Loss of control and in-flight breakup
Gemini Helicopters Inc.
Robinson R44 Raven II (Helicopter), C-GOCM
Fox Creek, Alberta 21 nm SW
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Gemini Helicopters Inc. Robinson R44 Raven II (registration C-GOCM, serial number 10472) was being used to conduct monitoring of well sites southwest of Fox Creek, Alberta. At 1311 Mountain Standard Time, the helicopter departed from its base of operations at the Horse Facility gas plant camp for the day's activities. After several flights, including one with a passenger, the helicopter landed at a roadside security gate, dropped off the passenger, and departed at 1735 with only the pilot on board. The helicopter broke up in flight over a wooded area 5 minutes later. The pilot was fatally injured. There was no post-crash fire. Although the emergency locator transmitter activated on impact, no signal was received due to impact damage to the emergency locator transmitter.
Factual information
History of the flight
The Robinson R44 Raven II helicopter (registration C-GOCM, serial number 10472) was being used to monitor well sites and other facilities southwest of Fox Creek, Alberta, for a local oil company. The helicopter was flown to several well sites until 1433,Footnote 1 then was flown back to the Horse Facility base, from where it departed 3 minutes later. One more stop was made at a well site, and then at 1450, the helicopter made an unauthorized Footnote 2 flight to a roadside security gate. After 3 approaches, the helicopter landed at 1510. At 1545, the pilot was observed to be staggering and smelling of alcohol. On being questioned, the pilot uttered some derogatory remarks. The pilot and an unauthorized passenger from the security gate then boarded the helicopter. The helicopter departed at 1554 to a compressor site, landing 8 minutes later. The helicopter was left running while work was done at the site by the pilot. It departed at 1611, and was flown low along the Berland River before landing and shutting down at a remote cabin at 1630. Forty-eight minutes later, at 1718, the helicopter lifted off and flew to the location of the security gate, where it made several low passes and turns. The aircraft landed at the gate at 1731, and the passenger disembarked 2 minutes later. The helicopter took off at 1735 and was observed to be flying erratically during departure. It broke up in flight over a wooded area 5 minutes later (Appendix A).
Aircraft
The helicopter was manufactured in 2004, and was owned and operated by Gemini Helicopters Inc. (Gemini Helicopters). Records indicate that the helicopter was certified, equipped and maintained in accordance with existing regulations and approved procedures.
The investigation found that the helicopter was operating within all weight and balance limits.
The helicopter did not have a cockpit voice recorder or a flight data recorder, neither of which is required by regulation.
The helicopter had a Dart bubble window installed as per Supplemental Type Certificate (STC) SH05-13. The flight manual supplement for this installation limits the never-exceed speed (VNE) to 100 knots indicated airspeed (KIAS) with the bubble windows installed. Onboard GPS data showed that, in the minutes before the breakup, a ground speed of 127 knots was attained. Given the atmospheric conditions this equates to an indicated airspeed of approximately 126 knots.
Wreckage description
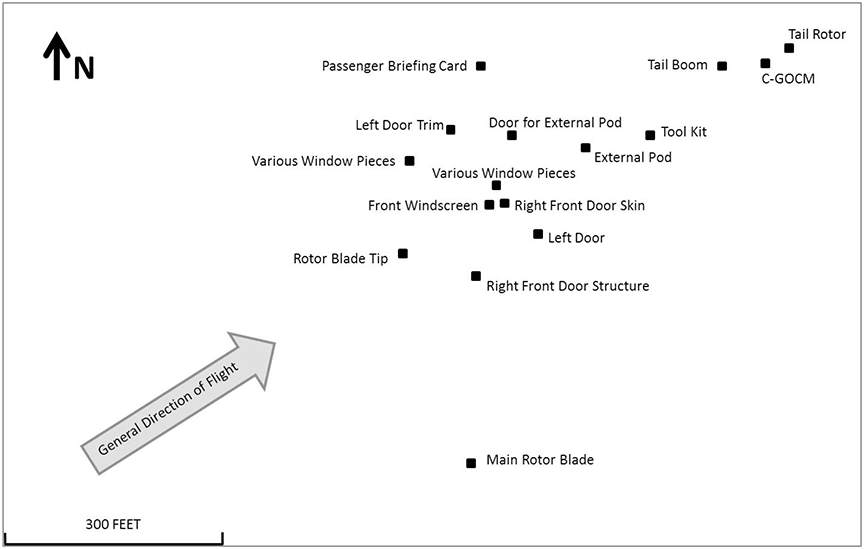
The helicopter suffered an in-flight breakup at approximately 820 feet above ground level (agl). The total length of the wreckage trail (Appendix B) was 758 feet, with the first item being one of the rotor blades (Photo 1).

Examination of the detached rotor blade indicated a bend in the downward direction from approximately mid to outer span. Damage to the blade was consistent with overload forces as a result of downward bending, air loads, and impact with the ground. The investigation determined that the blade failed at the root, very close to the mast, in an upward direction. The other main rotor blade was shown to have struck the right side of the cabin immediately beside the pilot. It also struck the cabin on the left side above the left windshield and at the left front passenger-side upper door frame. Examination of the engine and flight controls did not reveal any system failures or abnormalities that would be considered contributory to the in-flight breakup.
Causes of helicopter in-flight breakups
A main rotor excursion can lead to an in-flight breakup due to blade contact with the fuselage. In addition to catastrophic mast bumping Footnote 3 as a cause of in-flight breakup, the pilot can induce main rotor disk excursions in several ways, including through:
- high bank angles,
- low-g flight conditions, and
- rapid cyclic control movement.
With high bank angles, the rotor system can be unloaded if positive gFootnote 4 is not maintained by the pilot throughout the manoeuvre and recovery. As well, rapid cyclic reversals in roll or pitch can displace the rotor disk plane faster than the fuselage can respond, leading to blade–to–fuselage contact.
Robinson Safety Notice SN-11 (revised November 2000) deals with low-g pushovers and identifies the manoeuvre as dangerous:
Pushing the cyclic forward following a pull-up or rapid climb, or even from level flight, produces a low-G (weightless) flight condition. If the helicopter is still pitching forward when the pilot applies aft cyclic to reload the rotor, the rotor disc may tilt aft relative to the fuselage before it is reloaded. The main rotor torque reaction will then combine with tail rotor thrust to produce a powerful right rolling moment on the fuselage. With no lift from the rotor, there is no lateral control to stop the rapid right roll and mast bumping can occur. Severe in-flight mast bumping usually results in main rotor shaft separation and/or rotor blade contact with the fuselage.
The rotor must be reloaded before lateral cyclic can stop the right roll. To reload the rotor, apply an immediate gentle aft cyclic, but avoid any large aft cyclic inputs. (The low-G which occurs during a rapid autorotation entry is not a problem because lowering collective reduces both rotor lift and rotor torque at the same time.)
Never attempt to demonstrate or experiment with low-G maneuvers, regardless of your skill or experience level. Even highly experienced test pilots have been killed investigating the low-G flight condition. Always use great care to avoid any maneuver which could result in a low-G condition. Low-G mast bumping accidents are almost always fatal.Footnote 5
Weather
Visual meteorological conditions (VMC) existed at the time of the accident, and the ceiling and visibility conditions were suitable for the intended flight. The nearest aviation weather reporting station was located at the Edson Airport (CYET) in Edson, Alberta, situated 53 nautical miles (nm) southeast of the accident site. Hourly weather for CYET, taken 19 minutes after the accident, indicated that surface winds were calm, and visibility was 9 statute miles (sm), with a few clouds at 8500 feet agl. The temperature was −4°C, and the dew point was −9°C, with an altimeter setting of 29.62 inches of mercury (in. Hg).
Another aviation weather reporting station was located at the Grande Prairie Airport (CYQU) in Grande Prairie, Alberta, situated 79 nm northwest of the accident site. Hourly weather for CYQU, taken 19 minutes after the accident, indicated that surface winds were calm, and visibility was 25 sm, with scattered clouds at 6000 feet agl, a broken cloud layer at 8000 feet agl, and a third broken cloud layer at 22 000 feet agl. The temperature was −8°C, and the dew point was −9°C, with an altimeter setting of 29.62 in. Hg. The area forecast for that part of Alberta, valid at the time of the accident, indicated visibility greater than 6 sm, with broken mid-level cloud and no turbulence. A photo of the helicopter, taken approximately 2 hours before the accident and 8 nm southwest of the accident site, showed ceiling and visibility conditions consistent with the area forecast. The sun had set at 1723, with the end of civil twilight at 1802.
Company information
Gemini Helicopters operates a fleet of 20 helicopters and holds a valid air operator certificate (AOC) issued by Transport Canada under Subparts 702 and 703 of the Canadian Aviation Regulations (CARs). Gemini Helicopters provides helicopter charter services to the oil and gas sector and, over the years, has expanded its capabilities beyond transportation, offering complete airborne and ground production operation solutions. Company services are grouped into 2 divisions: helicopter charter services and production services. Gemini Helicopters' headquarters and aircraft maintenance are located in Grande Prairie, with flight operations conducted from Grande Prairie, High Level, and several field locations coincident with oil and gas customer facilities.
Gemini Helicopters did not have a safety management system (SMS) program in effect, nor was one required by Transport Canada regulations.
Flight following
Gemini Helicopters operated under a Transport Canada type D operational control system.Footnote 6 According to the CARs:
Operational control is delegated to the pilot in command of a flight by the Operations Manager, who retains responsibility for the day-to-day conduct of flight operations.
[…]Current information on the location of the air operator's aircraft shall be maintained at the main base of operations, sub-base or where appropriate, from the location from which the flight following is being carried out.
[…]Each flight shall be conducted under an IFR [instrument flight rules] Flight Plan, VFR [visual flight rules] Flight Plan or Flight Itinerary as appropriate.Footnote 7
Although the type D system only requires a flight follower during IFR and night VFR operations, the company required that a flight follower be on duty whenever an aircraft was operating. Appropriate company and search-and-rescue authorities were to be notified if the flight was overdue or missing.
Pilots were directedFootnote 8 to use one of the following methods to ensure effective flight following:
- a company flight itinerary, filed with a flight follower or a responsible person, for flights in a remote area;
- a VFR flight plan filed with NAV CANADA; or
- prearranged reporting periods if the aircraft is in constant communications with a radio operator.
Gemini Helicopters equips its helicopters with the SkyTrac onboard satellite tracking system. The system is programmed to provide a “power on” and a “power off” message, distributed as an email, each time the helicopter powers on or off, along with a position update every 1 minute. Position updates are posted to the SkyTrac website and included track, altitude and ground speed of the aircraft superimposed over a terrain map. In addition to satellite tracking, pilots are required by the Gemini Helicopters Inc. Operations Manual to send a text message through the satellite tracking system upon every shutdown landing. The text message is to alert the flight follower that the aircraft has landed safely. The SkyTrac information was monitored by a flight follower at the Gemini Helicopters base in Grande Prairie.
On the day of the accident, the pilot did not file a flight plan or a company flight itinerary with the flight follower or with a responsible person. As well, constant radio communications were not available. The pilot had not filed flight itineraries on several other flights that week. The first SkyTrac email message from C-GOCM was at 1305 and indicated that the unit was powered up. The unit operated throughout the day, giving 4 “on” and 4 “off” power cycle email messages and position updates to the web-based map every 2 minutes when power was on. The last email message occurred at 1741, when power was removed from the SkyTrac unit during the crash sequence. Although the flight follower received the SkyTrac email messages, the information was not noticed, because no flight itinerary had been received from the pilot, and the aircraft was not expected to be flying that day. The flight follower was focusing on other company aircraft operating to the north and did not have the map information displayed for the area in which C-GOCM was operating, so the position reports were not seen. C-GOCM was not reported missing until 1927 by the Horse Facility co-workers.
The Gemini Helicopters Inc. Operations Manual details the training that personnel responsible for flight following of company helicopters shall receive. Although this training program meets regulatory requirements, there was no documentation available to show that this training had been done for the individual who was on duty on the day of the accident. The flight follower was a newly hired, low-time pilot. An informal briefing and familiarization, conducted by another flight follower in late December 2012, was the only training provided to this individual before flight following duties.
Search and rescue: emergency locator transmitter
The Horse Facility personnel called the company at 1927, declaring the pilot to be missing. The flight was then reported to the Joint Rescue Coordination Centre (JRCC). A search was initiated involving a Hercules airplane and a Griffon helicopter. The Griffon helicopter had to return to base shortly after departure, due to weather en route from Edmonton, Alberta.
No emergency locator transmitter (ELT) signal was received by the search and rescue satellites (SARSAT) on the 406-MHz frequency. When the Hercules aircraft was overhead of the site assisting ground searchers, a faint 121.5-MHz signal was received. The Royal Canadian Mounted Police (RCMP) found the aircraft at approximately 0500, with the assistance of the SkyTrac data supplied by Gemini Helicopters personnel.
During initial examination of the wreckage, the ELT (Artex model ME406HM, part no. 453-6604, serial no. 197-08693) was observed to have been connected by coaxial cable to an external roof-mounted antenna and through a D-shaped multi-wire connector to a remote cockpit switch. The ELT had been separated from its mounting plate, as the Velcro retention straps had severed during impact. The ELT was hanging and still connected to the external coaxial antenna cable and antenna, both of which were intact and found in later testing to be functional. The D-shaped multi-wire connector joined to the remote switch in the cockpit had been pulled out during the crash. On this model of ELT, if the D-shaped multi-wire connector is disconnected first, the internal “g” switch cannot activate the ELT. This is a design feature intended to prevent inadvertent activation during transport for maintenance or testing. A flashing red light, indicating the activation of the ELT, was observed on the top of the ELT. The ELT was then shut off by the TSB investigator.
The ELT had been mounted in the aircraft on the upper left-hand side truss of the frame section, immediately behind and to the left of the main transmission, next to the tail rotor driveshaft coupling. The mounting system consists of a rectangular polycarbonate plastic tray affixed to the aircraft tube frame. The ELT rests within a raised box structure around the perimeter of the mounting tray and is secured by a fabric strap featuring a hook-and-loop Velcro system. When the strap is tight, the ELT is held in the mounting tray box. Instructions in the installation manualFootnote 9 direct installers to pull the loose end of the strap with enough force that the stitched seam aligns with the crown of the radius of the ELT case. This procedure had been done correctly.
On 19 April 2012, TSB Safety Advisory 825-A11W0151-D1-A2 was sent to ELT manufacturers using fabric loop-and-hook retention systems and advising that the manufacturers may wish to develop and publish methods of determining the degree of strap tightness, and to inform maintenance personnel of the necessity of proper installation.
On 23 May 2012, the United States (US) Federal Aviation Administration (FAA) issued Special Airworthiness Information Bulletin HQ-12-32, addressed to manufacturers and installers of ELTs and to aircraft maintenance personnel. The bulletin expressed concern about the ability of hook-and-loop–style fasteners to retain their designed capability to restrain ELTs during accident impact and about the quality of installation instructions for ensuring adequate tightness of the fasteners.
A new technical standard order (TSO-C126b, 406-MHz Emergency Locator Transmitter) has been approved that applies to all new applications for ELT certification. It states that Velcro fasteners are not an acceptable means of attachment for compliance with the crash safety requirements of section 2.2.5 of the Radio Technical Commission for Aeronautics document RTCA/DO-204A for automatic fixed (AF) and automatic portable (AP) ELTs. All presently certified ELTs may continue to be manufactured and installed under the previous certification standards.
Testing of the ELT in conjunction with personnel at the JRCC in Trenton, Ontario, and through use of the SARSAT system, showed that no signal was being received by orbiting satellites. The investigation determined that the unit was transmitting on 439 MHz. The unit was not opened. Further testing was conducted at the ELT manufacturer's facilities under TSB supervision. Further examinations were then conducted at the TSB Laboratory. The findings were as follows:
- The ELT's crash-sensing circuitry activated during the crash sequence.
- The ELT could not produce a proper 406-MHz signal due to impact damage to a crystal oscillator, allowing a higher than normal frequency to be transmitted. It is most likely that the oscillator was damaged during the crash sequence.
- The frequency and signal strength of the ELT's 121.5-MHz signal met the required specification.
- The ELT's antenna and antenna coaxial cable were both serviceable and properly installed at the time of the occurrence.
- The cause of the faint 121.5-MHz signal could not be positively determined; however, it may have been the result of the signal being blocked by wreckage.
This type of ELT should be able to perform properly after being subjected to a shock impulse waveform (half sine) with a magnitude of 500 g and a pulse width of 4.0 ±1.0 milliseconds in each of its 6 orthogonal axes.Footnote 10 There is also a 100-g shock test, with a requirement to pass the “aliveness” test that checks the frequency and power.Footnote 11
The highest ground speed recorded near the end of the flight was 72 km/h (65.6 feet per second). Calculations were done with speeds equal to 66 and 100 feet per second to show both a probable impact speed and a much faster and improbable impact speed. The ELT specifications specify a half sine impulse, so all calculations were with the sine impulse and were done using the WINVEST program from the TSB Laboratory.
Assuming a flight path angle of 70° and of 80° and using a 1-foot stopping distance,Footnote 12 the resulting g loads were as shown in Table 1:
| Speed (feet/second) | Flight path angle (degrees) | Stopping distance (feet) | Impact (g) |
|---|---|---|---|
| 66 | 70 | 1 | 94.6 |
| 66 | 80 | 1 | 103.1 |
| 100 | 70 | 1 | 217.3 |
| 100 | 80 | 1 | 236.7 |
Pilot information
Records indicate that the pilot was certified and qualified for the flight in accordance with existing regulations. The pilot's work-rest schedule accorded with regulations and was such that fatigue was not considered a factor in the occurrence. The pilot had been employed with Gemini Helicopters since May 2011, and had approximately 2200 hours of total flight time, with 2100 hours on the accident aircraft type. The pilot's medical examination record was valid until May 2013, and the next pilot competency check was scheduled for July 2013.
Canadian Aviation Regulations
Subpart 602.03 of the CARS states that no person shall act as a crew member of an aircraft:
- within eight hours after consuming an alcoholic beverage;
- while under the influence of alcohol; or
- while using any drug that impairs the person's faculties to the extent that the safety of the aircraft or of persons on board the aircraft is endangered in any way.Footnote 13
Medical and pathological information
The impact with the ground was not survivable.
The evening before the occurrence, the pilot had left the camp and proceeded to town to pick up a case of beer; the pilot is believed to have consumed 3 or 4 beers at the camp that evening.
It is not known when the pilot consumed additional alcohol. Following the occurrence, an empty wine bottle and an empty liquor bottle were found at the cabin. There was no other indication that anyone had been at the cabin during the winter prior to or after the date of the occurrence.
Postmortem toxicological tests were positive for high levels of ethanol (alcohol), with 3 samples showing similar blood alcohol concentrations (BACs): Footnote 14 femoral BAC was 0.33 grams per decilitre (g/dl); vitreous BAC was 0.39 g/dl, and bile BAC was 0.35 g/dl. The average BAC of the 3 samples was 0.35 g/dl. The medical examiner reported the cause of death as attributable to multiple blunt injuries, and ethanol intoxication was thought to be a significant contributory factor in cause of death.
Tolerance to alcohol
Table 2 provides a summary of the typical effects of various blood alcohol levels on individual behaviour and performance.Footnote 15 There is a great deal of variability in actual effects, due to individual differences in tolerance.
Research specific to the task of piloting an aircraft has shown impaired performance in aircraft handling tasks at BACs as low as 0.01 g/dl. Other piloting tasks, including workload management, reaction time, and tasks requiring short-term memory, have been affected at BACs in the range of 0.03 to 0.05 g/dl, and the number and seriousness of errors committed by pilots increases with higher BAC. Given that these studies are conducted using familiar tasks in flight simulators, performance effects would likely be greater given an unfamiliar situation, such as an inflight emergency.Footnote 16
| BAC (g/dl) | Typical effects on behaviour and performance |
|---|---|
| 0.01-0.05 | average individual appears normal |
| 0.03-0.12 | mild euphoria, talkativeness, decreased inhibitions, decreased attention, impaired judgment, increased reaction time |
| 0.09-0.25 | emotional instability, loss of critical judgment, impairment of memory and comprehension, decreased sensory response, mild muscular incoordination |
| 0.18-0.30 | confusion, dizziness, exaggerated emotions (anger, fear, grief) impaired visual perception, decreased pain sensation, impaired balance, staggering gait, slurred speech, moderate muscular incoordination |
| 0.27-0.40 | apathy, impaired consciousness, stupor, significantly decreased response to stimulation, severe muscular incoordination, inability to stand or walk, vomiting, incontinence of urine and feces |
| 0.35-0.50 | unconsciousness, depressed or abolished reflexes, (abnormal body temperature, coma; possible death from respiratory paralysis (450 mg% or above) |
Tolerance is defined as: “a diminution of effectiveness after a period of continuous or large-dose administration of the drug” Footnote 17 and may be metabolic or functional. Metabolic tolerance results from an increased rate of metabolic processing of the drug and will result in lower BAC for the same amount of alcohol ingested. Functional tolerance refers to a reduced sensitivity of an organ or system to the drug such that more of the drug is required to produce an equivalent effect.Footnote 18
As noted above, a BAC above 0.3 g/dl is normally associated with severe lack of coordination and loss of consciousness. However, there have been many cases of drinking drivers found to have BACs in excess of 0.40 g/dl.Footnote 19,Footnote 20 Further, studies of alcoholics entering voluntary detoxification treatment have found that many individuals appeared normal in many aspects of behaviour including speech, gait, verbal comprehension, coordination, and ability to conduct tasks such as getting undressed, with BACs in excess of 0.30 g/dl.Footnote 21 Such BAC levels are believed to be common in individuals who abuse alcohol.Footnote 22
Increases in functional tolerance make it more difficult for others to detect alcohol intoxication or abuse, since the individual will show fewer physical or behavioural signs.Footnote 23
Transportation Safety Board Laboratory reports
The following TSB Laboratory reports were completed, and are available on request.
- LP042/2013 – Main Rotor Blade Root Examination
- LP039/2013 – ELT Examination and Testing
- LP038/2013 – Instrument and Lamp Analysis
- LP016/2013 – SkyTrac NVM Recovery
- LP043/2013 – Main Rotor Blade / Fuselage Paint Matching Analysis
- LP075/2013 – GPS Download, C-GOCM
Analysis
The investigation found nothing to indicate that any airframe failure or system malfunction that could have contributed to the in-flight breakup occurred before or during the flight. The helicopter was being operated within its weight and centre-of-gravity limits at the time of the accident. As well, the weather at the time of the accident was suitable for visual flight rules (VFR) flight. Therefore, the analysis will focus on several other factors: the in-flight breakup, the pilot's consumption of alcohol, and operational control within the company.
In-flight breakup
The pilot manipulated the flight controls in a manner that resulted in a main rotor blade contacting the right side of the cabin and leading to an in-flight breakup.
Alcohol use
On the day of the accident, many aspects of the pilot's flight planning, flying technique, and decision making were inconsistent with regulatory and administrative requirements, with the company operations manual, and with safe flying practices. These aspects included not filing a flight plan or flight itinerary, making unauthorized flights with an unauthorized passenger, exceeding allowed flight parameters, and consuming alcohol when piloting an aircraft. The quantity of ethanol in the pilot's system was over the limit of zero for piloting an aircraft, and over 4 times the legal limit for driving an automobile. This amount of alcohol was more than sufficient to cause major impairment of judgment and performance.
Flight following
The pilot was responsible for filing a flight plan or a flight itinerary, which was not done. Gemini Helicopters had systems and procedures in place to monitor flights and provide alerting services in the event of an accident or an overdue aircraft. These procedures could not be followed, as no itinerary was passed on to the flight follower or to any other responsible individual. As a result, the flight follower on duty was not aware of the flight, did not notice the email notification from the SkyTrac system, and did not bring up the satellite tracking notifications and position updates for C-GOCM.
There was no requirement within the company operations manual to track such flights. The flight follower was a new, low-time company pilot and was not properly trained in accordance with the company operations manual. These circumstances compromised any benefits that satellite tracking technology afforded.
As a result, when the accident occurred, no flight following was taking place, and the company was not aware that the helicopter was overdue.
Emergency locator transmitter
Although the emergency locator transmitter (ELT) appeared to have been installed in accordance with the manufacturer's instructions, the Velcro retention straps failed, and this may have contributed to the damage to the ELT's internal circuitry that resulted in it transmitting on an incorrect frequency.
The recently approved TSO–C126b states that Velcro-type fasteners no longer meet the requirements of newly manufactured or certified ELTs, and all future automatic fixed (AF) and automatic portable (AP) ELT approvals under that order must cover some other means of attachment. All existing installations that use the Velcro method of attachment may still be at risk of failure.
The lack of damage to the ELT case and the fact that the only circuit component that was damaged was the crystal oscillator strongly suggest that this ELT experienced impact forces less than 500 g. The failure of the crystal oscillator prevented the ELT from meeting the required performance standards, and as such, this oscillator may not be suitable for use in the AF/AP type of ELT.
Findings
Findings as to causes and contributing factors
- While piloting the helicopter under the influence of alcohol, the pilot made flight control inputs that caused the main rotor blade to contact the cabin and precipitate the in-flight breakup.
- If pilots do not adhere to company flight-following procedures, there is an increased risk of a company being unable to provide a timely response to an overdue aircraft.
- If an emergency locator transmitter fails to transmit a signal, this failure may significantly delay rescue, increasing the risk of serious injury or death.
- If emergency locator transmitters are attached to their mounting plates using Velcro, there is a risk of emergency locator transmitter failure due to impact damage.
Other findings
- Although information about the flights was available, it was not noticed by the flight follower.
- The emergency locator transmitter transmitted on an incorrect frequency due to an internal failure.
- The SkyTrac system in C-GOCM was instrumental in locating the accident site.
Safety action
Safety action taken
ACR Electronics
ACR Electronics, the manufacturer of the Artex emergency locator transmitter (ELT) model ME406HM, has produced a modified ELT mounting plate (part no. 8303.1), which is certified to TSO-C126b. The Velcro retaining straps have been replaced with metal, and these new backing plates can be used with previously certified ME406HM models certified under the previous technical standard order (TSO).
Gemini Helicopters Incorporated
Gemini Helicopters Inc. has made amendments to its company operations manual and its flight following procedures. It now has dedicated staff for the latter function. In addition, Gemini Helicopters has developed and implemented a daily flight risk-assessment document that is used by the operations and dispatch departments. The company has also put in place daily morning conference calls involving a member of the management team and all operations personnel to determine operational considerations for the day. This management team member authorizes each flight for every aircraft on a daily basis.
This report concludes the Transportation Safety Board's investigation into this occurrence. the Board authorized the release of this report on . It was officially released on .