated with the runway environment—particularly the number and intensity of the lights—will become increasingly visible. In this occurrence, the conditions for the flight crew to acquire and maintain the visual cues would have been challenging because the aircraft crossed the MDA 0.3 nm farther back than the published distance and visibility was reduced by blowing snow.
At the MDA, the flight crew were occupied with the need to assess the aircraft's position and its rate of change of position. The flight crew were relying on the approach and runway lights to achieve this. Using the aircraft's autopilot system allows more time and resources to assess the overall operational situation.
Considering the challenging conditions to acquire and maintain the visual cues, it is likely that the flight crew delayed disconnecting the autopilot until beyond the minimum descent altitude because of their reliance on the autopilot system.
Flight crews can be subject to a plan continuation bias: without salient triggers, they will continue with their original plan (that is, to carry out the landing). In this occurrence, there was nothing particularly significant to cause the flight crew to re-evaluate their original plan of action. Therefore, the flight crew's recognition that the aircraft was too low at that point during the approach would have been delayed because of plan continuation bias.
Visibility estimates indicate that a portion of the runway lighting may have been visible to the flight crew on the approach. To detect any change in the aircraft's position relative to the runway, the flight crew would have used cues such as the aspect ratio between the runway edge lights and threshold lights, the linear perspective of the runway lights, and the amount of space between each runway edge light. However, the cues would have appeared late in the approach and the flight crew would not had much time to interpret and react to them. The uphill slope on the runway may also have aggravated the situation.
Although the flight crew eventually became aware that the runway environment did not look as it should have and began a go-around, they did so too late in the approach sequence to avoid the aircraft colliding with terrain.
The limited number of visual cues and the short time that they were available to the flight crew, combined with potential visual illusions and the reduced brightness of the approach and runway lights, diminished the flight crew's ability to detect that the aircraft's approach path was taking it short of the runway.
Although a go-around was initiated, the aircraft stuck terrain approximately 740 feet short of the runway threshold, bounced twice, and then slid along the runway before coming to a rest approximately 1900 feet beyond the runway threshold.
2.6 Cabin door
After the aircraft came to rest, the L1 door was opened in the locked position. However, it was reported that the door began to slide back during the evacuation. For the door to move out of the locked position, the pushbutton to release the gust lock would have had to be activated. Considering the aircraft orientation and the direction of the wind, once the door was unlocked it would have moved toward the closed position. Therefore, it is likely that, during the evacuation, a passenger activated the L1 door gust lock release pushbutton while trying to expedite his or her exit, which allowed the door to move freely.
2.7 Cabin floor
When the aircraft's aft fuselage struck the snow‑covered ground, it caused the cargo compartment floor to be displaced upward. This forced the door net stanchions of the bulk cargo compartment and the frame 65 (FR65) vertical beam upward. Neither the FR65 vertical beam nor the stanchions incorporated a design feature to absorb longitudinal forces. Because these components remained rigid and did not fail, they punctured the cabin floor. Although no one was injured as a result, the holes in the cabin floor could have posed an obstacle to egress, as passengers could have tripped on the raised floor material.
Airbus has implemented a design change for the FR65 vertical beam, which now incorporates a predetermined breaking point. However, the stanchion design remains unchanged; therefore, there is still a risk that the stanchions will penetrate the cabin floor when the fuselage strikes the water or ground. There is a similar risk for any vertically mounted, non-structural beam (channel, tube, etc.) installed between the floor and ceiling of a cargo compartment.
If they do not incorporate a means of absorbing forces along their longitudinal axis, vertically mounted, non-structural beams (channels, tubes, etc.) in cargo compartments could penetrate the cabin floor when the fuselage strikes the water or ground, increasing the risk of aircraft occupants being injured or emergency egress being impaired.
2.8 Passenger seats
The passenger seat shear pins are designed to shear when the seatback is struck from behind or with an inertial load of 20g. No damage consistent with a 20g inertial load was observed.
During the impact sequence, some passengers came into contact with the seatbacks in front of them and others used the seatbacks to brace themselves. As well, it is likely that some passengers bumped into seatbacks during the emergency egress as they tried to exit the aircraft quickly.
This contact with passengers likely caused the shear pins to shear, which in turn led to the seatbacks dislodging.
2.9 Flight crew shoulder-harness assembly
2.9.1 Captain
Although the captain wore his restraint system, his head struck the glare shield. During the impact sequence, the captain would have been exposed to intermittent acceleration forces as the aircraft struck the ground twice and slid along the runway. Because the forces were intermittent, the shoulder harness would have repeatedly locked and unlocked, which would have allowed the captain to be flung about. At some time during the impact sequence, the captain's head struck the glare shield because there were insufficient acceleration forces to lock the shoulder harness and prevent movement of his upper body.
2.9.2 First officer
The first officer's (FO's) right shoulder harness was damaged so that the automatic locking feature of the inertia reel was unserviceable. Without the locking feature, the harness allowed unrestrained motion in all conditions.
In addition, as a result of this type of damage, if a sudden acceleration force were applied to the FO's harness, then only the left side of his body would be restrained, resulting in his upper body twisting to the left. The location of the dent in the glare shield and the type of injury to the FO's head were consistent with his body twisting to the left as it moved forward, allowing the right side of his head to contact the glare shield during the impact sequence. The first officer sustained a head injury and a serious injury to the right eye as a result of striking the glare shield because the automatic locking feature of the right-side shoulder-harness inertia reel was unserviceable.
The flight crew restraint system is designed to restrain the occupant of the seat. The purpose of the shoulder-harness assembly is to prevent the occupant from accelerating forward and to so minimize the risk of injury or death. If the shoulder-harness assembly is unserviceable and does not lock during a sudden acceleration, then the seat occupant is at a much greater risk of injury or death during an accident. Performing a proper pull test verifies that the shoulder-harness assembly is airworthy and therefore capable of restraining the occupant of the seat during an accident.
Although the restraint system maintenance manual provided inspection intervals and criteria to determine whether the shoulder-harness assemblies were in an airworthy condition, this information was not included on the Airbus maintenance task card nor, as a consequence, on the Air Canada maintenance task card.
Given the safety-critical importance of having an airworthy shoulder-harness assembly, and in the absence of published instructions, Air Canada developed a typical practice to verify that the shoulder harness inertia reel would lock under a forward acceleration.
The damage noted on the FO's shoulder harness was consistent with conducting a pull test without first extending the strap. It could not be determined when the plastic flange had fractured and rendered the FO's shoulder harness unserviceable.
If an aircraft manufacturer's maintenance instructions do not include the component manufacturer's safety-critical test criteria, the component risks not being maintained in an airworthy condition.
2.10 Coffee brewer assembly
During the impact sequence, the coffee brewer assembly would have been jolted repeatedly. This would have caused the locking lever, which had been previously damaged, to move away from the brewer housing and would have allowed the spring-loaded locking mechanism to release. Once the locking mechanism was released, the brewer was free to move. The flight attendant was injured by a coffee brewer that came free of its mounting base because its locking system was not correctly engaged.
2.11 Passenger address system
The passenger address (PA) system was serviceable until electrical and battery power were completely lost.
In an evacuation, the flight and cabin crews typically use the PA system to convey critical safety information to passengers. If there is a complete loss of electrical and battery power and the PA system does not have an independent emergency power supply, the PA system will be inoperable, and the initial command to evacuate or to convey other emergency instructions may be delayed, putting the safety of passengers and crew at risk.
2.12 Passenger safety and emergency information
During a planned or prepared emergency, the cabin crew carry out an emergency briefing, which includes an instruction for passengers to leave their carry-on baggage behind and describes what the brace position is and how and when to adopt it. However, during an unplanned emergency, the cabin crew does not have time to provide this briefing and, therefore, must adapt to the situation at hand.
Before departing from Toronto, the cabin crew provided the pre-departure safety briefing, which included instructions for passengers to leave their carry-on baggage behind in an emergency and to review the safety-features cards for additional safety information. The safety-features card reiterated the instruction to leave carry-on baggage behind in an emergency and included a pictogram of the brace positions. Research has shown that passengers typically pay little attention to the pre-departure briefings and to the safety-features cards.
Once the aircraft had come to a stop, the cabin crew instructed the passengers to leave their carry-on baggage behind. In spite of these instructions as well as the instructions provided in the pre-departure briefing and the safety-features card, some passengers exited the aircraft with their carry-on baggage. Such behaviour can impede egress and injure passengers and cabin crew. If passengers retrieve or attempt to retrieve their carry-on baggage during an evacuation, they are putting themselves and other passengers at a greater risk of injury or death.
In this occurrence, some of the passengers had not reviewed the safety-features card and, therefore, were unfamiliar with the brace position.
If passengers do not pay attention to the pre-departure safety briefings or review the safety-features cards, they may be unprepared to react appropriately in an accident, increasing their risk of injury or death.
2.13 Transportation of occupants post-accident
Timely transportation of evacuated passengers and crew to a safe holding area is important, and even more so in harsh weather conditions when aircraft occupants are without shelter. The Canadian Aviation Regulations and the International Civil Aviation Organization guidelines identify the need to include available resources for transporting people in an organization's emergency response plan (ERP).
The transportation of passengers and crew from an on-airport accident site is a widely known scenario, and one for which organizations should be prepared. About 7 minutes after the aircraft came to a stop, airport staff were made aware of the passenger evacuation. However, a request for transportation was not initiated immediately because the emergency response services (ERS) had not stated that the site was all clear.
Delaying the dispatch of non-emergency vehicles to the accident site allows the ERS to focus on their emergency-response duties and responsibilities, and having non-emergency vehicles on site could impede the ERS's activities. However, making concurrent arrangements to have the transportation vehicles ready to deploy once the all-clear message has been received would minimize the time that passengers wait at the accident site. Additionally, having a list of all available transportation resources, and instructions on when and how to request and dispatch those resources, could further expedite moving passengers and crew from the accident site.
Although both the Halifax International Airport Authority's (HIAA's) ERP and Air Canada's ERP identified that it was Air Canada's responsibility to arrange for transportation of passengers from an on-airport accident site, neither Air Canada's nor the HIAA's ERP identified that the airport Park'N Fly (PnF) mini-buses could be used for transporting uninjured passengers. If an organization's ERP does not identify all available transportation resources, there is an increased risk that evacuated passengers and crew will not be moved from an accident site in a timely manner.
However, when carrying out emergency-preparedness exercises, HIAA's practice was to consider the use of the PnF mini-buses for this purpose. Although the airport emergency-preparedness exercises considered this, it was not practised during these exercises.
At about 0043, within about 1 minute after receiving the all-clear message from the ERS, the HIAA duty manager initiated the request for the PnF mini-buses. Action was taken to start dispatching the PnF mini-buses and the airport patrol vehicles about 5 minutes later. Coordinating this dispatch without the operations radio network made it difficult to communicate with individuals and impossible to broadcast collective messages. In addition, instructions given to the vehicle drivers over cellular phones did not provide a clear description of where the aircraft was located, and airside access was delayed because the gate had to be opened manually owing to the electrical power outage. Travel to the accident site was also hindered by snow-covered roads and poor visibility. As well, vehicles initially proceeded to the wrong location and had to be redirected to the accident site. If organizations do not practise transporting persons from an on-airport accident site, then they may be insufficiently prepared to react appropriately to an actual accident, which may increase the time required to evacuate the passengers and crew.
Recovery of the uninjured passengers from the accident site was delayed as a result of a number of factors, including the severe weather conditions; the failure of the airport's 2 standby generators to provide backup power after the loss of utility power; the loss of the airport operations radio network; and the lack of arrangements for the dispatch of transportation vehicles until after ERS had advised that all passengers were evacuated and the site was all clear.
2.14 Transport Canada's management of obstructive sleep apnea in pilots
Obstructive sleep apnea (OSA) is a medical disorder that, if left untreated, can lead to performance impairments and other aeromedically relevant conditions. In pilots who suffer from the disorder, adequate treatment of OSA is essential to be deemed medically fit to fly.
Given that the TC Civil Aviation Medical Examiner (CAME) is usually the only person who physically examines the applicant and makes a recommendation for medical certification, it would be reasonable to expect the guidance provided to CAMEs to include information related to OSA. However, TC's Handbook for Civil Aviation Medical Examiners (2004) does not provide specific information regarding OSA.
TC has indicated that it has an undocumented protocol for the assessment and ongoing surveillance of OSA in pilots. However, the actual method and practice used are typically left up to the individual CAME and regional aviation medical officer (RAMO), and is based on what they know about OSA and on what the pilot has reported to them. Pilots with OSA considered to be adequately treated were deemed medically fit. In the captain's case, because no daytime sleepiness had been reported, TC deemed him to be medically fit.
If TC does not consistently follow its protocol for the assessment of aeromedical risk and ongoing surveillance in applicants who suffer from obstructive sleep apnea, some of the safety benefit of medical examinations will be lost, increasing the risk that pilots will fly with a medical condition that poses a risk to safety.
3.0 Findings
3.1 Findings as to causes and contributing factors
- Air Canada's standard operating procedure (SOP) and practice when flying in flight path angle guidance mode was that, once the aircraft was past the final approach fix, the flight crews were not required to monitor the aircraft's altitude and distance from the threshold or to make any adjustments to the flight path angle. This practice was not in accordance with the flight crew operating manuals of Air Canada or Airbus.
- As per Air Canada's practice, once the flight path angle was selected and the aircraft began to descend, the flight crew did not monitor the altitude and distance from the threshold, nor did they make any adjustments to the flight path angle.
- The flight crew did not notice that the aircraft had drifted below and diverged from the planned vertical descent angle flight profile, nor were they aware that the aircraft had crossed the minimum descent altitude further back from the threshold.
- Considering the challenging conditions to acquire and maintain the visual cues, it is likely the flight crew delayed disconnecting the autopilot until beyond the minimum descent altitude because of their reliance on the autopilot system.
- The approach and runway lights were not changed from setting 4 to setting 5; therefore, these lights were not at their maximum brightness setting during the approach.
- The system to control the airfield lighting's preset selections for brightness setting 4 was not in accordance with the NAV CANADA Air Traffic Control Manual of Operations requirement for the omnidirectional approach lighting system to be at its brightest settings.
- The limited number of visual cues and the short time that they were available to the flight crew, combined with potential visual illusions and the reduced brightness of the approach and runway lights, diminished the flight crew's ability to detect that the aircraft's approach path was taking it short of the runway.
- The flight crew's recognition that the aircraft was too low during the approach would have been delayed because of plan continuation bias.
- The aircraft struck terrain approximately 740 feet short of the runway threshold, bounced twice, and then slid along the runway before coming to a rest approximately 1900 feet beyond the runway threshold.
- At some time during the impact sequence, the captain's head struck the glare shield because there were insufficient acceleration forces to lock the shoulder harness and prevent movement of his upper body.
- The first officer sustained a head injury and serious injury to the right eye as a result of striking the glare shield because the automatic locking feature of the right-side shoulder-harness inertia reel was unserviceable.
- A flight attendant was injured by a coffee brewer that came free of its mounting base because its locking system was not correctly engaged.
- Because no emergency was expected, the passengers and cabin crew were not in a brace position at the time of the initial impact.
- Most of the injuries sustained by the passengers were consistent with not adopting a brace position.
3.2 Findings as to risk
- If aircraft cockpit voice recorder installations do not have an independent power supply, additional, potentially valuable information will not be available for an investigation.
- If Transport Canada does not consistently follow its protocol for the assessment of aeromedical risk and ongoing surveillance in applicants who suffer from obstructive sleep apnea, some of the safety benefit of medical examinations will be lost, increasing the risk that pilots will fly with a medical condition that poses a risk to safety.
- If new regulations on the use of child-restraint systems are not implemented, lap-held infants and young children are exposed to undue risk and are not provided with a level of safety equivalent to that for adult passengers.
- If passengers do not dress appropriately for safe travel, they risk being unprepared for adverse weather conditions during an emergency evacuation.
- If the type of approach lighting system on a runway is not factored into the minimum visibility required to carry out an approach, in conditions of reduced visibility, the lighting available risks being less than adequate for flight crews to assess the aircraft's position and decide whether or not to continue the approach to a safe landing.
- If they do not incorporate a means of absorbing forces along their longitudinal axis, vertically mounted, non-structural beams (channels, tubes, etc.) in cargo compartments could penetrate the cabin floor when the fuselage strikes the water or ground, increasing the risk of aircraft occupants being injured or emergency egress being impaired.
- If an aircraft manufacturer's maintenance instructions do not include the component manufacturer's safety-critical test criteria, the component risks not being maintained in an airworthy condition.
- If there is a complete loss of electrical and battery power and the passenger address system does not have an independent emergency power supply, the passenger address system will be inoperable, and the initial command to evacuate or to convey other emergency instructions may be delayed, putting the safety of passengers and crew at risk.
- If passengers retrieve or attempt to retrieve their carry-on baggage during an evacuation, they are putting themselves and other passengers at a greater risk of injury or death.
- If passengers do not pay attention to the pre-departure safety briefings or review the safety-features cards, they may be unprepared to react appropriately in an accident, increasing their risk of injury or death.
- If an organization's emergency response plan does not identify all available transportation resources, there is an increased risk that evacuated passengers and crew will not be moved from an accident site in a timely manner.
- If organizations do not practise transporting persons from an on-airport accident site, they may be insufficiently prepared to react appropriately to an actual accident, which may increase the time required to evacuate the passengers and crew.
3.3 Other findings
- The service director assessed the evacuation flow as good and determined that there was therefore no need to open the R1 door.
- The flight attendants stationed in the rear of the aircraft noted no life-threatening hazards. Because no evacuation order had been given, and deplaned passengers and firefighters were observed walking near the rear of the aircraft in an area where the deployment of the rear slides may have created additional hazards or risks, the flight attendants determined that there was no requirement to open the L2 and R2 doors.
- Although Transport Canada required the dual-exit drill to be implemented in training, it did not require all cabin crew to receive the training before an organization implemented the 1:50 ratio.
- At the time of the accident, neither the service director nor the flight attendants had received the dual-exit training, nor were they aware of the requirement for such training in order for Air Canada to operate with the exemption allowing 1 flight attendant for each unit of 50 passengers.
- Although Transport Canada had reviewed and approved Air Canada's aircraft operating manual and the standard operating procedures (SOPs), it had not identified the discrepancy between the Air Canada SOPs and the Airbus flight crew operating manual regarding the requirement to monitor the aircraft's vertical flight path beyond the final approach fix when the flight path angle guidance mode is engaged.
- A discrepancy in the Halifax International Airport Authority's standby generators' control circuitry caused the 2 standby generators to stop producing power.
- Air Canada's emergency response plan for Halifax/Stanfield International Airport indicated that the airline was responsible for the transportation of passengers from an accident site.
- Air Canada's emergency response plan did not identify the airport's Park'N Fly mini-buses as transportation resources.
- The Halifax International Airport Authority's emergency response plan did not identify that the airport Park'N Fly mini-buses could be used to transport the uninjured passengers, nor did it provide instructions on when and how to request and dispatch any transportation resources available at the airport.
- The Air Canada Flight Operations Manual did not identify that the required visual reference should enable the pilot to assess aircraft position and rate of change of position in order to continue the approach to a landing.
- In Canada, the minimum visibility that is authorized by the operations specification for non-precision approaches does not take into account the type of approach lighting system installed on the runway.
- It is likely that, during the emergency, a passenger activated the L1 door gust lock release pushbutton while trying to expedite his or her exit, which allowed the door to move freely.
- The passenger seatbacks were dislodged because the shear pins had sheared, likely as a result of contact with passengers during the impact sequence or emergency egress.
- Recovery of the uninjured passengers from the accident site was delayed owing to a number of factors, including the severe weather conditions; the failure of the airport's 2 standby generators to provide backup power after the loss of utility power; the loss of the airport operations radio network; and the lack of arrangements for the dispatch of transportation vehicles until after emergency response services had advised that all passengers were evacuated and the site was all clear.
- Given that the captain rarely used continuous positive airway pressure therapy, he would have been at risk of experiencing fatigue related to chronic sleep disruption caused by obstructive sleep apnea. However, there was no indication that fatigue played a causal or contributory role in this occurrence.
4.0 Safety action
4.1 Safety action taken
4.1.1 Air Canada
Air Canada has issued the following documentation:
- Flight Operations Manual (FOM) Bulletin 324, which amends the FOM Approach Policy in a number of areas, including the following changes:
- The Required Visual Reference list now includes VASI/PAPI [visual approach slope indicator/precision approach path indicator] as an option.
- The definition of Required Visual Reference has been amended.
- The "lights only" call has been removed from standard operating procedures.
- Pilot monitoring duties have been modified to require a greater emphasis on instrument monitoring during all approaches after the minimum descent altitude.
- The Approach Visibility Requirements in Canada – 75% of Charted Visibility section for non-precision approaches has been revised to reflect the link between approved minimums and approach lighting requirements.
- FOM Bulletin 322: Threat-Based Briefings, which codifies and embeds the threat-based briefing format for all departure and approach briefings into the Air Canada standard operating procedures.
- Aircraft Technical Bulletin 482: Revised NPA [non-precision approach] Vertical Descent Approaches, to provide clarity when flying Vertically Selected Non-Precision Approaches. The bulletin contains the following warning: "FPA [flight path angle] is not a vertical navigation system. It is an angle in space. The aircraft may drift above or below the vertical profile."
Air Canada has submitted a letter to Transport Canada requesting that the standard for approach minimums be tied to the approach lighting capability of the runway, and that the corrected minimums be published on the approach plates.
Air Canada has contacted 9 airports in Canada to recommend that they upgrade their approach lighting currently serviced by omnidirectional approach lighting system (ODALS) to simplified short-approach lighting system with runway alignment indicator lights (SSALR) systems. The airline has also coordinated and participated in specific meetings with airport authorities at Halifax, Ottawa, and Kelowna to discuss its concerns, highlight operational impacts and considerations, and advocate for immediate improvements to existing ODALS.
Air Canada is working with Airbus to develop service bulletins to install global positioning systems on the 47 Airbus aircraft that are not so equipped and has started a project to upgrade the enhanced ground proximity warning system software on all Air Canada aircraft. These updates are expected to be completed by July 2017.
Flight attendant training has been amended to incorporate practical training on 2-door operation.
Air Canada's Express regional partner airlines have aligned their non-precision approach ban policy to adopt the changes in Air Canada FOM Bulletin 324.
4.1.2 Airbus
Airbus has revised the Aircraft Maintenance Manual to reflect the seat manufacturer's component maintenance manual update, which recommends that the shoulder-harness webbing be extended 25% before testing the operation of the inertial reel.
4.1.3 Halifax International Airport Authority
In response to requests and information Halifax International Airport Authority (HIAA) received from Air Canada following this occurrence, the HIAA has installed high-intensity approach lighting systems on Runway 05 and Runway 32. The existing ODALSs on both runways were replaced with SSALR systems. Transport Canada and NAV CANADA were consulted throughout the planning, design, and construction phases.
The HIAA has equipped its emergency operations centre with updated equipment such as laptop computers, mobile radios, and wireless access points.
A backup emergency operations centre has been established.
An automated mass notification system, which is used to call back personnel during emergencies, has been installed.
The emergency response plan has been revised to include a list of on-site assets available for use during emergencies.
The emergency response vehicles have been fitted with rescue sheets, which are thermal blankets for survival emergencies.
The frequency of testing of the personal communication system has been increased.
An intelligent uninterrupted power supply, which monitors and identifies faults and usage, has been installed for the network switch.
The utility service to the airport's main electrical substation has been upgraded to provide automatic switching between 2 distinct utility feeds, supplied from 2 independent Nova Scotia Power substations.
The standby diesel generator power system has been upgraded. The existing system was replaced with a new system using 3 generators. The new arrangement provides redundant capacity so that the standby system will be able to supply the full electrical load of the airport with only 2 of the 3 generators operating.
4.1.4 NAV CANADA
NAV CANADA issued a directive (effective 15 January 2016) to air traffic control personnel regarding the anomaly in the lighting panel preset buttons. The directive included instructions to refer to their Manual of Operations for lighting settings.
NAV CANADA accelerated the publication of revised global navigation satellite system (GNSS) procedures for Runway 05, which was released in August 2015.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was first released on .
Correction
The report has been amended to include a footnote (footnote 15) in the fourth paragraph before Figure 1 to indicate that the occurrence aircraft's altimeters were set correctly.
In addition, Table 1 in the report first released indicated that 25 people sustained minor injuries and that 112 people were not injured. The table has been corrected to show that 24 people sustained minor injuries and that 113 were not injured.
Finally, the last paragraph of the report (the second paragraph of section 4.1.4) has been amended to make it clear that NAV CANADA had accelerated publication of the revised global navigation satellite system procedures for Runway 05 in response to the occurrence, publishing them in August 2015, earlier than originally scheduled.
This correction was approved by the Board on ; the corrected version of the report was released on .
Appendices
Appendix A – Jeppesen approach chart for Halifax/Stanfield International Airport
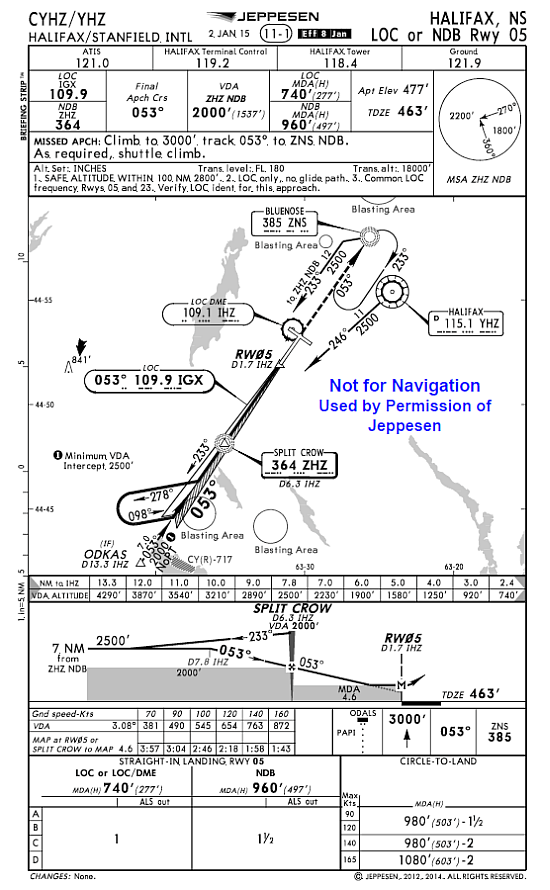
Appendix B – Jeppesen approach chart for FUNDY EIGHT standard terminal arrival route (Halifax/Stanfield International Airport)
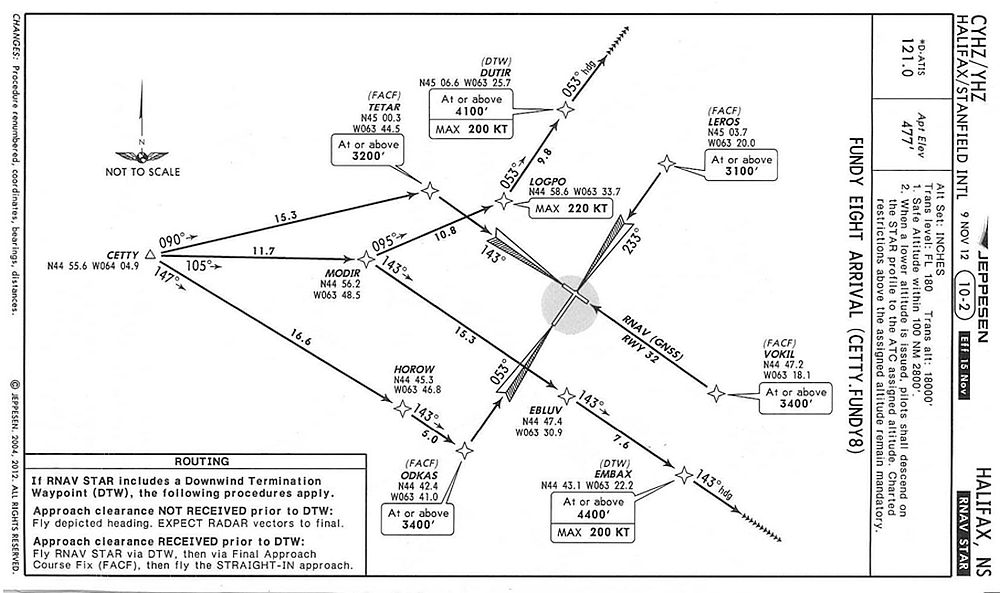
Appendix C – Aerodrome routine meteorological reports (METARs) and aerodrome forecasts (TAFs)
METAR CYHZ 282300Z 36019G26KT 1 1/2SM -SN DRSN OVC007 M04/M05 A2960 RMK SC8 SLP031=
SPECI CYHZ 282338Z 01018G24KT 3/4SM R14/2600VP6000FT/N -SN DRSN VV005 M05/M05 A2958 RMK SN8 PRESFR SLP023=
METAR CYHZ 290000Z 36016G27KT 3/4SM R14/2800FT/N -SN DRSN VV004 M05/M06 A2959 RMK SN8 /S03 PRESRR SLP028=
METAR CYHZ 290100Z 35015G21KT 1/2SM R14/3500FT/N SN DRSN VV002 M05/M06 A2962 RMK SN8 /S02/ PRESFR SLP037=
METAR CYHZ 290200Z 35019G27KT 1/4SM R14/2600FT/N +SN VV002 M06/M06 A2962 RMK SN8 /S05/ SLP036=
METAR CYHZ 290300Z 34019G25KT 1/8SM R14/P6000VM0300FT/N +SN DRSN VV003 M06/M07 A2962 RMK SN8 /S09/ SLP038=
METAR CYHZ 290300Z CCA 34019G25KT 1/4SM R14/P6000VM0300FT/N +SN DRSN VV003 M06/M07 A2962 RMK SN8 /S09/ SLP038=
SPECI CYHZ 290313Z 35020G26KT 1/2SM R14/3500V4500FT/N SN DRSN VV003 M06/M07 A2963 RMK SN8 SLP040=
METAR CYHZ 290400Z 34019G54KT 3/4SM R14/5000VP6000FT/D -SN DRSN BKN007 OVC010 M06/M07 A2964 RMK SF7SC1 SLP045=
SPECI CYHZ 290414Z 34024G33KT 3/4SM R14/P6000FT/U -SN DRSN BKN010 OVC018 M06/M07 A2965 RMK SF7SC1 SLP046=
METAR CYHZ 290500Z 33021G27KT 1 1/2SM -SN DRSN BKN013 OVC027 M06/M07 A2968 RMK SC6SC2 /S13/ SLP058=
TAF CYHZ 282044Z 2821/2918 01020G30KT 3/4SM -SN BLSN VV005 TEMPO 2821/2906 3SM -SN BLSN OVC010
FM290600 34015G25KT PSSM SCT020 OVC080 TEMPO 2906/2908 5SM -SN BKN020 BECMG 2909/2911 34012G22KT
FM291500 30010KT P6SM FEW025 BKN150
RMK NXT FCST BY 2900002=
TAF AMD CYHZ 281907Z 2819/2918 03018G28KT P6SM -SN OVC020 TEMPO 2819/2821 3/4SM -SN BLSN VV008
FM282100 01018G28KT 3/4SM -SN BLSN VV005 TEMPO 2821/2906 3SM -SN BLSN OVC010
FM290600 34015G25KT P6SM SCT020 OVC080 TEMPO 2906/2908 5SM -SN BKN020 BECMG 2909/2911 34012G22KT
FM291500 30010KT P6SM FEW025 BKN150
RMK NXT FCST BY 282100Z=
Appendix D – Approach lighting systems
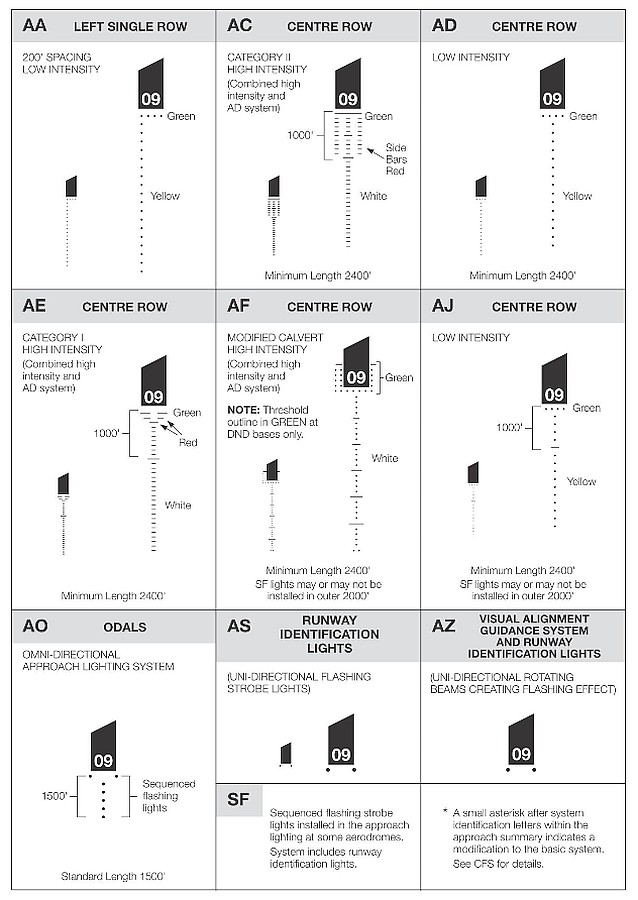
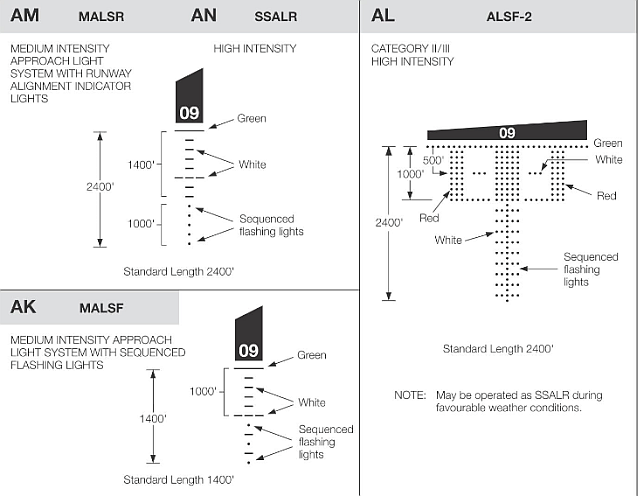
Appendix E – Glossary
- AC
- alternating current
- AC
- Advisory Circular (Transport Canada)
- AGL
- above ground level
- ALS
- approach lighting system
- AOM
- Aircraft Operating Manual
- AP
- autopilot
- AQP
- advanced qualification program
- ART
- annual recurrent training
- ASL
- above sea level
- ATC MANOPS
- Air Traffic Control Manual of Operations
- CAME
- civil aviation medical examiner
- CARs
- Canadian Aviation Regulations
- CPAP
- continuous positive airway pressure
- CVR
- cockpit voice recorder
- CYHZ
- Halifax/Stanfield International Airport, Nova Scotia
- CYQM
- Moncton/Greater Moncton International Airport, New Brunswick
- CYUL
- Montréal/Pierre Elliott Trudeau International Airport, Quebec
- CYYZ
- Toronto/Lester B. Pearson International Airport, Ontario
- DFDR
- digital flight data recorder
- EASA
- European Aviation Safety Agency
- EGPWS
- enhanced ground proximity warning system
- ELT
- emergency locator transmitter
- ERP
- emergency response plan
- ERS
- emergency response services
- FAF
- final approach fix
- FCOM
- Flight Crew Operating Manual
- FCTM
- Flight Crew Training Manual
- FO
- first officer
- FOM
- Flight Operations Manual
- FPA
- flight path angle
- fpm
- feet per minute
- GPS
- global positioning system
- GNSS
- global navigation satellite system
- HIAA
- Halifax International Airport Authority
- ICAO
- International Civil Aviation Organization
- ILS
- instrument landing system
- in. Hg
- inches of mercury
- ISA
- international standard atmosphere
- LOC
- localizer
- °M
- degree, magnetic compass
- MDA
- minimum descent altitude
- METAR
- aerodrome routine meteorological report
- NOTAM
- notice to airman
- nm
- nautical mile
- NTSB
- National Transportation Safety Board (United States)
- ODALS
- omnidirectional approach lighting system
- OPS Spec
- operations specification
- OSA
- obstructive sleep apnea
- PA
- passenger address
- PAPI
- precision approach path indicator
- PF
- pilot flying
- PFD
- primary flight display
- PM
- pilot monitoring
- PnF
- Park'N Fly
- RAMO
- regional aviation medical officer
- RAT
- ram air turbine
- RNAV
- area navigation
- RVR
- runway visual range
- SB
- Service Bulletin (Airbus)
- SCDA
- stabilized constant descent angle
- sm
- statute mile
- SMS
- safety management system
- SOPs
- standard operating procedures
- SPECI
- aerodrome meteorological special report (special weather observation)
- SSALR
- simplified short-approach lighting system with runway alignment indicator lights
- °T
- degree true
- TAF
- aerodrome forecast
- TC
- Transport Canada
- TC AIM
- Transport Canada's Aeronautical Information Manual
- TSB
- Transportation Safety Board
- VDA
- vertical descent angle
- VOR
- very high-frequency omnidirectional range
- V/S-FPA
- vertical speed/flight path angle