In-flight engine fire leading to a forced landing
Piper PA-34-200, C-GNAS
Nadeau Air Service Inc.
Victoriaville, Quebec, 2 nm E
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Piper PA-34-200 (registration C-GNAS, serial number 34-7350133) departed from the Trois-Rivières Airport, Quebec, with 2 pilots on board for an instrument training flight. At 2100 feet, during a missed approach to the Victoriaville, Quebec, Airport, the right engine experienced a catastrophic failure and caught fire. At 1402 Eastern Daylight Time, the pilot in training declared an emergency due to the engine fire, and indicated his intention to land. During this time, dense smoke was spreading in the cockpit. The aircraft turned back and quickly descended in an attempt to land in a field located 2 nautical miles east of the Victoriaville Airport. The aircraft struck the ground and came to rest inverted. The 2 pilots were seriously injured. A bystander helped the occupants within minutes of the accident. The Victoriaville fire department arrived on the scene about 10 minutes later. The 406-MHz emergency locator transmitter activated on impact.
Factual information
History of the flight
The Piper PA-34-200 (registration C-GNAS,serial number 34-7350133) departed from the Trois-Rivières Airport, Quebec,with 2 pilots on board for an instrument training flight. The pilot in training (the pilot), who was occupying the left seat, was at the controls. The pilot was conducting an RNAV (GNSS)Footnote 1 RWY 06 approach to the Victoriaville Airport, Quebec; he pulled up after a missed approach in order to enter a holding pattern at the LESOS waypoint. At 1401:44,Footnote 2 while at 1600 feet and climbing to 4000 feet, the instructor called the air traffic control centre (ACC). About 1 minute later, at approximately 2100 feet, the right engine experienced a catastrophic failure, and flames engulfed the engine nacelle. Thick smoke quickly filled the cockpit. The instructor immediately took control and carried out the engine fire checklist procedure from memory. At 1402:45, the pilot declared an emergency and indicated that he wanted to land. The ACC alerted the Joint Rescue Coordination Centre (JRCC) and called the 911 dispatcher, who alerted the Victoriaville Fire Department and the Sûreté du Quebec. The ACC then tried unsuccessfully to communicate with the aircraft.
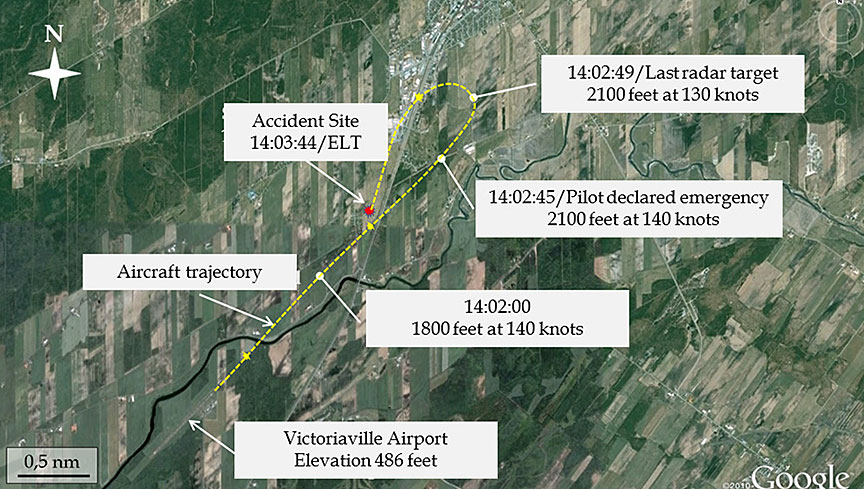
The PA-34-200 turned back toward the airport (Figure 1). The smoke cleared when the pilot opened his window and the instructor opened his door slightly. At the same time, flames from the right side of the aircraft appeared at the instructor's feet, setting fire to his trousers. The instructor immediately transferred control back to the pilot, urging him to make an emergency landing as he tried to smother the flames on his clothing with his hands. Smoke then filled the cabin again, making it difficult for the pilots to breathe and obstructing their view. The pilot decided to land straight ahead in a field. The instructor lost consciousness during the descent. The fire went out on its own. At the top of the trees, the pilot flared the aircraft for landing. The twin-engine aircraft struck the ground and bounced before stopping, inverted, some 435 feet later.
Meteorological information
There is no weather station in Victoriaville. The weather conditions were suitable for visual flight at the time of the accident. The Sherbrooke, Quebec, automated weather observation system, located 42 nautical miles (nm) from the accident site, reported southwest winds at 11 knots gusting to 19 knots, visibility of 9 statute miles (sm), and a ceiling of 3700 feet above ground level (agl). Based on the information obtained, the weather conditions in Victoriaville were similar. Weather is not considered to be a factor in this occurrence.
Personnel information
The instructor, who was the pilot-in-command, held a commercial pilot licence valid for single-engine and multi-engine aircraft, with a Class 1 instructor rating and an instrument rating. He had logged over 2000 hours of flight time, including about 105 hours on the PA-34-200 and 1300 hours as an instructor. The pilot held a valid private pilot licence, and was in the process of obtaining a commercial pilot licence (aeroplane) as well as multi-engine and instrument ratings. The pilot had logged almost 195 hours of flight time, including 15 hours on the PA-34-200.
Company information
At the time of the accident, Nadeau AirService Inc. conducted air taxi operations (under Subpart 703 of the Canadian Aviation Regulations [CARs]) and pilot training operations, using a fleet of 10 aircraft, including five Cessna 172s, three Cessna 150s, one Piper PA-34-200, and one PA-31-350.
Aircraft information
Built in 1973, C-GNAS was a twin-engine (Lycoming IO-360-C1E6) aircraft that had accumulated about 10 255 flight hours at the time of the accident. The aircraft was used by the Nadeau Air Service Inc. flight school mainly for instrument flight rules (IFR) training and flight training for twin-engine aircraft.
Heating, ventilation and defrost system
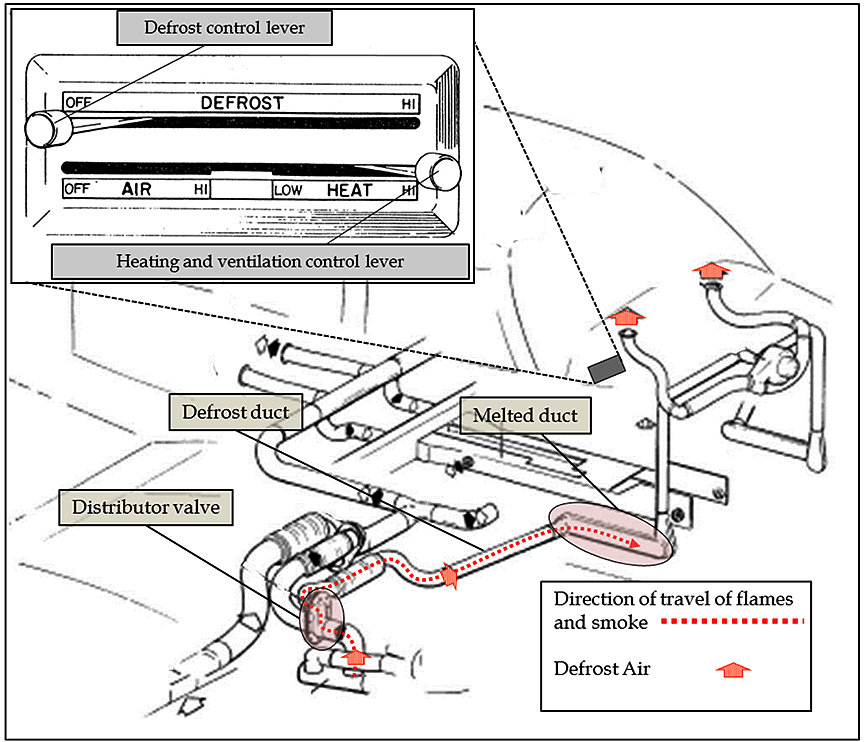
The outside air flows into a heat exchanger mounted on the exhaust manifold of each engine.This air is bled off to provide a source of hot air for the heating and defrost system. The air then flows from the heat exchanger to a distributor valve located in front of the engine firewall. The distributor valve is controlled by the heat and defrost setting switch on the right side of the instrument panel (Figure 2). The air flowing from the distributor valve for defrosting circulates in an independent system of ducts and conduits, and enters the cockpit through vents on either side of the windshield. The defrost lever controls the airflow by way of a cable,Footnote 3 activating a flap in the distributor valve.
The ventilation system is designed in such a way that the distributor valve prevents smoke from seeping into the cockpit and the cabin. Anomalies such as an engine oil leak can sometimes allow contaminants such as engine oil to seep into the ram air system. The pyrolysis of these contaminants can create smoke and odour in the supply lines for the heating and defrosting system.
Procedure for an in-flight engine fire
The PA-34-200 is not equipped with an engine fire warning or extinguishing system, nor is such a system required by regulation.
When crew members detect an engine fire,they are trained to follow the Engine Fire in Flight procedure (Figure 3).
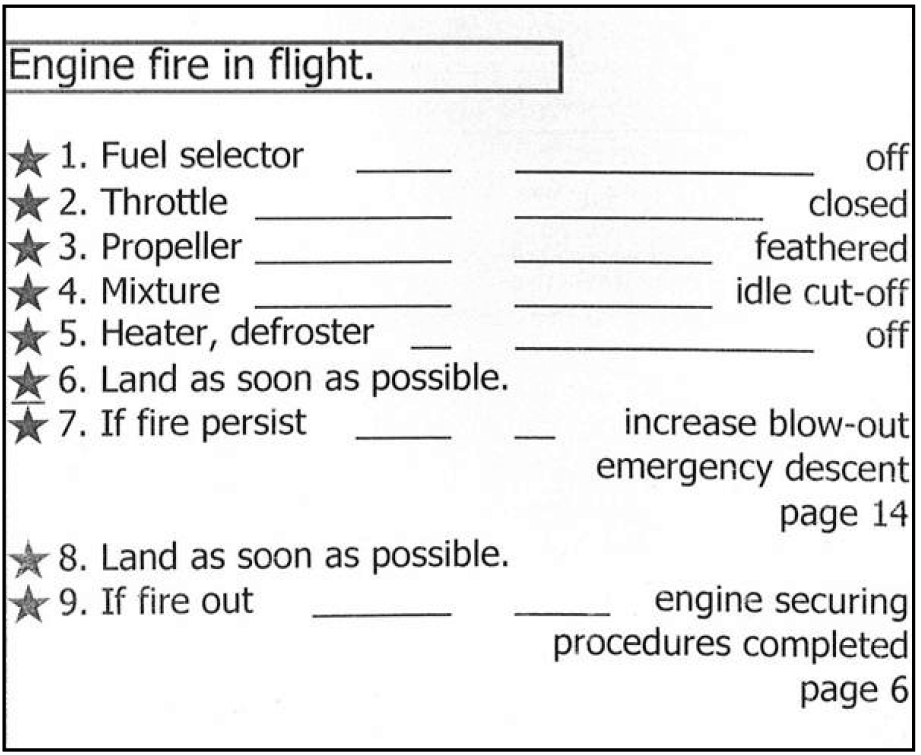
This procedure, which pilots must memorize, requires the pilot to immediately take certain actions. The first steps of the procedure are the following: turn off the fuel selector, close the throttle, feather the propeller, pull the mixture control to the idle/cut-off position, and close the heat/defrost air inlets. The purpose of these actions is to cut the flow of pressurized oil and fuel to the engine compartment to shut down and secure the affected engine. It also prevents fire and smoke from spreading into the cabin through the heater and defroster air ducts.
The propellers
The propeller of the affected engine must be feathered manually by pulling the propeller lever of the defective engine. The propellers are equipped with a lock that prevents feathering when engine speed is below 800 revolutions per minute (rpm). Consequently, if a propeller requires feathering, its lever must be brought back to the rear stop detent before engine speed drops below 800 rpm.
Aircraft inspection and maintenance records
At the time of the accident, Nadeau AirService Inc. had contracted all of its aircraft maintenance to Nadeau Mécanique Aviation Inc., an approved maintenance organization (AMO). Nadeau Air Service Inc. was the AMO's primary customer.
The engines were maintained on condition in accordance with Airworthiness Notice B041, edition 3, dated 18 December 1997. This airworthiness notice should have been replaced by edition 4, dated 31 March 2005, under the company's quality assurance program, in order to keep the engine maintenance schedule and inspection criteria up to date.
The aircraft was last inspected on 27 September 2012.Footnote 4 The phase I periodic inspectionFootnote 5 was performed in accordance with the maintenance schedule approved by Transport Canada (TC). The aircraft's journey log contained no mention of an anomaly in the right engine. Information obtained during the investigation indicated that a non-metallic deposit had been observed in the engine oil filter. The maintenance manager had decided to examine the filter after 10 hours of flight.
Based on the inspection sheets, it was also found that the technician who inspected the heating, ventilation, and defrost system did not find any anomaly. However, the investigation determined that Piper's recommended system-check procedure had not been followed; during the inspection, the positions of the control levers and the flaps on the distributor valve were not checked.
Documentation of anomalies
The maintenance records of C-GNAS indicate that the aircraft was not maintained in accordance with the CARs. An examination of the aircraft's journey log and work orders revealed that anomalies were not systematically recorded. Anomalies were reported verbally to maintenance personnel. The maintenance manager recorded the anomalies in the aircraft's journey log after corrective action was taken. More specifically, the disabling of the autopilot, the erratic operation of the global positioning system (GPS), and the oil leak spotted on the right engine cowl during the flight before the accident were not recorded in the aircraft's journey log as required by the CARs.Footnote 6 The last anomaly recorded by the flight crew in the journey log was on 14 December 2006.
Right engine maintenance history
On 10 October 2009, the aircraft engines and propellers were damaged after the nose gear collapsed during a landing. Following the accident, both engines were overhauled by Aéro Performance Moteur Inc.Footnote 7,Footnote 8 Several engine components were replaced, and the crankcases were sent to Divco Inc.Footnote 9 for a non-destructive inspection.
Divco Inc. weld-repaired 3 cracks on the crankcase on the outside of the No. 2 cylinder of the right engine. Lycoming does not recommend repairs of critical areas by any third party, because proper welding is difficult. The crankcase repairs were partially documented; documents detailing the size of the defects, their locations, and the amount of material removed were destroyed after 2 years. As well, the Transportation Safety Board (TSB) was not provided with proprietary information about the repair methods and materials; for that reason, it was impossible to determine whether the repairs were made in accordance with Federal Aviation Administration (FAA) Advisory Circular (AC) 33-6: Weld Repair of Aluminium Crankcases.Footnote 10
The cylinder studs and through-bolts were taken apart and reassembled by Divco. There is no mention of their condition in the description of the work.Footnote 11 Lycoming's mandatory service bulletin, Mandatory Parts Replacement at Overhaul and During Repair or Maintenance (No.240W), does not require maintenance on studs and through-bolts.
On 10 November 2010,Footnote 12 the right engine No. 2 cylinder was replaced following an excessive engine speed decrease during the magneto check.
On 11 September 2012,Footnote 13 after a phase I inspection of the aircraft, a broken stud had to be replaced onthe No. 1 cylinder.
On 12 October 2012, during the flight that preceded the accident flight, the pilot of C-GNAS noticed an oil slick on the inboard side of the right engine cowl. The crew reduced engine power and landed without additional incident. The pilot told the company's maintenance manager about the incident. The valve cover assemblies were tightened, the engine cowls were cleaned, and the oil level was checked. There was no ground run or maintenance flight after the check. The maintenance manager decided to check the engine after the next flight. Neither the oil leak nor the remedial measures were recorded in the aircraft's journey log.
Wreckage and impact information
Accident site
C-GNAS made a forced landing in a field, 1.8 nm from the edge of Runway 06 and 700 feet to the left of the extended runway centreline. The nose of the aircraft struck the ground heavily, on a heading of approximately 213° magnetic (°M), in a left-bank attitude. The first point of impact was 435 feet from the wreckage. The aircraft bounced and became airborne for about 200 feet before striking the ground and overturning. The aircraft came to a stop on its back about 235 feet further on.
At the first point of impact, the left propeller left 4 marks in the ground over a distance of 7 feet. Extensive debris was scattered on both sides of the break-up trajectory.
Examination of the wreckage
The aircraft came to rest perpendicular to the impact trajectory. The left wing was partially severed from the fuselage and connected to the wreckage by electrical wires and flight control cables. The nose of the aircraft disintegrated during the impact sequence. The right wing was attachedto the fuselage. An examination of the flight controls revealed no indication of malfunction prior to the crash. The landing gear had been extended at the time of impact and was torn off. The flaps were retracted.
The right engine was separated from the wing. The No. 2 cylinder was torn off and rested 10 feet from the wreckage. Piston No. 2 was not found. The engine fairings were scattered across the accident site.
The engine controls were in full forward position, except for the left engine throttle, which was pulled back slightly. Neither of the 2 propellers had been feathered. Both propellers were at afine-pitch angle. The left fuel selector valve was ON, and the right fuel selector valve was OFF. (It should be noted, however, that the positions of the levers may have shifted during the crash sequence.) All of the circuit breakers were engaged. The fire extinguisher was still in its bracket between the 2 pilot seats. Although its safety pin was no longer in place, the extinguisher had not been used. The seats, seatbelts, and shoulder harnesses were intact.
After on-site examination, the wreckage was taken to the TSB Laboratory in Ottawa for further examination.
Examination of the engines
The 2 engines were examined to determine the serviceability of the left engine and the reason for the right engine's failure.
Left engine
The damage to the left engine was typical foran engine running at the time of impact. No pre-existing defect was found.
Right engine
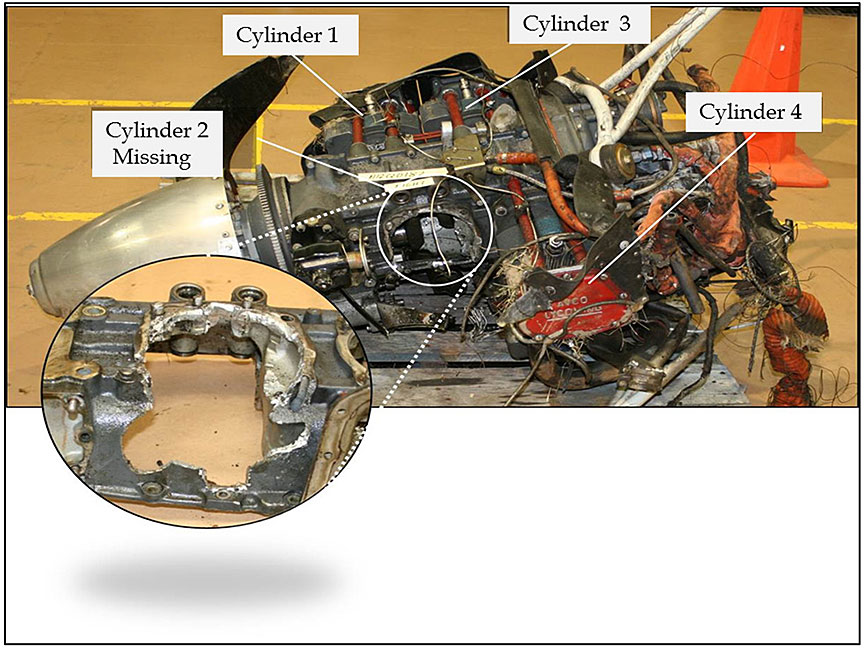
The No. 2 cylinder had separated from the engine. The part of the crankcase connected to the No. 2 cylinder was missing, as were studs 3, 7, and 8 (Figure 4). The remaining No. 2 cylinder studs were broken. The broken parts of the studs were missing, as were their bolts.
Preload is the tension created in the bolt by the application of torque during installation. In the present case, the nuts used to install the cylinders on the crankcase were plain nuts. Such nuts rely solely on the friction forces at the thread and joint surfaces to prevent the loss of preload due to vibration in service.Footnote 14
Among other things, examination of the engine revealed the following:
- The backoff torque for the nos. 1, 3, and 4 cylinders holddown nuts was normal.Footnote 15
- All of the recoveredFootnote 16 studs of the No. 2 cylinder had failed due to fatigue cracks.
- The studs exhibited no manufacturing defect, and the stud material complied with Lycoming's specifications.
- Fretting was observed on the surfaces where the crankcase and the No. 2 cylinder meet.
- The right engine airframe fuel filter was heavily contaminated.
- There was no indication of detonation or hydraulic locking in the No. 2 cylinder's combustion chamber.
The metallurgical examination of the right engine components revealed defects associated with the crankcase weld repair.The following anomalies were observed:
- There was a fatigue crack inthe No. 2 through-bolt hole of the No. 2 cylinder. The crack began in a welded area on the surface of the crankcase.
- A porosity that exceeded Lycoming's acceptance limit was found on the contact surface of the right crankcase near the No. 2 through-bolt.
- The crankcase hardness was either at or just below the minimum limit of Lycoming's hardness requirements. The measure of hardness of the repaired areas was less than that of the unrepaired areas. The repaired areas of the crankcases were susceptible to fatigue because they were softer.Footnote 17
- There was no indication of detonation or hydraulic locking in the No. 2 cylinder's combustion chamber.
Alerts issued to the aviation industry regarding weld-repaired crankcases
The FAA and the Australian Civil AviationSafety Authority (CASA) have issued alerts regarding problems associated with Lycoming horizontally-opposed engine crankcases that have been weld-repaired around or near the crankcase cylinder. The purpose is to alert operators and maintenance workers to the problems observed and to provide recommendations toward detection of potential catastrophic engine failures.
As well, in May 1989, the FAA published an alertFootnote 18 that documents problems associated with weld-repaired crankcases. The document relates 2 events in which the separation of a cylinder from the crankcase caused the engine to stall after fatigue cracks appeared at or near the stud holes. The alert recommends checking cylinder studs and bolts.
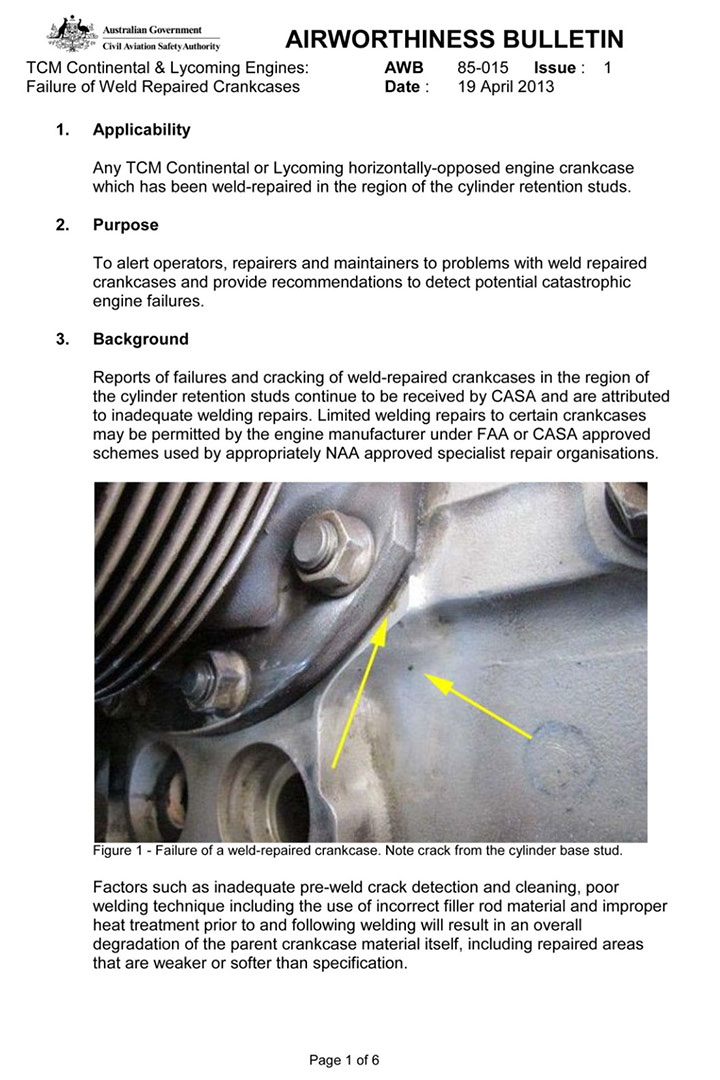
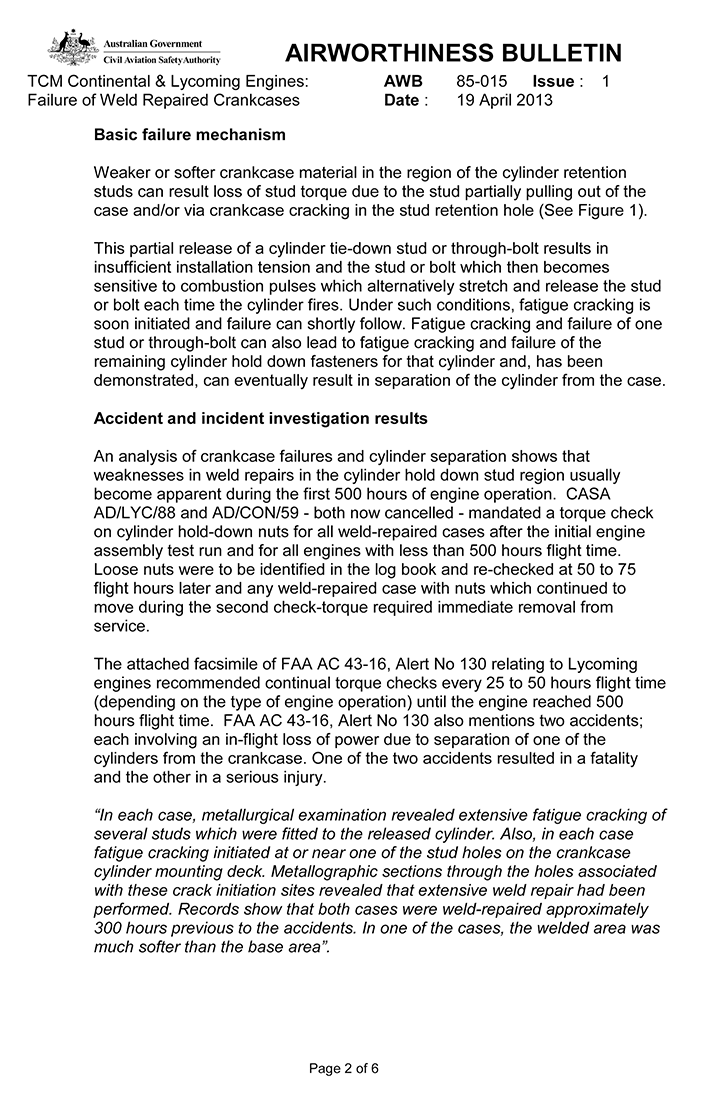
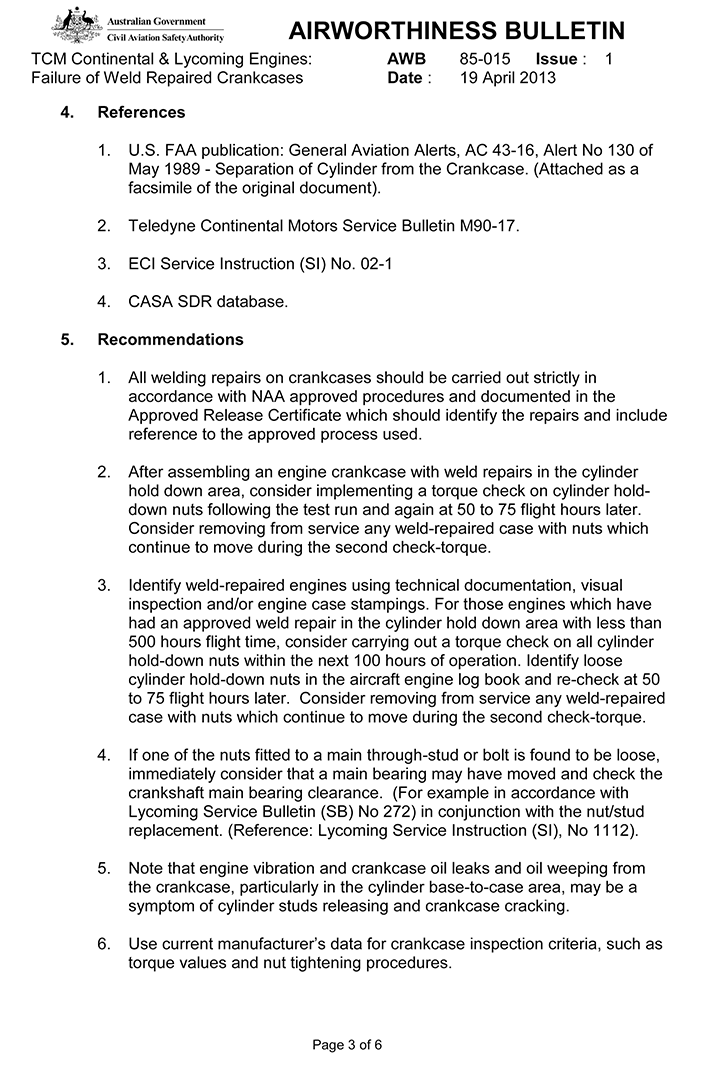
On 19 April 2013, the CASA issued Airworthiness Bulletin (AWB) 85-015 (Appendix A)Footnote 19 after receiving reports of failures and cracks near cylinder studs and through-boltsof weld-repaired crankcases. The bulletin makes 6 recommendations regarding repair methods, documentation of repairs, post-repair maintenance checks, and symptoms of a problem.
Damage caused by the engine fire
The damage caused by the engine fire to the cockpit, defrost/heating system, and engine nacelle was examined.
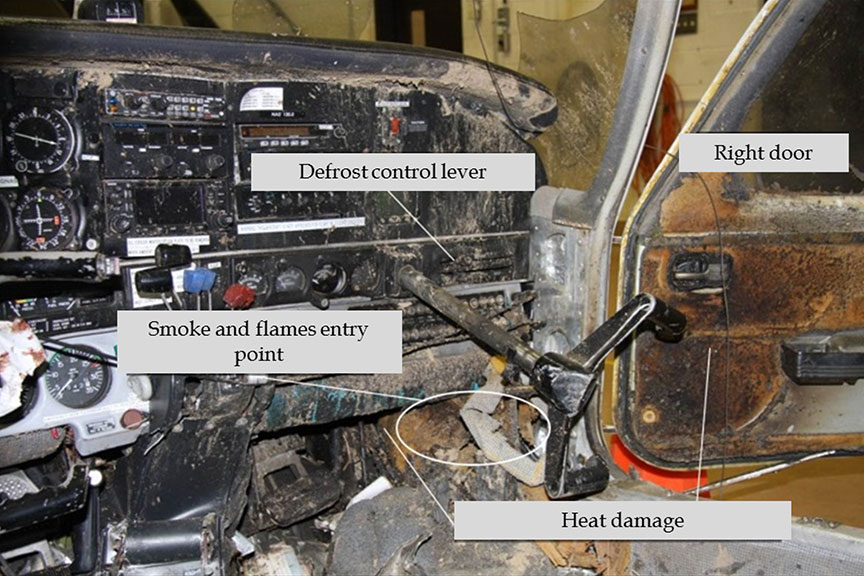
The damage to the cockpit indicates that the fire was concentrated in the space at the instructor's feet (right side),in the front portion of the right door and behind the instrument panel (Figure 5). The fire did not burn through the aircraft skin at any place along the fuselage. There were varying degrees of soot accumulation on the interior surface of some of the elements in the area of the fire. The fire was partially fuelled by flight documents in a pocket located on the right fuselage wall, at the pilot's feet. The insulation blanket that was located where the defrost air conduit turns at a right angle toward the top suffered the most damage due to the heat; the thermoplastic conduit had almost entirely melted. Part of theinsulation blanket installed directly against the right door skin was charred.
Examination of the ventilation system
In order to document and determine the trajectory of the smoke and fire, the aircraft's ventilation system was sent to the TSB Laboratory for examination. The heat and defrost levers were found to be positioned slightly to the right of the OFF position, and were freely moveable.
The components of the heating system did not reveal anything unusual: there was no soot accumulation in the ducts, the flaps were closed, and the control cables were connected to the flap.
However, the defrost system revealed the following anomalies:
- The right and left control cables connected to the control lever were not attached to their flaps.
- The right control cable duct had a tight bend at the junction of the wing and engine nacelle, and the sliding cable had a tight bend near the control lever, which impeded its movement and that of the flap.
- The end of the sliding cable of the right control cable was completely covered in soot.
- The flaps were open.Footnote 20
- The pattern of the soot on the right flap indicated that the flap was open during the engine fire.
- There was a considerable amount of soot on the inside face of the right defrost ducts.
- The fibreglass fairing of the distributor valve was almost entirely destroyed by the fire.
- The right defrost vent in the cockpit was partially blocked by adhesive tape.
TSB Laboratory reports
The following TSB Laboratory reports were completed, and are available from the TSB upon request:
- LP214/2012 – iPhone Analysis Project SummaryFootnote 21
- LP227/2012 – Engine and Propeller Examination
- LP228/2012 – Fire Examination
Analysis
Following an instrument approach to the Victoriaville Airport, Quebec, the right engine failed, and a fire erupted in the engine nacelle while the pilot was conducting a missed approach. The No. 2 cylinder sustained a catastrophic failure, allowing pressurized engine oil to spray into the engine compartment. The engine oil then caught fire, probably when it came into contact with the exhaust system. The smoke and flames then entered the cockpit, obstructing the pilots' vision and causing severe burns to the instructor.
Right engine failure
The engine failure was caused by the separation of the No. 2 cylinder after its tightening studs broke due to fatigue. All of the other damage to the right engine components occurred after the cylinder separated.
Incorrect preload has been identified as a leading cause of fatigue failure of engineering fasteners. A reduction in the preload will cause an increase of the load excursions experienced by the fastener. If the reduction in preload is sufficiently severe, the cyclic stress experienced by the fastener may exceed its endurance limit, leading to fatigue failure.
Incorrect preload can occur due to insufficient application of torque during installation and/or to self-loosening in service. Self-loosening of fasteners is commonly caused by vibration, but flexing of joint members, transverse slip, thermal cycles, and other factors can also cause a joint to loosen.
The fatigue failure of the No. 2 cylinder studs probably occurred as a result of insufficient preload in at least one stud. However, it was not possible to determine whether this insuffiency was caused by improper torque application during assembly or to loosening in service. Since some mounting studs were not recovered, it was not possible to determine the sequence of No. 2 cylinder stud failures.
The crankcase contained a fatigue crack inthe No. 2 stud hole. This crack extended from the welding area to the surface of the case. The metallurgical examination showed that the repaired parts of the crankcase were softer than specified by the manufacturer and contained welding defects, which made them more susceptible to fatigue. The fatigue crackin the No. 2 stud hole and the porosity of the contact surface could have contributed to release of the torque of the No. 2 through-stud. In such a case, therelease of torque, which reduced the stud preload, eventually resulted in a fatigue crack in the stud and caused it to break.
Divco Inc. was unable to provide all of the information required by Federal Aviation Administration (FAA) Advisory Circular (AC) 33-6 to be able to track the repair history. Therefore, the actions designed to ensure effective quality control cannot be evaluated. Divco's controlprocess is such that it was impossible to detect anomalies after the right engine crankcase was repaired.Footnote 22
The repaired area contained defects that exceeded the manufacturer's standardsFootnote 23 and led to the formation of a fatigue crack in the crankcase. It is possible that the crankcase repair and poor quality control processes increased the risk of engine failure.
Although the Australian Civil Aviation Safety Authority (CASA), the FAA, and Lycoming are aware of the risks associated with weld-repairing crankcases, FAA-approved shops can perform such repairs. The risk of engine failure also increases because a torque check isnot required when periodic inspections are performed. Consequently, if an aircraft is equipped with weld-repaired crankcases, there is an increased risk of engine failure.
During the flight that preceded the accident, the pilots noticed an oil slick in the right engine inboard cowl. However, neither the anomaly nor the maintenance work in this regard was noted in the aircraft's journey log. It is not known whether the oil leak came from a crackin the crankcase or from the base of the No. 2 cylinder. Due to its proximity to the event and its location, it is conceivable that the oil leak occurred before the No. 2 cylinder separated.Footnote 24 After cleaning the engine, the maintenance manager decided to check the engine after the next flight. However, it may have been prudent to determine the source of the oil leak prior to returning the aircraft to service.
Handling of the emergency
Given that the engine compartments of the PA-34-200 are not equipped with a fire extinguishing system, the fire fuelled by the engine oil could not be controlled. Once the oil burned off, the flames went out.Footnote 25 By taking the steps on the emergency checklist, the fuel supply to the engine was cut off, thereby limiting the intensity of the fire and protecting the cabin from the combustion products and flames. The flames and the smoke entered the cockpit even though the instructor moved the defrost and heating levers to the OFF position.
Movement of the smoke and fire from the right side to the cockpit
The soot accumulation found in the ventilation system indicates that the smoke and flames entered the cabin through the ducts and conduits of the defrost system on the right side. The smoke spread through the cabin through the vents at first, then through the hole created by the flames in the right side of the cabin, at the instructor's feet.
Significant anomalies were observed in the defrost system. Examination of the system revealed that the 2 control cables were disconnected from the flaps on the right and left distributor valves, and that the flaps were open. As well, the tight bend in the right control cable prevented the flexible cable from moving in the duct and shifting the flap. The fact that the left flap was open while the defrost control lever was in the OFF position may indicate that the cable was detached before the engine fire occurred. However, this cannot be confirmed. The cable may have detached from the flap on impact after the aircraft sustained structural damage.
The possibility that the right control cable became detached from the flap during the impact sequence was eliminated because of the soot accumulation that completely coated the flexible cable in the engine compartment. If the cable had become detached after impact, no soot would have been found where it was attached to the flap. Moreover, the pattern of the soot on the flap indicates that it was open during the fire. As a result, although the pilot moved the defrost control lever to the OFF position as soon as the engine failed, the smoke and flames generated by the oil fire were able to circulate through the ducts and conduits of the defrost system and enter the cockpit.
Maintenance and testing of the heating, ventilation and defrost system
It was impossible to determine conclusively when the anomalies observed on the right control cable occurred. However, the heating, ventilation and defrost system was not checked according to the aircraft manufacturer's recommended procedure during the last inspection (i.e., 9 flight hours before the accident). The inspection, as it was conducted, did not determine whether the system was operating properly, since the positions of the control lever and the flap were not checked.
Although it is considered a major emergency, an engine fire can almost always be brought under control by following the recommended procedure. In such a situation, proper operation of the systems required to carry out the emergency procedure is critical to the flight being able to continue. Maintenance personnel must perform the maintenance work in accordance with established procedures.
The malfunction of the defrost system made matters worse, creating an extreme emergency that required the aircraft to land immediately in a field. Conditions in the cockpit deteriorated very quickly.The flames and smoke affected the 2 pilots immediately. Besides a deterioration in visibility in the cockpit, the carbon monoxide in the smoke was on the way to triggering hypoxia in the crew and rendering them unable to perform their tasks. The instructor had to hand over control of the aircraft in order to put out the fire on his trousers, and did lose consciousness very shortly thereafter. During this time, the pilot, who was at the controls, had trouble breathing and discerning the landing area. The aircraft struck the ground because the smoke affected the pilot's ability to see outside, making it difficult for him to distinguish objects with the clarity required to land successfully.
Although the instructor carried out the engine fire checklist procedure and pulled on the propeller lever all the way to the feather position, the right propeller was not in the feathered position at the time of impact.Footnote 26 The catastrophic failure of the No. 2 cylinder caused the engine speed to quickly drop below the feathering limit, and the emergency procedure was rendered ineffectiveFootnote 27
Documentation of anomalies
The documentation suggests that C-GNAS was maintained in accordance with existing regulations. However, defects were not always recorded in the aircraft journey log. For example, the work done on the aircraft after the oil leak was spotted on the right engine during the flight before the accident was not recorded in the journey log, contrary to regulatory requirements. A lack of rigour in documenting anomalies and maintenance work makes it impossible to determine the exact condition or airworthiness of the aircraft before flight.
If anomalies are not systematically recorded in the aircraft's journey log, there is a risk that crews will not have information critical to the safety of the flight.
Findings
Findings as to causes and contributing factors
- Separation of the right engine No. 2 cylinder assembly resulted from the fatigue failure of the cylinder holddown studs, causing the right engine to fail.
- The fatigue of the cylinder holddown studs was a result of cyclic stresses caused by a loss of preload whose origin could not be determined conclusively.
- The repaired area of the right engine contained defects that exceeded the manufacturer's standards and would have been more susceptible to the formation of a fatigue crack in the crankcase.
- The catastrophic failure of the No. 2 cylinder released pressurized engine oil, which sprayed into the engine compartment and then caught fire on contact with the exhaust system.
- The flap on the right distributor valve was open, and the cable connecting the defrost lever was disconnected. It was therefore impossible to prevent the ram air in the engine compartment from flowing through the defrost system and into the cockpit.
- The smoke and flames entered the cabin by circulating through the ducts and conduits of the defrost system on the right side, requiring a forced landing in a field.
- As a result of the flames and smoke in the cockpit, the instructor lost consciousness, and the pilot had trouble discerning objects outside.
- The examination of the heating, ventilation and defrost system during the last inspection of the aircraft was not performed according to the procedures recommended by the aircraft manufacturer. Consequently, it was impossible for the inspection to ascertain whether the system was operating properly.
Findings as to risk
- Although the risks associated with weld-repaired crankcases are documented, Federal Aviation Administration-approved shops can perform such repairs. If an aircraft is equipped with weld-repaired crankcases, there continues to be a risk of engine failure.
- If anomalies are not recorded in the aircraft’s journey log, there is a risk that crews will not have information critical to the safety of the flight.
- If crankcase repair and overhaul companies do not maintain information needed to track repair history, there is a risk that actions designed to ensure effective quality control cannot be evaluated.
Other findings
- The crankcase contained a pre-existing fatigue crack at the through-stud No. 2 hole. This fatigue crack had initiated from a weld zone at the surface of the crankcase. An internal weld crack had served as one of the fatigue origins.
- The origin of the oil leak reported during the flight preceding the engine failure was not determined before the aircraft was put back into service.
This report concludes the Transportation Safety Board's investigation into this occurrence. The Board authorized the release of this report on . It was first released on .
Correction
The report has been amended as a result of new, more detailed information concerning the separation of the right engine No. 2 cylinder assembly that the Transportation Safety Board received after the report's initial release.
In the Factual information section, the fourth sentence of the second paragraph under the heading Right engine maintenance history refers to the FAA requirement that records describing the repair need to be maintained for only 2 years.
In the Analysis section, the sentence “Since some mounting studs were not recovered, it was not possible to determine the sequence of No. 2 cylinder stud failures” has been added to the fourth paragraph under the heading Right engine failure. The fifth paragraph has been modified, and the original sixth and seventh paragraphs have been deleted. The new sixth paragraph describes the FAA requirement for maintaining repair records.
The first 3 findings as to causes and contributing factors have been amended to reflect the new information concerning the right engine failure.
The reference to FAA AC 33-6 has been removed from the third finding as to risk.
Other finding number 1 has been added to describe the pre-existing fatigue crack at the thru-stud No. 2 hole.
This correction was approved by the Board on and the corrected version of the report was released on .
Appendices
Appendix A – Australian Civil Aviation Safety Authority Airworthiness Bulletin 85-015