Engine Problem - Collision with Terrain
Aéropro (2550-4330 Québec Inc.)
Beechcraft A100 King Air C-FGIN
Québec, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
On 23 June 2010, the Beechcraft A100 King Air (registration C-FGIN, serial number B-164) operated by Aéropro (2550-4330 Québec Inc.) as flight APO201 was making an instrument flight rules flight from Québec to Sept-Îles, Quebec. At 0557 Eastern Daylight Time, the crew started its take-off run on Runway 30 at the Québec/Jean Lesage International Airport; 68 seconds later, the co-pilot informed the airport controller that there was a problem with the right engine and that they would be returning to land on Runway 30. Shortly thereafter, the co-pilot requested aircraft rescue and fire-fighting (ARFF) services and informed the tower that the aircraft could no longer climb. A few seconds later, the aircraft struck the ground 1.5 nautical miles from the end of Runway 30. The aircraft continued its travel for 115 feet before striking a berm. The aircraft broke up and caught fire, coming to rest on its back 58 feet further on. The 2 crew members and 5 passengers died in the accident. No signal was received from the emergency locator transmitter (ELT).
1.0 Factual Information
1.1 History of the Flight
On the day of the accident, the 2 pilots arrived at the company's offices at Québec City/Jean Lesage International Airport around 0500.Footnote 1 The pilot-in-command (PIC) and co-pilot divided up the pre-flight tasks. The PIC obtained weather information from the NAV CANADA website and did the weight and balance calculation. At 0538 the PIC filed a flight plan with the Québec Flight Information Centre. Take-off was scheduled for 0600 from Québec to Sept-Îles and Natashquan, Quebec. The co-pilot performed the external inspection of the aircraft and added 1 litre of oil to the right engine.
At 0543, the 5 passengers boarded the aircraft. The PIC was seated in the left seat and was the pilot flying (PF). The co-pilot was seated in the right seat and was the pilot not flying (PNF). The engines were started using the ground power unit at 0545. The aircraft was then positioned for run-up and systems check.
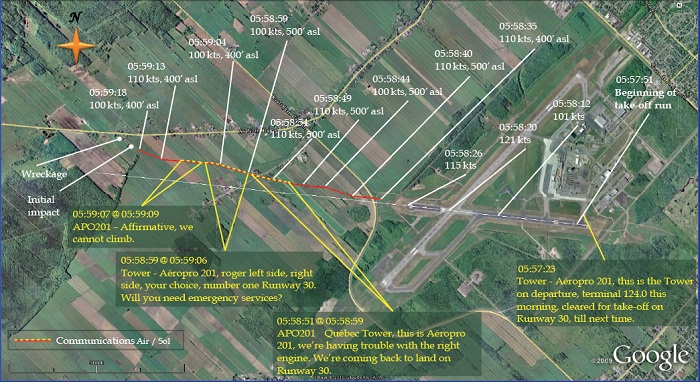
At 0554, APO201 proceeded onto Taxiway Charlie toward Runway 30 for take-off. Approximately 2 minutes later, the controller instructed APO201 to contact the terminal after lift-off and cleared the flight for take-off. In the seconds that followed, the aircraft began its take-off run with flaps retracted. At 0558, passing Taxiway Juliet (2900 feet from the runway threshold), APO201 rotated at 100 knots.Footnote 2 Directly over the Runway 06/24 intersection, the ground speed of the aircraft was 121 knots, the maximum speed reached during the flight. Approximately 6 seconds later, over the end of Runway 30, the ground speed dropped to 115 knots.
APO201 appeared on the Québec radar approximately 800 feet past the end of the runway, 160 feet above ground level (agl)Footnote 3 at 110 knots (Figure 1). Five seconds later, the aircraft turned 10° to the right; it was at 260 feet agl, the maximum altitude reached during the flight; its speed was unchanged. A few seconds later, the co-pilot informed the airport controller that there was a problem with the right engine and they would return and land on Runway 30. The controller immediately informed APO201 that it had priority to land and asked whether emergency services would be needed.Footnote 4 The co-pilot stated that the aircraft was unable to climb. This was the last transmission from APO201.
Nine seconds later, the aircraft disappeared from radar at 160 feet agl travelling at 100 knots. Ten seconds after the last transmission, APO201 crashed in a field. The aircraft travelled for 115 feet before hitting a berm. The aircraft broke up and caught fire coming to rest on its back 58 feet further.
The impact site was approximately 1.5 nautical miles (nm) from the end of Runway 30 and slightly to the right of the extended centreline. At 0614, approximately 15 minutes after the crash, vehicles from the Québec fire department arrived at the site and began fighting the intense fire. The fire was brought under control at 0630. All of the occupants remained inside the aircraft. The 2 pilots and 5 passengers died in the accident.
1.2 Injuries to Persons
|
Crew |
Passengers |
Others |
Total |
|---|---|---|---|---|
Fatal |
2 |
5 |
0 |
7 |
Serious |
0 |
0 |
0 |
0 |
Minor/None |
0 |
0 |
0 |
0 |
Total |
2 |
5 |
0 |
7 |
1.3 Damage to the Aircraft
Much of the aircraft was destroyed by the fire rendering a complete examination of the aircraft impossible. Only the engines, propellers and a few external tail components were recognizable.
1.4 Other Damage
Slightly less than 2600 pounds (388 US gallons) of Jet-A1 fuel was spilled, enabling a fire to start after the aircraft struck the berm. The fire destroyed the aircraft and burned approximately 4000 square feet of grass and several trees. The soil was extensively contaminated by residual material from the plastic and rubber components that melted after combustion.
1.5 Personnel Information
|
Pilot-in-command | Co-pilot |
|---|---|---|
Licence |
Airline pilot | Commercial pilot |
Medical expiry date |
01 September 2010 | 01 April 2011 |
Total flying hours |
3046 | 2335 |
Flying hours on Beechcraft King Air |
1677Footnote 5 | 455 |
Flying hours last 90 days |
144 | 128 |
Flying hours on type last 90 days |
118 | 121 |
Hours off duty prior to work |
13 | 12 |
1.5.1 Pilot-in-Command
The PIC was certified and qualified for flight in accordance with existing regulations and held a valid airline transport pilot licence.
The PIC worked as a flight instructor from August 2004 to February 2006. In March 2006, he was hired by a company based in Alberta. That month, he took ground and flight training on the King Air B200, and then passed a pilot proficiency check (PPC).Footnote 6 In October 2007 and after passing a PPC, he was promoted to PIC on the Beechcraft A100 aircraft. In December 2007, he obtained his PIC rating on the Beechcraft B200. In DePPCcember 2009, he took Crew Resource Management (CRM) training. The PIC's last flight for the Alberta-based company was on 20 April 2010. He was known to be a skilful pilot, to have good judgement and to scrupulously follow standard operating procedures (SOPs).
The PIC was hired by Aéropro in May 2010. He took ground and flight training from 3 to 12 May in accordance with the training program specified in the Aéropro operations manual. The ground training was delivered by the occurrence co-pilot.Footnote 7 The PIC did 5 hours of in-flight training on a Beechcraft A100 King Air with a company-designated pilot instructor. On 13 May, he passed an initial PPC to act as PIC for both single and multi-crew flights on the Beechcraft A100 King Air. The PPC was conducted by a designated approved check pilot (ACP).Footnote 8
Aéropro was required to track flight and duty times and rest periods for all of its pilots. To this end, pilots must record and update company records. The company's record of the PIC's flight and duty time could not be found. According to the PIC's personal logbook and the aircraft's journey log the PIC's work schedule met the requirements pertaining to flight and duty time limitations and rest periods.
Before the occurrence, the PIC flew with the co-pilot twice, on 27 May and 8 June 2010. Over these 2 days, they logged 16.6 flying hours on 9 flights. The PIC had made 15 flights on the occurrence aircraft in June 2010, on 1, 21 and 22 June 2010.
1.5.2 Co-pilot
The co-pilot was certified and qualified for flight in accordance with existing regulations and held a valid commercial pilot licence. He worked as a flight instructor for various operators from 2002 to 2007. In July 2006, he was hired by the Centre de formation aéronautique de Québec (CFAQ) as an instructor.Footnote 9 In 2007, he became the chief flight instructor at Sasair Inc. That same year, he taught theory and technical courses for Aéropro and Sasair.
In September 2007, the co-pilot completed a 24-hour theory course on the Beechcraft A100 King Air, taught by the chief pilot at Aéropro. Between 7 and 16 February 2008, he did 4.3 hours of training flights on a company Beechcraft A100 King Air with the chief pilot and a company-designated flight instructor. The training covered emergencies and other items, including engine failure at take-off. On 5 May 2008, the co-pilot passed an initial PPC as a co-pilot on a Beechcraft A100 King Air, which was renewed on 10 June 2009. On 19 June 2010, as part of his PPC renewal,Footnote 10 he made 2 training flights on the Beechcraft A100 King Air with the company's chief pilot. The co-pilot did not receive CRM training and was not required to take it.
The company's record of the co-pilot's flight and flight duty time could not be found. The co‑pilot's personal logbook and the journey log of the aircraft were used to determine his work schedule. According to these documents, the co-pilot met the requirements pertaining to flight and duty time limitations and rest periods.
1.6 Aircraft Information
|
|
|---|---|
Manufacturer |
Beechcraft |
Type and model |
A100 King Air |
Year of manufacture |
1974 |
Serial number |
B-164 |
Certificate of airworthiness |
Valid |
Number of airframe hours / Number of airframe cycles |
19 665 hours / 16 800 cycles |
Engines |
Pratt & Whitney Canada, PT6A-28 (2) |
Maximum allowable take-off weight |
11 500 pounds |
Recommended fuel types |
Jet-A1, Jet-A, Jet-B |
Fuel type used |
Jet-A1 (confirmed in laboratory) |
1.6.1 General
The Beechcraft King Air is a pressurized twin-engine turboprop aircraft manufactured by Beechcraft. Over 6600 have been manufactured and have accumulated more than 10& million flight hours in private, commercial and military operation around the world. C–FGIN was configured to carry 2 crew members and up to 9 passengers.
1.6.2 Aircraft Weight and Balance
The aircraft journey log, flight plan, and weight and balance report were found in the wreckage. The weight and balance report confirmed the positions of the 5 passengers on board: 2 passengers in Row 2, 2 in Row 3, and 1 in Row 4. The aircraft was carrying 2600 pounds (388 US gallons) of fuel in the main tanks. The take-off weight of the aircraft was 11 123 pounds and the centre of gravity was at 186.9 inches, which is within the allowed weight and balance limits.
1.6.3 Review of Aircraft Maintenance Records
1.6.3.1 General
Maintenance records show that C-FGIN was certified, equipped, and maintained in accordance with existing regulations and approved procedures.
On 16 April 2010, Aéropro's approved maintenance organization (AMO) conducted a routine Phase 3 inspectionFootnote 11 of C-FGIN in accordance with the Transport Canada (TC)-approved maintenance program. At the time of the inspection, the aircraft had logged a total of 19 510 hours 45 minutes of flight time. Approximately 380 elements were to be checked during the inspection, which included a ground test of engine performance and the operation of various systems. There is no indication that any deficiencies were observed during these tests. On the day of the occurrence, the aircraft had 32 hours 15 minutes of flight time remaining before the next scheduled inspection.
1.6.3.2 Recording of Defects
Examination of the aircraft journey logs and work orders revealed that work was often done on C-FGIN without the defects being recorded in the journey log. The investigation revealed that pilots often reported aircraft defects orally to maintenance personnel or in writing on a piece of paper and did not record them in the journey log as required by the Canadian Aviation Regulations (CARs),Footnote 12the Maintenance Control Manual (MCM),Footnote 13 and the Aéropro SOPs. After receiving an oral report of defects from the pilots, maintenance personnel would write them down on a piece of paper and prepare work orders later. The investigation was unable to find any of these notes. Corrective measures were taken when parts became available and the entries were added to the aircraft journey log later on. The CARs requirements for recording defects are indicated in the reference note in the MCM, which states that at the end of a flight, any defects observed must be recorded in the aircraft journey log by a member of the flight crew.
The company SOPs contain the following instructions in Subsection 2.21, “Mechanical Failure”:
SOP Subsection Mechanical Failure 2.21.1 To reduce delays in the event of a mechanical failure, you must contact Maintenance immediately. 2.21.2 It is very important that all defects be recorded in the log book.
1.6.3.3 Autopilot Inoperative
On 19 February 2009, the C-FGIN autopilot was reported inoperative on a work order, but no mention of this appeared in the aircraft journey log defect description box. To make sure flight crews did not use the autopilot, its associated circuit breaker was pulled and a crew information sheet placed on the control panel. The defect was then recorded in the journey log deferral items box as a 120-day deferred item in accordance with the Aéropro Minimum Equipment List (MEL) for the Beechcraft A100 King Air. According to the MEL, the autopilot should have been returned to service on 30 May 2009. It was still inoperative on the day of the occurrence which was not in compliance with Aéropro's MEL requirement. However, the autopilot was not required since the flight was conducted by 2 crew members.
1.6.3.4 Work on the Left Engine
From 2 June to 7 June 2010, Aéropro maintenance personnel performed routine maintenance on the left engine (PT6A-28). The compressor turbine wheel was replaced at the end of its service life, a routine hot section inspection was performed, and the injection nozzles were replaced in accordance with the schedule prescribed by the company and the engine manufacturer. A powerFootnote 14 test was then done on both engines at 1400 ft-lb of torque, following the procedures set out in the aircraft maintenance manual (AMM).Footnote 15 The results showed no problems with engine performance.
1.6.3.5 Repairs to Propeller De-icers
On Friday 18 June 2010, an apprentice mechanic received instructions to perform a series of tasks over the weekend. On C-FGIN, he was to replace the right propeller de-icer, check the system, and, if necessary, replace the de-icer wiring harnesses on both propellers. The mechanic documented the work performed on 20 June 2010 on a work order in accordance with company procedure. The apprentice mechanic did not have the authority to certify the work done on the aircraft. The spinners and engine access panels remained removed for inspection by a certified technician. The work on C-FGIN was completed on 21 June 2010; however, there was no mention in the aircraft journey log of the work being done before the aircraft was returned to service. On 21 and 22 June 2010, C-FGIN made 4 flights with no problems. It was only after the aircraft had returned from the flights that the defect, the repairs and the aircraft certification were entered in the aircraft documentation. The MCM states that maintenance personnel must ensure that documents are completed and that the aircraft is duly certified for flight before being returned to service. This maintenance work was not documented in accordance with the company MCM.
1.6.3.6 Engine Condition Trend Monitoring Program
Aéropro used an engine condition trend monitoring (ECTM) program recommended by the engine manufacturer, Pratt & Whitney Canada. Implementing an ECTM program provides information about engine parameter trends and can help extend the service life of engine components. The pilots do a reading of the engine parameters once established at cruising altitude. The reading is done on the first flight of the day and the parameters are recorded in the aircraft journey log. An analysis of the parameters for the month preceding the accident, as entered in the aircraft journey log, showed no deterioration in engine performance. The program is not intended to confirm the engine control rigging and cannot confirm the maximum power available or used on take-off.
1.6.4 Beechcraft A100 King Aircraft Flight Manual
The FAA-approved aircraft flight manual (AFM) for the Beechcraft A100 King Air sets out the aircraft operating limits and procedures that must be followed.
According to the AFM, the allowable engine power at take-off is limited by the following parameters: 1628 ft-lb of torque, ITTFootnote 16 of 750°C, or gas generator (N1) at 101.5% for a maximum of 5 minutes. The Beechcraft A100 King Air AFM does not indicate or prescribe any procedure for take-off with reduced power.Footnote 17 It also does not provide a separate set of limits and performance data for take-offs with reduced power.
Section 4 of the AFM, entitled Performance, provides the performance data required to determine the minimum power (torque) value at which take-off performance can be obtained. A crew must refer to chart 4.11 to determine the minimum take-off power required for the actual take-off conditions. According to the chart titled Minimum Take-Off Power at 2200 rpm, and 66 knots indicated airspeed (IAS), for the occurrence flight, a minimum of 1585 ft‑lb was required to obtain the published performance figures. Power above 1585 ft-lb may be used up to the torque or ITT engine limitations.
In an emergency situation, the maximum continuous power is the same as the maximum allowable take-off power, which is 1628 ft-lb. It is intended to be used in an emergency at the pilot's discretion.
Certain speed limits and operating limits are indicated on the aircraft airspeed indicators by coloured lines and bands. The minimum control speed (Vmc)Footnote 18 is indicated by a red line at 85 knots. The best rate of climb with one engine inoperative (Vyse) is indicated by a blue line at 120 knots.
Because the rotation speed (Vr)Footnote 19 varies depending on the aircraft weight and configuration on take-off and the runway conditions, this measurement is not shown on the airspeed indicator. The crew must consult the appropriate take-off performance chart to determine the appropriate Vr. Aéropro set a Vr of 100 knots, which is 1 knot over the lift-off speed for the maximum gross take-off weight of the aircraft indicated in the AFM. The speed corresponding to the maximum rate of climb with 2 engines is 119 knots.
The stall speed (Vs) also varies depending on the aircraft weight and configuration. The C-FGIN stall speeds with and without engines were 64 and 88 knots, respectively. The chart entitled Stall Speed cannot be used to calculate Vs with one engine inoperative. According to the manufacturer, the single-engine Vs of a twin-engine aircraft is slightly lower than the Vs with no engines.
1.6.5 Normal, Abnormal and Emergency Procedures
1.6.5.1 General
The aircraft operating procedures are published in the AFM. Because the Beechcraft A100 King Air is certified for IFR flight with a single pilot, the manufacturer developed the procedures so that they could be performed by only one pilot. The AFM does not indicate any memory items in the emergency procedures.
In accordance with CAR 703.107, Aéropro developed and updated SOPs for its aircraft operated by 2 pilots. The SOPs enabled the crew members to operate the aircraft within the limits specified in the AFM. The SOPs outline company rules and procedures, aircraft operating procedures and the use of checklists. TC had reviewed Aéropro's SOPs and found them to be in conformity with CAR 703.107. However, SOPs for 703 operations are not subject to in-depth review of content and are not subject to approval by TC. This also applies to checklists.
One purpose of SOPs is to improve coordination among crew members. To this end, SOPs normally assign each task listed in the normal and emergency procedures, specifying which tasks are to be performed by the PF or the PNF.
Aéropro prepared checklists for the Beechcraft A100 King Air: one for operating under normal situations (CHKL) and one for abnormal and emergency situations (ECHKL). The company checklists indicate the SOP items that are considered important to flight safety. The ECHKL is used at the PF's request and is read by the PNF. Abnormal or emergency procedures are generally performed by reading them, then carrying them out. However, some urgent situations require immediate action that the pilots must have memorized. There were no memory items in the emergency procedures described in the AFM, but Aéropro took the initiative of identifying memory items in its ECHKL. These actions could be carried out by either the PF or the PNF, and were shown in red on the checklists and preceded by an asterisk in the SOPs.
The Aéropro SOPs recognized the importance of good coordination among crew members. The SOPs stated that crew member coordination measures for abnormal and emergency situations were discussed in the chapter on these procedures. Each task in a normal procedure was assigned to one of the 2 pilots depending on the pilot's responsibilities or role. However, the task distribution for each pilot was not specified in the section on Beechcraft A100 King Air emergency procedures, and the emergency procedures in the SOPs did not mention any standard calls.
1.6.5.2 Normal Procedures
Normal procedures are intended for checking aircraft system operation and making sure that the aircraft configuration is appropriate for the planned or current phase of flight.
There were some minor differences between the AFM and the CHKL with regard to pre-take-off checks: namely, the order of some task checks was changed. These differences were not a factor in the occurrence.
There was a notable difference between the feathering system check in the AFM and the check in the CHKL and the SOPs. The AFM required both the automatic and manual feathering systems to be checked, whereas the CHKL required only the autofeathersystem to be checked. The CHKL may have been prepared without bearing in mind that some of the company's Beechcraft A100 King Airs, such as C-FGIN, were not equipped with an autofeather system.
SOPs subsection 2.16 “Company Limitations”, which outlined the limits set by the company, differed considerably from the AFM with regard to engine power limits. Aéropro limited engine power as follows:
- Take-off: 1500 ft-lb or 700°C and 2200 rpm
- Climb: 1500 ft-lb or 700°C and 2000 rpm
- Level flight or descent: 1400 ft-lb or 700°C and 1900 rpm
- All company parameters must be adhered to at all times, except in an emergency.
In this regard, the company issued 2 memos restating the operational limits of the engines as indicated in the SOPs. The first memo, issued by the chief pilot and the operations director on 25 May 2007, stated that the parameters set by Pratt & Whitney Canada were based on a time between overhauls (TBOs) of 3600 hours. On the most recent hot section inspections and when the engines were overhauled, costs were abnormally high because some of the engines were not operated as directed by the manufacturer. The memo required compliance with the directive, with penalties for non-compliance. The second memo, issued by the chief pilot and dated 21 December 2007, reminded pilots that adhering to these limits was imperative in order to avoid incurring additional costs on engine overhauls. Neither memo mentioned that the limits set by the company did not apply in an emergency situation.
According to the SOPs, the crew must review normal and abnormal take-off procedures, standard instrument departure (SID) if applicable or the first flight segment, and review emergency procedures for an engine failure, on the first flight of the day. An example follows in the form of a table from the SOP:
PNF |
PF |
|---|---|
|
Standard take-off Runway 30 |
|
V1 and Vr at 100 knots |
Anything unusual before V1/ Vr? |
Reject take-off. |
After V1/ Vr? |
Continue take-off. |
|
SID or first segment? |
Heading 295, climb 660', left turn heading 274, climb 4000' |
|
|
Questions? |
1.6.5.3 Emergency Procedures
In this occurrence,
- the engine problem occurred less than 30 seconds after take-off;
- the co-pilot reported a problem with the right engine;
- the gear warning tone sounded indicating that the crew had pulled back the power lever on one engine (Section 1.8.3, Analysis of Communications from APO201);
- the right engine was producing little or no power at the time of the crash (Section 1.11.6, Examination of the Engines).
Taking into account the observations listed above, the procedures for engine problems or requiring a reduction in engine power published in the AFM, the SOPs and the ECHKL were considered by the investigation:
- Engine fire in-flight: examination of the wreckage ruled out the possibility of an in-flight fire.
- Oil and fuel leak: the engine examination revealed no oil and fuel leaks.
- Low oil pressure (below 40PSI): the engine investigation revealed no oil pump system malfunction and proper quantity of oil was found in the engine.
- Engine magnetic chip detector light on: Engine chip plug and oil filter were examined and found in good condition, the right chip detector light bulb analysis revealed that it was extinguished at the time of impact.
Two remaining procedures were considered:
- Engine failure (power loss) after take-off
- Flight low pitch stop system malfunction.
These are discussed in detail in the following paragraphs.
1.6.5.4 Procedure for Engine Failure After Take-off
The procedure for engine failure after take-off was designed so that all critical actions were performed sequentially, in order of priority. For an engine failure after take-off, the SOPs reproduced the AFM emergency procedure titled Engine Failure During Takeoff, as well as a diagram showing the flight profile of the aircraft and the tasks to be performed by the crew, but it does not specify who performs which tasks. The ECHKL requires the first nine items on the following list, which pilots must have memorized, to be performed immediately:
ENGINE FAILURE AFTER LIFT-OFF
- Power - MAXIMUM ALLOWABLE
- Propeller - FULL INCREASE
- Airspeed - MAINTAIN speed at engine failure until obstacles are cleared. Reduce speed only if single engine BEST RATE OF CLIMB SPEED is exceeded.
- Landing Gear - UP
- Confirm Inoperative Engine
- Propeller (inoperative Engine) - FEATHERED
- Airspeed - BEST ANGLE OF CLIMB SPEED (after obstacles clearance altitude is reached)
- Flaps - UP
- Airspeed - BEST RATE OF CLIMB SPEED
- Clean – Up (Inoperative Engine):
- Condition lever - CUT OFF
- Bleed Air Valve - AS REQUIRED
- Auto Ignition - OFF
- Fuel firewall Valve - CLOSED
- Generator - OFF
- Fuel Control Heat - OFF
- Autofeather Switch - OFF
- Propeller Synchrophaser - OFF
- Electrical Load - MONITOR
NOTE: If the autofeather is being used, do not retard the failed engine power lever until the autofeather system has completely stopped propeller rotation. To do so will deactivate the autofeather circuit and prevent automatic feathering.
If an engine failure were to occur after take-off from Runway 30 at Québec Airport, performing the first 3 items on the list would provide maximum thrust and an optimal flight profile; the power levers would be pushed to produce maximum power, 1628 ft-lb; the propeller levers would be pushed fully forward; and the aircraft would accelerate to the best rate of climb speed (120 knots).Footnote 20 Performing items 4 to 9 would eliminate most drag and provide the maximum rate of climb. Because the aircraft was not equipped with an autofeather system, the propeller of the affected engine needed to be feathered manually by pulling the propeller lever for the failed engine. The last 2 items on the list are not essential and may be performed at the crew's discretion.
The instructions on the flight profile diagram for engine failures after take-off differ slightly from the ECHKL in their sequence and when they are to be performed (Figure 2). They recommend retracting the flaps and performing the ECHKL items at 400 feet above ground level (agl). According to the diagram, the non-essential items are to be performed and ATS is to be contacted at 1000 feet agl.
1.6.5.5 Flight Low Pitch Stop System
C-FGIN was equipped with a ground and a flight low pitch stop system. It is managed by the propeller controller, which controls the minimum pitch angle on the ground to approximately 10° and also prevents the propeller pitch from reversing on the ground. The flight low pitch stop system controls the minimum pitch angle for each propeller in flight, an angle of approximately 14° , and prevents propellers from reversing in flight. The flight low pitch stop system is activated when the aircraft weight is removed from both main landing gear at take-off.
The low pitch propeller position is determined by the flight low pitch stop which is an electrically monitored hydraulic stop type. The system works by receiving an electrical signal and opening a propeller control valve to release the fluid pressure to the propeller, allowing the propeller to move towards a higher pitch position. If the flight low pitch stop system malfunctions, a steady amber light on the annunciator panel illuminates to alert the crew (PROP LOW PITCH).
The propeller system is driven by 1 propeller governor and 1 overspeed governor that control the propeller rpm. The propeller governor controls the propeller through its entire range. The propeller control lever operates the propeller by means of its governor. If the propeller governor should malfunction and request more than 2200 rpm, the overspeed governor cuts in at 2288 rpm to keep the rpm from exceeding 2288 rpm.
The flight low pitch stop annunciator/warning system and the prop governor are protected by circuit breakers.
A low pitch stop system malfunction will cause the low pitch stop warning light to illuminate and cause one of the following conditions:
a. the propeller blade angle to increase (towards feather)
- engine torque increase
- propeller rpm decrease
- engine torque fluctuations
- propeller rpm fluctuations.
Both of these would be indicated to the crew by the change in engine noise and indicated torque accompanied by associated yaw.
When the flight low pitch stop annunciator/warning system breaker is not engaged, the crew will not be provided with the PROP LOW PITCH warning.
If one of the 2 propellers drops below the ground low pitch stop, its warning indicator illuminates to indicate that the system has been activated and is resolving the situation. If an electrical system failure in the flight low pitch stop system occurs when one of the 2 propellers unexpectedly begins feathering, the SOP prescribes the following procedure:
If either propeller unexpectedly begins feathering in flight: *Power Lever (affected side) - REDUCE AS REQUIRED (to keep torque within limits). *"PROP GOV-IDLE STOP" Circuit Breaker (co-pilot's right subpanel) – PULL. Propeller speed should increase to governor setting. *Power Lever (affected side) - RETURN TO DESIRED POWER
WARNING: Any malfunction of the Flight Low Pitch Stop system be repaired before the next flight.
The procedure for a low pitch stop failure is included in the section on emergency procedures in the AFM, Aéropro's SOPs and training material, but is not included on the ECHKL.
1.6.5.6 Performance Figures
The AFM includes take-off and climb performance data. The performance figures provided by manufacturers are obtained using airplanes that conform to what will become the type design. The data collected is then written in accordance with the certification standards and presented as the airplane flight manual's (AFM) performance information. The performance data presented in the AFM is conservative and reproducible by a pilot in an airplane operated and maintained in accordance with the type design.
Using the AFM performance graph 4.11, Minimum Take-Off Power at 2200 rpm at 66 knots, the crew must determine if the aircraft engines deliver the minimum power for the actual pressure altitude and outside air pressure. On the day of the occurrence C-FGIN had to deliver a power of 1585 ft-lb during the take-off roll at 66 knots indicated airspeed in order to meet the published take-off performance.
The crew had company SOPs not to exceed 1500 ft-lb. on takeoff. Therefore the crew was unable to obtain the minimum take-off power required on that day and to assess if the engines were capable of delivering the take-off power.
In this investigation the airplane was not being operated in accordance with the type design; i.e., the reduced-performance take-off, therefore no take-off performance information presented in the AFM was valid for the occurrence takeoff.
1.6.5.7 Take-off Distance
The take-off distance required for a rolling take-offFootnote 21 is almost the same as a take-off made following the criteria of the AFM chart entitled Take-Off Distance‑0% Flaps.Footnote 22 Given the weight of the aircraft at take-off and the conditions at the Québec Airport, the aircraft should have taken off after a take-off run of 2250 feet. The take-off run represents the length of the roll between the point where the aircraft is lined upFootnote 23 on the runway and where it reaches 100 knots, which is the rotation speed used by the company.
1.6.5.8 Aircraft Performance During the Take-off Run
According to the airport surface detection equipment (ASDE) data,Footnote 24 the aircraft reached the indicated speed of 100 knots after travelling nearly 2800 feet.
In order to evaluate the aircraft performance during the last take-off, TSB used the ASDE data to analyze 6 take-off runs made by C‑FGIN in the 23 days leading up to the occurrence. The analysis did not reveal any major differences among the take-off runs.
1.6.5.9 Single Engine Climb Rate According to the Aircraft Flight Manual
In order to predict the effect of temperature and altitude on single engine climb performance, the Beechcraft A100 King Air AFM, in Section 4, FAA Performance, includes a chart that can be used to determine the maximum rate of climb. The chart is based on the following conditions:
- maximum continuous power on the working engine;
- 0% flaps;
- landing gear retracted;
- the propeller of the inoperative engine being feathered; and
- climb speed of 118 knots.
According to the chart entitled Single Engine Climb,Footnote 25 the aircraft should have been able to climb at a vertical rate of 450 feet per minute on 1 engine with the other propeller feathered.
1.6.5.10 Rate-of-Climb Calculations Correlated with Observations of the Wreckage
The maximum rate of climb is the vertical rate that provides the most gain in altitude in the shortest amount of time. The rate of climb of an aircraft depends on the difference between the total thrust and the total drag. When the total thrust is higher than the total drag, the aircraft can climb at a constant or increasing rate. When the aircraft climbs at an angle greater than the extra available power allows, speed decreases.
The aircraft manufacturer prepared some performance calculations at the request of TSB. The object was to determine the vertical rate of the aircraft for different flight parameters, correlating the following information:
- observations of the wreckage (flaps and landing gear retracted);
- observations of the engines (right engine developing little or no power);
- observations of the propellers (right propeller at low pitch);
- the aircraft take-off weight (11 123 pounds);
- the weather conditions on the day of the occurrence (29.92 inches of mercury, 18°C, wind 0 kts); and
- the maximum altitude of the flight (260 ft agl).
When an engine fails on a twin-engine aircraft, the propeller of the failed engine generates significant drag if it is not feathered, and drag increases with the speed of the aircraft. As a result, the rate of climb increases with the reduction in aircraft speed in relation to Vyse. The results of the calculation of the rate of climb with the right engine inoperative and the propeller at low pitch are shown in the table below.
Table 1. Rate of climb – right engine inoperative and propeller at low pitch
| Left engine power (ft-lb) | Rate of climb in feet per minute / IAS | |||||
|
95 knots | 100 knots | 105 knots | 110 knots | 115 knots | 120 knots |
1400 |
-32.7 | -39.3 | -61.2 | -94.8 | -140.2 | -197.2 |
1450 |
5.8 | 0.4 | -20.5 | -53 | -97.3 | -153.2 |
1500 |
43.8 | 39.6 | 19.8 | -11.6 | -54.8 | -109.5 |
1550 |
81.3 | 78.4 | 59.7 | 29.4 | -12.6 | -66.2 |
1628 |
139 | 138.1 | 121.2 | 92.6 | 52.5 | 0.8 |
The thrust/drag coefficient for an idling engine/propeller is not available, and no test flights were done to determine the performance of the Beechcraft A100 King Air in such a configuration. The vertical rate of the aircraft was estimated using the power required for zero thrust.
The following table shows the estimated rate of climb with the right engine at zero thrust (idle power), the propeller at low pitch and the same parameters as for the inoperative engine.
Table 2. Rate of climb – right engine at idle power and propeller at low pitch
| Left engine power (ft-lb) | Rate of climb in feet per minute / IAS | |||||
|
95 knots | 100 knots | 105 knots | 110 knots | 115 knots | 120 knots |
1400 |
188 | 217.7 | 235.9 | 246.2 | 248.8 | 243.9 |
1450 |
226.6 | 257.6 | 276.8 | 288.2 | 291.8 | 288.1 |
1500 |
264.7 | 296.9 | 317.2 | 329.7 | 334.5 | 331.9 |
1550 |
302.4 | 335.9 | 357.3 | 370.9 | 376.9 | 375.5 |
1628 |
360.3 | 395.8 | 419 | 434.4 | 442.2 | 442.7 |
The PIC's training notes indicated that the take-off power was adjusted to 1400 ft‑lb. Consequently, Hawker Beechcraft Corporation calculated the rate of climb at 1400 ft-lb of engine torque for the left engine with the right propeller feathered.
Table 3. Rate of climb – with relation to aircraft weight
| Aircraft weight (lb) | Rate of climb in feet per minute | |||
|
110 knots | 115 knots | 120 knots | 125 knots |
11 000 |
313 | 321 | 323 | 317 |
11 500 |
236 | 146 | 250 | 247 |
According to Hawker Beechcraft's calculations, the aircraft would be capable of climbing at approximately 300 feet per minute if the propeller were feathered.
1.7 Meteorological Information
Because the aircraft took off at 0557, the 0500 ATISFootnote 26 was in effect when the aircraft took off from the Québec Airport. The weather was reported as follows:
- wind 90° M at 5 knots;
- visibility of 15 statute miles (sm);
- a few clouds at 9000 feet, overcast at 12 000 feet; and
- temperature of 19°C, dew point at 10°C, altimeter setting 29.92 inches of mercury.
The 0600 ATIS was broadcast at 0607, and the weather was reported as follows:
- wind 110°M at 5 knots;
- visibility 25 sm;
- overcast at 8500 feet; and
- temperature of 19°C, dew point at 12°C, altimeter setting 29.92 inches of mercury.
Because the wind was below 15 knots, the airport controller was not required to provide the pilot with the wind speed and direction when clearing the aircraft for take-off. Based on the ATIS information, the aircraft took off with a tailwind component of approximately 4 knots. The aircraft flight manual does not specify a limit to the tailwind component on take-off. The tailwind increases take-off distance and reduces climb performance after take-off. The weather was not considered a factor in this occurrence.
1.8 Telecommunications
1.8.1 Communications Between APO201 and Quebec Airport Control
All communications recorded by NAV CANADA between APO201 and Québec ATC were of good technical quality; that is, all of the recording equipment functioned normally and the sound quality was good. There is nothing to indicate that communications were misunderstood or not received by either ATC or APO201.
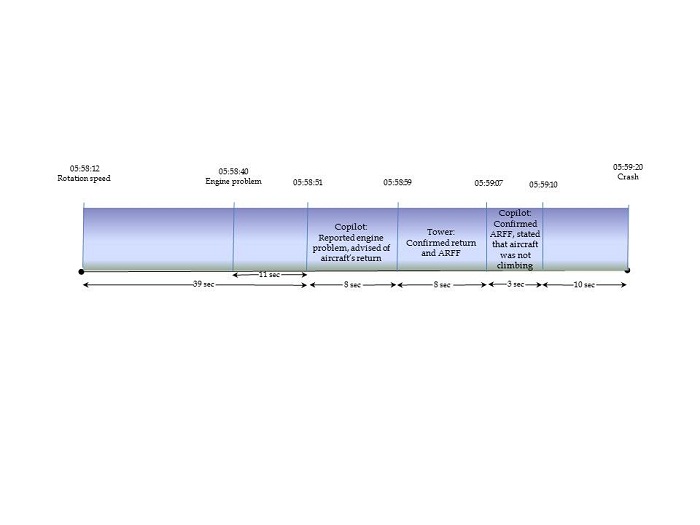
There were 3 radio communications between APO201 and the Québec tower after take-off (see Figure 3). They occurred after the engine problem, one after the other. All communications from APO201 were made by the co-pilot. They contained the distress call, navigation information, the dispatch of aircraft rescue and firefighting (ARFF) services, and the aircraft performance problems. The communications began 39 seconds after the aircraft reached rotation speed and occurred over a total period of 19 seconds. The aircraft crashed 21 seconds after the first call from APO201 and 10 seconds after the last communication.
When the co-pilot issued the distress call at 0558:51, the airport controller responded in accordance with NAV CANADA standards and practices. In the seconds that followed, the airport controller informed the Montreal ACC, then called the controller on break back to his post. Immediately after observing the explosion that followed the accident, the controller directed ARFF services to the crash site and called 911. These communications were clear, timely, and unambiguous.
1.8.2 Internal Communications
The communications between the pilots were not recorded because the aircraft was not equipped with a cockpit voice recorder (CVR). As a result, the investigation was unable to determine the nature of the communications between the crew members.
1.8.3 Analysis of Communications from APO201
The audio spectrum analysis of communications from APO201 revealed that an intermittent warning tone was sounding during the 2 calls from the co-pilot following take-off. It was also noted that no warning tone was recorded during APO201's previous transmissions. The warning tone recorded during the flight had a harmonic frequency similar to that of the gear warning tone.
The aircraft is equipped with only 1 intermittent audible alarm, which is intended to prevent a belly landing of the aircraft with the landing gear retracted. The alarm sounds when 1 or both power levers are pulled below a certain level of engine power and the landing gear is retracted.
1.9 Aerodrome Information
The Québec Airport has 2 runways: Runway 12/30, which is 5700 feet long and 150 feet wide, and Runway 06/24, which is 9000 feet long and 150 feet wide. The runways intersect 4300 feet from the threshold of Runway 30.
The elevation of the end of Runway 30 is 239 feet asl. Beyond the end of the runway, the ground slopes downward over 1 nm to approximately 230 feet asl, then gradually rises toward Mont Bélair, located approximately 3 nm from the end of the runway. A post-occurrence inspection of the runway did not reveal any deficiencies, debris or objects that could have been a factor in the occurrence.
1.10 Recorders
1.10.1 Flight Data Recorder
C-FGIN was not equipped with a flight data recorder (FDR), nor was it required by regulation.
1.10.2 Cockpit Voice Recorder
C-FGIN was not equipped with a cockpit voice recorder (CVR). According to the type certificate, the aircraft can be operated with only 1 pilot on board. The terms of its air operator certificate Footnote 27 did not authorize C-FGIN to be operated with only 1 pilot because it did not have all the equipment required by the CARs.Footnote 28 The autopilot had been inoperative since February 2009.
In 2003, an amendment to the CARsFootnote 29 pertaining to CVRs indicated that, subject to Section 605.34, no person shall conduct a take-off in a multi-engine turbine-powered aircraft that is configured for 6 or more passenger seats and for which 2 pilots are required by the aircraft type certificate, or by the subpart under which the aircraft is operated, unless the aircraft is equipped with a cockpit voice recorder. C-FGIN was configured with 9 passenger seats. According to the Canadian Civil Aircraft Register, there are 1635 multi-engine turbine-powered aircraft to which the CVR requirements apply. It could not be determined how many of these are not equipped with a CVR.
On 24 February 2004, TC sent enforcement letters to 3 air taxi operators in Quebec, including Aéropro, regarding the installation of CVRs in their Beechcraft 100 aircraft. TC gave them 30 days to submit a timetable for corrective action and installation of CVRs.
These operators disputed TC's interpretation of the requirement to install a CVR when the aircraft is operated under Subpart 703 with a 2-pilot flight crew in Federal Court. On 17 October 2005, the Federal Court of Appeal found in favour of the operators, ruling that they are not required to use a 2-pilot crew and that they can voluntarily, at their option, operate their Beechcraft 100s as commercial air taxis with 2 pilots instead of 1 without having to install CVRs in their aircraft. In its ruling, the Federal Court of Appeal ruled that this requirement does not apply to aircraft certified for operation by a single pilot and that it was erroneous to state that the CVR provisions applied to these operations.
As a result, in November 2009, TC developed a notice of proposed amendment (NPA) to the CARs. The aim of the NPA was to make it clear that a CVR is required at all times when this type of aircraft (configured with 6 or more passenger seats) is operated with 2 pilots. At mid‑2011, the CARs had not yet been amended.
Since 2009, 2 other accidentsFootnote 30 have occurred involving aircraft of similar type which were not equipped with a CVR and were operating as an air taxi service. These accidents resulted in 2 fatalities and 2 people with serious injuries. As with this investigation, the lack of a CVR adds to the complexity of these investigations and deprives the investigators of information that is essential to an understanding of how and why these accidents happened.
In this occurrence, the lack of a CVR made it impossible to clearly establish the activities of and communications between the 2 pilots as the occurrence unfolded. Consequently, it was not possible to identify potential safety deficiencies and to disseminate them within the industry to prevent similar occurrences in the future.
In 2010, the TSB published a WatchlistFootnote 31 describing the safety problems that represent the greatest risks to Canadians and which were investigated by the TSB. Concerning the safety problems identified, the TSB is of the view that information that is essential to an understanding of how and why transportation accidents happen is often lost or damaged, or collecting it is not mandatory.
1.10.3 Guardian Skytrax 3
30 April 2010. The system collects and transmits GPS flight dataFootnote 32 to the Guardian company server and to the air operator, making it possible to follow the movement of each aircraft on the ground and in the air, in almost real time. The system installed on C-FGIN consisted of an antenna and a data box installed in the nose of the aircraft. The Skytrax 3 can provide flight history, such as position, altitude, direction and speed, recorded to the second. The system is housed in a sturdy plastic enclosure. However, in this occurrence it was destroyed by fire and could not be retrieved for data analysis.
1.11 Wreckage and Impact Information
1.11.1 Accident Site
C-FGIN struck the ground approximately 1.5 nm past the end of Runway 30, 900 feet to the right of the extended centreline. Initial impact was made in a direction of approximately 320 magnetic, banking right. The right wingtip left a 5-foot-long furrow in the ground 173 feet before the wreckage (Figure 4).

The marks made by the left wing in a tree (BΔ) show that the aircraft was banking right at approximately 23°. About 92 feet further, there were marks made by the left propeller (C). The space between the first 3 marks made by the propeller is 0.8 feet. Analysis of these marks revealed that the aircraft was travelling at 69.7 knots, based on the assumption that the engine rpm was 2200 at that specific time. Approximately 23 feet further on, the left wing hit a berm (D), causing the fuselage to roll to the right. The right wing broke on the ground, the right engine (G) separated from the wing and the fuel tank was crushed. After point (C), where the left propeller struck the ground, the aircraft travelled just over 82 feet before coming to rest on its back (F). Much of the aircraft was destroyed by fire. The fire may have been caused by electrical arcing resulting from damaged electrical harnesses, the heat of the engines and possibly friction from the sheet metal coming into contact with the fuel.
1.11.2 Wreckage Distribution
The fuselage assembly was on its back. The left elevator (E) was separated from the empennage and lay some 62 feet to the right of the wreckage (F). An examination of the wreckage did not reveal any deficiencies, and the damage was consistent with the impact with the berm and the ground. The right engine and propeller (G) were approximately 26 feet in front of the wreckage along the crash trajectory of the crash.
1.11.3 Examination of the Wreckage
Examination of the wreckage determined that the landing gear was retracted and locked. The flap actuators indicated that the flaps were retracted. The stabilizer trim jackscrews were found in the neutral position, which is equivalent to 0° stabilizer trim indicator position. The aileron trim tab was found at 6° down and the rudder trim tab at 2° left. An examination of the flight controls revealed no indication of a malfunction prior to the crash.
The aircraft was equipped with 9 forward-facing passenger seats: 4 on the left and 5 on the right. The crew members' seatbelts were unbuckled, as were 5 of the passenger seatbelts; 2 passenger seatbelts were found buckled, and the remaining 2 belt buckles could not be found in the debris.
The locks on the main boarding door and the emergency exit were in the locked position.
1.11.4 Examination of the Annunciator Panel
The Beechcraft A100 King Air is equipped with an annunciator panel that alerts the crew to certain engine or aircraft system malfunctions. It is located in the glare shield of the instrument panel and consists of 24 different colour-coded warning lamps. When a malfunction occurs, the warning lamp for the defective system illuminates at maximum brightness. If the malfunction requires the crew's immediate attention, the main warning lamp, located just to the left of the annunciator panel, flashes red.
The annunciator panel and on-board instruments allow the crew to identify the affected system and determine the severity of the malfunction. Tactile and sensory cues are also obvious signs of a problem.
The C-FGIN annunciator panel was partly destroyed in the fire. The fractures and deformations of the panel warning lamp filaments were analyzed. The 4 lamps at the extreme right end of the panel were missing and the 4 to their immediate left were partly melted. A number of these lamps were involved in reporting the problem with the right engine and propeller; examination of the lamps did not yield any information.
Examination of the 16 other lampsFootnote 33 determined that they were all extinguished at the time of the crash.
1.11.5 Examination of the Propellers
Both propellers were manufactured by Hartzell Propeller Inc., model HC-B4TN-3A.Footnote 34 The left propeller was still attached to the engine and showed damage consistent with rotation at the time of impact with the ground. Laboratory examination of the propeller did not reveal any defects. The evidence gathered shows that the propeller was rotating and developing power at low pitch. However, the exact power could not be determined.
The right propeller was still attached to the engine and showed less rotation damage than the left propeller. Laboratory examination of the propeller did not reveal any malfunctions. The information gathered confirms that the propeller was rotating and indicates that it was developing little power compared to the left engine, and that the blades were in the low pitch range on impact. However, the exact power could not be determined.
1.11.6 Examination of the Engines
Examination of the PT6A-28 engines was performed at Pratt & Whitney Canada in the presence of TSB, NTSBFootnote 35 and FAAFootnote 36 investigators, as well as representatives from Aéropro and Transport Canada.

The left engine (serial number 50450) had a total of 18 656 hours and 16 000 cycles since new. It had logged 1498 hours and 1292 cycles since its last service, and 62 flying hours since overhaul on 6 June 2010.
Internal examination of the left engine revealed significant rub marks in the various areas of the engine made by the rotating components coming into contact with the engine housings. The engine air inlet strut was fractured from the impact and torsional overstresses. The evidence indicates that the engine was developing power at the time of impact (Photo 1).
The right engine (serial number 52411) had a total of 2037 hours and 2796 operating cycles since new. It had logged 797 hours and 672 cycles since its last service. According to the technical log books, it had been overhauled on 9 June 2009, after 1240 hours in service.

Internal examination of the right engine revealed that the turbine and compressor components showed very faint rub marks, indicating that the engine was developing power below engine idle speed or little power at impact (Photo 2).
The accessoriesFootnote 37 of both engines were examined. The fuel and control lines were intact, and the attachments were loose, which is normal when components have been exposed to extreme heat from a fire. The composite and plastic parts had melted, and any defects could not be identified. No defects were observed on the other mechanical components.
1.11.7 Examination of the Propulsion Control System
Propulsion is controlled using 3 sets of levers:
- Power levers on the left of the console, control the supply of fuel to control engine torque and thus the gas generator rotation speed. During take-off these levers would normally be advanced to the calculated power required for take-off. In-flight the levers are retarded to the climb or cruise setting as applicable. When the levers are pulled back and raised (below the idle positionFootnote 38), the propellers pitch reverses to assist the braking action during landing.
- Propeller levers in the middle of the console, are used to set the desired propeller rpm by adjusting the propeller governor. The governor then alters the propeller pitch to achieve the desired rpm, with regard to engine to torque and aerodynamic forces thus increasing or decreasing the propeller blade pitch. The normal propeller operating rpm range selectable by the pilots' movement of the propeller levers is 1800 rpm to 2200 rpm once the propeller is in a governing range. When the levers are brought back to the rear stop detent it activates propeller feathering.
- Condition levers on the right of the console, have three positions: fuel cutoff, low idle and high idle. They supply or cut off fuel and limit engine rotation speed to 60% for low idle and the high idle position provides from 70% up to take-off power.
Examination of the propulsion control system levers in the cockpit did not reveal any relevant information that could improve understanding of the accident. No defects were noted that could have prevented the engines from functioning normally.
1.11.8 Examination of the Flight Low Pitch Stop System
As the components on the left engine were destroyed in the fire, only the right engine flight low pitch stop system components were examined. The components did not show any mechanical defects. The system's electronic components, situated at the rear of each engine nacelle, were destroyed in the fire. The flight low pitch stop system operation could not be verified because of the condition of the electrical components after the fire.
A review of Service Difficulty Reports (SDR)Footnote 39 pertaining to the flight low pitch stop system showed mainly defects with mechanical components such as the levers, the carbon plates, the moving parts of the system, and the low pitch stop and proximity detectors.
Several Beechcraft A100 King Air operators have reported that the flight low pitch stop system requires frequent maintenance. The maintenance associated with this system has led many operators to replace the propellers, thus removing the system. A number of operators and pilots (including at Aéropro) have also reported making flights with the flight low pitch stop system warning light circuit breaker pulled.
Flight low pitch stop system operation must be tested before the first flight of each day, as indicated in the AFM. The aircraft must not be flown if the system is inoperative. A review of the aircraft log books did not reveal any defects related to the flight low pitch stop system in the past year. Even though the investigation revealed that it was a practice to pull the flight low pitch stop warning light circuit breaker, nothing indicated that the flight low pitch stop system controlling circuit breaker was pulled before take-off.
Deactivating the flight low pitch stop system by opening the controlling circuit breaker does not prevent the propeller governor from knowing were the mechanically monitored hydraulic low pitch stop is and properly commanding blade angles, although a finer blade angle than 14° can then be commanded in the air.
1.12 Medical Information
The occupants all survived the initial impact but were burned extensively. They all inhaled products of combustion, as indicated by the traces of soot in their airways. The damage to the fuselage and the major fire that erupted immediately after impact prevented the occupants from evacuating the aircraft. The investigation determined that there were no indications that the crew's performance was degraded by physiological factors.
1.13 Survival Aspects
A surveillance camera located at Gate 24 of the Québec Airport captured APO201 taking off starting at a point 1500 feet from the threshold of Runway 30. The poor quality of the video recording made it impossible to examine the aircraft in detail or follow its complete flight path. However, at 0559:22, an explosion could be seen after the aircraft crashed at the foot of Mont Bélair behind the stand of trees. No sign of fire or unusual lights were observed before the aircraft crashed.
The airport controller notified the Québec Airport ARFF services at 0559, one second after the co-pilot advised him of their intention to return to the airport. Fire department vehicles from Québec City arrived at the accident site at 0614 and started fighting the fire. They were joined by ARFF personnel about 1 minute later. The fire was extinguished at 0630.
All occupants were found in the cabin after the fire had been extinguished. All of their seatbelts were unbuckled. The PIC was lying near the main door at the left rear of the aircraft. The co‑pilot was found near the emergency exit door over the right wing. The doors were examined and found to be locked. The overturned cabin, the smoke and the extreme heat of the fire made survival impossible. It would have been difficult to move around inside the aircraft; the seats were hanging over the occupants' heads as the cabin quickly filled up with smoke and the heat became intolerable. Evacuation was not possible.
The accident produced g-force below human tolerance limits,Footnote 40 and the cabin was relatively intact immediately after it came to rest on its back. However, the accident was not considered survivable because of the intensity of the fire. The survival rate is lower in smaller aircraft after a post-impact fire.Footnote 41
1.14 Training Information
1.14.1 Pilot Training on the Beechcraft A100 King Air
Aéropro's pilot training program was approved by Transport Canada. Following a program validation inspection (PVI) in October 2009, the Transport Canada principal operations inspector monitored some ground school sessions.
1.14.1.1 Technical Ground Training
Aéropro's technical ground training program on the Beechcraft A100 King Air met CARs requirements. The program required pilots to receive instruction on the following:
- the aircraft systems;
- the differences in equipment, operation and layout between other aircraft of the same type in the fleet; and
- the appropriate standard operating procedures for the PF's and PNF's tasks for normal, abnormal, and emergency procedures.
Company records indicate that both pilots had received training on all required topics and had passed the evaluation tests for each training module. However, in contrast to the training program, the Beechcraft A100 King Air SOPs did not describe the specific tasks of the PF or the PNF for abnormal and emergency procedures.
1.14.1.2 Flight Training
Aéropro used only its own aircraft for flight training on the Beechcraft A100 King Air. It did not use a flight simulator for training, nor was this required by regulation. Some Beechcraft A100 King Air operators use a Beechcraft B200 King Air flight simulator because the 2 models have similar physical characteristics. The systems, engines and performances of the Beechcraft B200 King Air are different from those of the Beechcraft A100 King Air, but the simulator is used primarily to optimize multi-pilot crew performance in abnormal and emergency situations.
Flight training at Aéropro was usually done on an aircraft weighing considerably less than the maximum allowable take-off weight.Footnote 42 Various emergencies were simulated; at no time was the engine stopped in flight or the propeller feathered. The exercise was conducted at a minimum height of 400 feet agl, either on a take-off or approach. As a low pitch stop failure could not be re-created in flight, it was an item that was briefed by the instructor.
1.14.1.3 Pilot-in-command Training
The PIC had taken a full training course on the Beechcraft A100 King Air at another operator prior to employment with Aéropro. Although both companies used the same aircraft model, significant differences between the actual aircraft needed to be taken into account: namely, all of the other operator's aircraft were equipped with an autofeather system, whereas C-FGIN was not. The PIC had not done any flight training on C-FGIN. The engine failure procedures published in the SOPs of both companies also differed significantly. Unlike the other operator, Aéropro did not clearly define standard calls and the tasks of each pilot in abnormal and emergency situations.
During ground training at Aéropro, the PIC wrote the following procedure on his course notes:
[TRANSLATION] "Take-off, Departure, Emergency – first flight of the day.
Standard take-off Runway 30 – short runway -, power set to 1400 ft-lbs, flaps 0°, V1/Vr of 100 kts. SID/Visual take-off, runway heading, up to ____ ft , left/right turn…* [Any problem before V1/Vr reject, after V1/Vr take-off continues, in-flight emergency procedures. That will be max power, positive rate, gear up. I put my hand on the lever of the operative engine, you confirm and retard the lever, from left to right, then I confirm the firewall valve and close, at 400 ft flaps up, advise ATC – return and emergency checklist.] *Same briefing as earlier."
The PIC's flight training proceeded normally and was in accordance with current approved practices. He received PIC training for both single and multi-crew situations. As a single pilot, he was to perform all procedures himself, and when in command of a multi-pilot crew, he was to delegate tasks to the co-pilot in accordance with the SOP.
1.14.1.4 Co-pilot Training
The co-pilot's flight training involved acquiring the skills needed to control the aircraft from the right seat. This meant that, in an emergency situation, the co-pilot could be able to assume pilot flying tasks. There were no problems reported about his training. His last in-flight training on the Beechcraft A100 King Air took place in June 2009.
1.15 Information on the Operator and Management
1.15.1 General
Aéropro held operations certificates issued under Subparts 703 and 704 of the CARs. The occurrence aircraft was operated under Subpart 703.Footnote 43
In 2010, Aéropro's fleet consisted of 16 aircraft, including the Beechcraft King Air 100 and 90 models, Piper Pa-31, Embraer Emb110, and Metroliner SW2. Aéropro operated a shuttle and air taxi service with its main base at Québec and its secondary base at Sept-Îles.
1.15.2 Management
The company had the following management staff: President and Accountable Executive (AE), Operations Manager, Director of Maintenance, Chief Pilot 703 Operations, and Chief Pilot 704 Operations. Aéropro shared resources with Sasair, a related company.
TC created the position of AE in 2005Footnote 44 for all operators. The TC instructionsFootnote 45 read as follows:
The Accountable Executive (AE) is the agent for cultural change within an organisation; cultural change starts at the top. This key position is crucial to the success of the safety management system initiative and it is, therefore, very important to have the correct individual appointed at the outset. The regulation requires that the Accountable Executive have control, on behalf of the certificate holder, of the financial and human resources necessary for the operations or activities authorized under the certificate. In financial terms, this is not merely a matter of having control of a large budget but, rather, is directed at the level of the individual who authorizes that budget on behalf of the certificate holder. While the concept of "control" is not defined under the Aeronautics Act, if there is any uncertainty concerning the named executive simply asking the questions “Do they have the final decision?” and “Can they be overruled?” may assist. In general terms, if the appointed person is an employee and/or reports to anyone who can overrule them then that person is not at the correct level within the company to be the accountable executive.
The roles and responsibilities of management personnel indicated in the company operations manual included the following:
- The operations manager ensures the safety of air operations and has numerous responsibilities related to management, coordination and communication with the various internal and external elements of the company.
- The chief pilots are responsible for professional standards issues relating to the crews placed under their management. In their absence, tasks must be delegated to another qualified person in accordance with the CARs.
- The director of maintenance must possess the required qualifications and assume the responsibilities outlined in the company maintenance control manual (MCM).
- The company pilots report to the chief pilot and are required to ensure the safety of the flights they have been assigned.
- The flight followers track flights.
Aéropro's AE officially accepted the appointment and the responsibilities of the position in July 2005. This individual had his appointment as operations manager at Aéropro revoked by TC in June 2001 when TC found that he was unable to safely conduct operations.
1.15.3 Conditions of Employment for Pilots
The company employed about 20 pilots, most of whom were in their first years as commercial pilots. A number of them had been trained at Sasair before being hired by Aéropro. The Aéropro pilots belonged to a union to which they could report safety concerns. No safety concerns were reported to the union representative.
Pilot remuneration was based partly on the number of flight miles. Therefore flight assignment (flight hours) had a significant impact on a pilot' salary. At the beginning of employment, pilots were required to sign a company training bondFootnote 46 as a guarantee. Repayment of the bond was prorated over 12 months. Pilots who left the company before the end of 1 year were required to repay part of the training bond. This was a mutual agreement between the company and the pilot. Such financial arrangements were not unique to Aéropro.
According to the Safety of Air Taxi Operations Task Force (SATOPS) study,Footnote 47 remuneration based on miles or hours flown has a direct and negative impact on pilots' decision making. The SATOPS report recommends finding some means of requiring air operators to remunerate pilots in a way that eliminates the pressures associated with it.
1.15.4 Safety Management at Aéropro
In early 2010, TC informed industry of the February 2011 deadline for the mandatory implementation of Safety Management Systems (SMS) for 703 and 704 operations. Aéropro submitted a draft of Phase 1 of its SMS to TC in May 2010. TC responded that it would review the documents at a later date, because the regulations were not in force and the standards had not yet been set. TC encouraged Aéropro to continue promoting safety within the company. Since that time, TC has postponed the mandatory implementation of SMS indefinitely for 703 operations. As part of the initial SMS approach, Aéropro developed a safety policy, which was posted in several locations within the company, and held safety meetings with pilots. The policy, signed by the President and AE, stated that:
- Safety is a key company value.
- The company is committed to implementing an SMS, which is a proactive system for identifying and reducing hazards and risks.
- All managers and employees are accountable, starting with the President.
- The President is personally committed to making sure the policy is understood and implemented at all levels.
- All employees should have the tools and training to develop a safety culture.
- All employees are encouraged to report safety situations.
- No disciplinary action will be taken against employees who report hazards in accordance with the established criteria.
Whether or not an SMS was required, Aéropro was obliged to ensure compliance with the CARs and manage aviation safety in its 703 and 704 operations.
The SATOPS studyFootnote 48 listed the following safety management activities:
- occasional safety meetings;
- safety bulletins being posted;
- open communication between operating personnel and management;
- open discussion of problems experienced in day-to-day operations; and, most importantly,
- management's insistence on safe operating practices.
Aéropro's primary means of ensuring safe operations management were supervision by managers; participation by all employees; training programs; company procedures; the company operations manual and SOPs; checklists; and service, safety and operations memos. The memos were posted in the pilots'common areas, and pilots were required to initial the service and safety memos after reading them. Aéropro was unable to provide minutes of safety meetings with personnel.
The operations manual was approved by TC and contained the company's guiding policies and procedures. The manual stated that all operations personnel must follow the procedures as indicated.
SOPs establish specific procedures for air operations by the company. TC does not approve SOPs and checklists for 703 and 704 operations. TC verifies their compliance to CAR 703.107. The AFM for each aircraft is approved and certified by the regulatory authority. The company is responsible for ensuring that the SOPs are consistent with the procedures and limits set out in the AFMs for the aircraft it operates.
1.16 Transport Canada Oversight
1.16.1 General
TC Civil Aviation (TCCA) expects that enterprises take an ownership role in proactively managing the safety of their operations and have programs in place to ensure their continued compliance with all regulatory requirements. TCCA's surveillance program has been designed to evaluate whether an aviation enterprise has implemented appropriate and effective systems. This is intended to provide TCCA with reasonable confidence that an enterprise is operating effectively and in compliance with regulations. The TC surveillance program conducts specific systems-based surveillance inspections at intervals based on risk indicators. The surveillance program is outlined in 4 documents: Civil Aviation Directive (CAD) SUR-008: Surveillance Policy; Staff Instruction (SI) SUR-009: National Planning Standard; SI SUR-001: Surveillance Procedures; and SI-SUR-002: Enhanced Monitoring. These documents, in conjunction with the Aviation Safety Program Manual, details TCCA's specific policies and procedures related to surveillance of aviation enterprises. The program is targeted at key systems, determined by certificate type and whether or not the enterprise is required to have a safety management system.
According to the Aviation Safety Program Manual that has been in effect since April 2009, safety management is based on the premise that hazards, risks and threats will always exist. Systemic and proactive management is therefore required to identify and control these hazards, risks, and threats before they lead to mishaps. A proactive safety culture involves TCCA and industry working together to reduce the likelihood of accidents. The manual states that the surveillance program is conducted on an enterprise basis.
The surveillance program is based on a systemic approach to managing risk. TC defines safety as the condition where risks are managed to acceptable levels. In the past, surveillance was done primarily through regulatory audits every three years, annual inspections in between audits, and additional audits or inspections if necessary. The objective of these activities was to determine regulatory compliance. The current surveillance program is carried out primarily through PVIs.Footnote 49 When the program was first implemented, the target PVI frequency was one per enterprise per year.
The current surveillance process can be summarized by the following steps: review of documentation; inspectors conduct onsite interviews and onsite sampling; and a report with findings of systemic deficiencies is produced. Subsequently a decision is made on how to address the non-compliance findings. The options for TCCA to address any identified systemic deficiencies include: allowing the company the opportunity to address the issue with a corrective action plan (CAP) that addresses the root cause of the issue; punitive enforcement action; certification (Notice of Suspension); or a combination of the above.
When planning a PVI, TC is not required to notify the enterprise in advance. However, in practice, the enterprise is notified of the inspection a few weeks beforehand. TC expects that the inspected organization will then be prepared to demonstrate to the inspection team that they have the appropriate systems in place to ensure compliance. In validating that an organization's systems are functioning, random sampling is conducted. The use of random sampling makes it difficult for an organisation to intentionally hide non-conforming activities.
The number of inspectors and the duration of the PVI depend on the size of the enterprise, the mandate of the PVI and the number of inspectors available to TC. In a PVI, TC systematically conducts interviews with key personnel and reserves the right to conduct interviews with employees. In practice, pilot interviews are not always conducted. The interviews are important for inspectors to fully understand and determine the effectiveness of certificate holder procedures and processes. The names of interviewees must not appear in the evaluation report. At the end of the PVI, a score from 1 to 5 is assigned. If the score is lower than 3, or if there are major findings of non-compliance, TC usually performs a risk assessment to determine what action the enterprise will be directed to take in order to manage the identified risks.
TC may conduct additional surveillance activities or enhanced surveillanceFootnote 50 if deemed necessary. Enhanced surveillance is a process to closely monitor a certificate holder, after an assessment or PVI has been conducted, to ensure that the certificate holder's regulatory performance does not deteriorate further while the certificate holder develops and implements measures to deal with its systemic deficiencies or regulatory non-compliance before the second or subsequent PVI is conducted. The expectations of enhanced surveillance are that the enterprise improves its systems, ensuring compliance with the CARs, and that a comprehensive examination of its systems confirms this. Enhanced surveillance performed following a PVI focuses on the components with major deficiencies. The plan must also include surveillance of systems that were not assessed or validated during the PVI. The enhanced surveillance plan must include the required allocation of resources.
1.16.2 Surveillance of Aéropro Operations by Transport Canada
Within the context of this occurrence, the following surveillance activities were reviewed:
- Safety analysis completed by TC in April 2007
- Inspection for regulatory audit of operations in March 2008
- PVI in October 2009
- Risk management in October 2009
- Revocation of approval of the operations director's appointment in November 2009
- Surveillance activity in May 2010.
- PVI in July 2010.
1.16.2.1 April 2007 Safety Analysis
In April 2007, TC conducted a safety analysis of Aéropro operations. Data were gathered from CADORSFootnote 51 (from 2001 to 2006), TSB investigations and discussions with TC inspectors. The report concluded that, unless there was a radical change in management culture, only close monitoring of Aéropro operations would improve its performance with regard to safety. Aéropro disputed the statistics and findings of the report and subsequently TC did not take further action.
1.16.2.2 March 2008 Regulatory Audit Inspection
TC performed its most recent regulatory audit inspection of Aéropro operations from 3 to 14 March 2008. TC made 17 findings of non-compliance with the CARs. The findings included the following:
- The operations manual and SOP manual for the company's Embraer-110 were non-compliant with regulations.
- There were deficiencies under the responsibility of the operations manager: incomplete training programs and operations manuals that were not compliant with existing regulations.
- The chief pilots of 703 and 704 operations had a number of shortcomings in training documentation and maintenance of crew training records.
- A number of pilot proficiency checks were performed by a company check pilot, but the training records did not indicate that the training had been completed.
- The training programs were non-compliant with existing regulations.
- The training records for 703 and 704 flight crews revealed several deficiencies.
- Training records were incomplete and training certificates were incomplete or non-compliant. Namely, the training records of 2 pilots did not indicate whether they had received theory and practical training on emergency procedures. The information obtained by the investigation indicated that at least one of these 2 pilots had not completed the practical training.
- An audit of flight documents revealed that several weight and balance sheets had not been signed by the pilot-in-command.
As a result of this inspection, Aéropro submitted a corrective action plan in response to the findings so that it could continue operations. TC subsequently approved the plan.
1.16.2.3 October 2009 Program Validation Inspection
The first PVI of Aéropro was conducted by a team of 4 inspectors from 5 to 9 October 2009. The company had been notified of the inspection in early September 2009. The objectives were to verify that the company had
- an operations manual containing procedures related to process;
- an operations manual that complied with regulations;
- personnel who complied with the operations manual; and
- a system that monitored company processes effectively.
At the beginning of the PVI, the Aéropro operations manager informed the TC team that the chief pilot for 704 operations had been absent since October 2008, a period of 12 months. From that point forward, the PVI focused primarily on the responsibilities of the operations manager. On 8 October 2009, before the PVI was finished, TC issued a Notice of Suspension to Aéropro because the company no longer had a qualified chief pilot for 704 operations.
The PVI report contained the following findings:
- The operations manager did not notify TC that one chief pilot's E110-type rating was expired since October 2008.
- A pilot had served as pilot-in-command with an expired type rating.;
- A pilot had flown single-crew flights for a period of time longer than the limit allowed by regulation.
- Five pilots had served as pilot-in-command on multi‑crew flights made in turboprop aircraft configured for six or more passengers that were not equipped with a CVR.
- The chief pilot of 704 operations did not keep his ratings or medical certificate up to date.
The PVI manager indicated in his report that TC would conduct enhanced monitoring of operations. The PVI convening authority (the manager of the Commercial and Business Aviation Division) was authorized to impose, at his discretion, enhanced monitoring if a score of 3 was not obtained. The regional director, the manager's immediate supervisor, needed to approve the enhanced monitoring. The PVI final report assigned a cumulative score of 2. The primary reason for this score was the finding that the operations manager had not carried out his responsibilities related to the CARs.
1.16.2.4 October 2009 Risk Management
In accordance with TC procedures, in response to the PVI results, TC conducted a risk assessment from 20 to 22 October 2009. The information made available to the risk management team included the PVI results and data obtained by TC in previous years. The risk assessment summary report stated that the company was non-compliant with the regulations. The specific breaches attributed to the operations manager concerned the training program, operating standards, crew scheduling, supervision of amendments to the operations manual, liaison with TC, and safety nets on board aircraft. The monitoring recommended by the team included the following elements:
- Revoking the approval of the appointment of the current operations manager.
- Delaying the Notice of Suspension to allow the company to hire a new operations manager.
- Attending training sessions.
- Doing more flight tests.
- Doing ramp inspections.
- Requiring the company to have a TC-approved safety officer.
- Revoking approval of all management positions occupied by the director of operations at both companies.
The team had identified a residual risk if the operations manager whose appointment at Aéropro was revoked were to remain in the same position at Sasair and continued to conduct himself in the same manner. TC had also noted the possibility of operations being transferred from Aéropro to Sasair. Two months earlier a PVI of Sasair had determined that the operations managerFootnote 52 was also not carrying out his responsibilities. TC considered that the findings of the Sasair PVI did not jeopardize the safety of its operations. Consequently, the operations manager had continued to perform his duties at Sasair from the Aéropro offices.
The interim Commercial and Business Aviation manager, the decision maker for this risk management activity, approved the “specific monitoring” option recommended by the team and carried out 5 of the 7 recommendations listed above. A safety officer was not considered necessary because that was the responsibility of the operations manager. The revocation applied only to Aéropro because the findings concerned that company's operating certificate.
The PVI final report stated that regulatory breaches had been identified and that the company would be subject to associated specific monitoring, and that the operating certificate and the operations manager would be subject to administrative measures to ensure compliance with the CARs. The TC instructions do not mention “specific monitoring” per se, but they do state that other monitoring activities can be conducted.Footnote 53 A number of factors were considered when deciding which type of monitoring to put in place, such as the aspects that needed to be monitored more closely, the anticipated benefits of replacing the operations manager, and the resources available to TC for enhanced monitoring. This type of ongoing monitoring, which lasts 90 days, requires more human and financial resources than other types of monitoring.
1.16.2.5 Revocation of the Operations Manager Appointment
On 9 November 2009, TC revoked its approval of the Aéropro operations manager after determining that he had not carried out his responsibilities to ensure that operations were conducted in accordance with the requirements of CARs 703.07 and 704.07.Footnote 54 On 10 November 2009, TC issued a Notice of Suspension to Aéropro because the company did not have an operations manager as required under CARs subparagraph 703.07(2)(b)(i).
On 23 November 2009, the Acting Regional Director, Civil Aviation, Quebec Region, sent the Aéropro AE a letter revoking its approval of the appointment of the company's operations manager. The AE was informed that the company was under specific monitoring and that it had to agree to provide TC with the dates of future ground and flight training for pilots and the dates of in-flight checks (PPCs or PCCs) 15 days in advance, until the next PVI. TC subsequently participated in the appointment process for a new operations manager at Aéropro, interviewing the applicants and reviewing theircredentials. In December 2009, TC approved the appointments of the new operations manager and the new chief pilot for 704 operations. TC considered the new operations manager would have a positive impact on Aéropro's regulatory compliance and safety culture.
1.16.2.6 May 2010 Monitoring Activity
On 3 May 2010, during the specific monitoring, the TC lead inspector for Aéropro noted irregularities in the pilot training program. Specifically, TC noted that pilots had not completed single-pilot PPCs and had served as pilot-in-command on multi-crew flights on turboprop aircraft that were configured with 6 passenger seats and were not equipped with a CVR. The company was required to submit another corrective action plan to address this finding.
1.16.2.7 Post-occurrence Program Validation Inspection
Following the occurrence involving C-FGIN, and in accordance with established procedures, TC performed an unscheduled, unannounced PVI from 24 June to 23 July 2010. The PVI was convened by the Acting Regional Director, Civil Aviation, Quebec Region. The mandate of the PVI was to inspect all aspects of operations and quality assurance (maintenance). The TC team had 11 inspectors. During the PVI, interviews were held with pilots. The inspection report noted 20 findings of non-compliance with the CARs, including the following:
- Pilot interviews revealed that procedures pertaining to aircraft defects were not always followed.
- Pilot interviews revealed that flight monitoring, flight tracking and telecommunications procedures were not always followed.
- Some pilots served as crew members on flights without having completed their training;
- Some pilots did not receive their minimum rest period.;
- One pilot's flight duty time was extended past the maximum allowable for 2 flights.
- One pilot served as a crew member without holding a valid licence.
- The new operations manager, who had held the position since December 2009, was not making sure that pilots kept their flight and duty time logs up to date.
- Some pilot training records were incomplete.
- Several components of the training course were not provided to pilots.
- The chief pilots had attested that the training of some pilots met the requirements of the company training program even though the minimum flight training times had not been completed.
- There were a number of instances of missing or non-compliant signage and safety equipment on board aircraft.
TC conducted the interviews as part of the post-occurrence PVI. These interviews revealed divergent opinions about the safety of operations. Some statements indicated that operations were safe and in compliance with the company SOPs, while others said the opposite. The information gathered during these interviews was used in the PVI final report, which stated, among other things, that:
- some pilots were not aware that the company had a published safety policy;
- there was a lack of communication between the various levels;
- some pilots had been asked to sign training forms when their training had not been completed; and
- management used a penalty-based system to limit pilots' flight hours in order to influence their behaviour.
In light of the PVI results, and given Aéropro's past history, TC analyzed its options in making a decision. TC decided not to replace all of the management personnel because that option had been tried, in part, but was not successful, and replacing all members of management would increase the risk. The 3 options considered were:
- Notice of Suspension and enhanced surveillance;
- cancellation of operator certificate; or
- immediate suspension and enhanced surveillance.
According to the analysis criteria, Options 2 and 3 had similar weighting, higher than that of Option 1. Option 3 was not selected because there was a high risk of recurrence given the company culture and history.
On 30 July 2010, TC issued a Notice of Cancellation of Air Operator Certificate for Aéropro. The Notice of Cancellation listed approximately 30 items dating from February 2001 to July 2010. Aéropro presented a preliminary request to quash the Notice of Cancellation for lack of procedural fairness, which was rejected by the Transportation Appeal Tribunal of Canada.
The TSB investigation highlighted differences between certain field practices and the written procedures in the operations manual and the SOPs. These findings are consistent with TC's findings from the July 2010 PVI.
Some defects were not recorded in the aircraft journey log. The systemic practice of discouraging people from recording defects in the journey log was intended to keep the aircraft from being grounded.
- A penalty-based system was occasionally used to limit pilots' flight time.
- The company allowed pilots to exceed flight duty times.
- SOPs and checklists were not used for all flights.
- The company required pilots to make flights on aircraft that did not have all the required equipment.
The TSB investigation also determined the following
- Several employees did not know about the safety policy published in 2010 as part of the SMS implementation.
- Some employees thought the former operations manager had held an official position within the company, but in reality he did not hold any position.
- Aéropro did not have a confidential internal system for employees to report safety concerns.
- No documentation was found to confirm that group safety meetings with pilots took place.
1.16.3 Program Validation Inspection Interviews
The PVI instructions state that interviews can be used to gain an understanding of company processes and procedures and determine their effectiveness. That person's statement may be used and disclosed later on as part of administrative or legal proceedings. The regulations do not guarantee absolute confidentiality to employees. For the July 2010 PVI, pilot interviews played a key role in making certain findings.
1.16.4 Aéropro Approved Maintenance Organization
The Aéropro Approved Maintenance Organization (AMO) was approved by TC in 1990 under CAR 573.02. The AMO was approved to perform maintenance on aeronautical products and held specializations in the following categories: Aircraft, Avionics, Components, Instruments, and Structures. The AMO primarily maintained the Aéropro and Sasair operations fleets. It was qualified to perform maintenance on 16 different types of aircraft, including the Beechcraft 90, the Beechcraft 100, the Piper-31, the Embraer 110, and the Merlin III, at 3 bases located in Québec, St-Hubert, and Sept-Îles. The Aéropro AMO was compliant with the CARs for the procedures described in the maintenance control manual (MCM), which defined, documented and governed all aspects of airworthiness for the aircraft of the maintenance organization and its personnel.
The technical personnel consisted of a maintenance director, a head technician, a quality assurance manager, an engineering clerk, base managers, aircraft maintenance engineers and mechanics, for a total of 13 employees. The maintenance director was defined in the regulations as the person responsible for maintenance (PRM). The PRM was accountable to the operations director for coordinating all maintenance activities and must ensure that they were carried out in accordance with the policies and statements set out in the MCM. Each person responsible for quality and other functions was accountable to the PRM. The Aéropro PRM was accountable to the AE of Aéropro.
A review of the defects in the log books and the maintenance actions performed on the aircraft confirmed that the pilots recorded few defects in the log books.
1.16.4.1 Transport Canada Surveillance of Aéropro AMO
The Aéropro AMO surveillance was done by TC Maintenance and Manufacturing Branch located in Québec. The relationship between this group of civil aviation inspectors and Aéropro was characterized by proximity and the high frequency of inspections.
The Aéropro AMO surveillance of 26 August 2008 resulted in a Notice of Suspension of the company's certificate. Aéropro had 30 days to implement all the corrective measures required by TC for the quality assurance program, maintenance control and to ensure that all procedures were applicable and effective. The AMO was to ensure that the corrective measures and decisions stemming from the findings were recorded. Follow-up was done to the satisfaction of TC. Aéropro's AMO remained in force without interruption.
From 25 to 27 February 2009, TC did a PVI of Aéropro specifically to validate the quality assurance program. The PVI involved an inspection of the records beforehand and familiarization with the quality assurance program as described in the company MCM. The on-site inspection included interviews with key personnel, sampling, and examination of procedures and records. There was also an audit of company activities to determine the effectiveness of the program and the degree of compliance with the CARs and the approved manuals. At the end of the inspection, program validation findings were noted. Aéropro took corrective measures for each non-compliant item to the satisfaction of TC.
TC conducted a targeted PVI on the Aéropro AMO from 31 March to 1 April 2010. The objective was to inspect the components of the quality assurance system. TC selected the functional area of company systems and procedures using the validation checklist to determine the degree of compliance with the CARs and with the company's approved manuals and documentation. The TC inspection did not reveal any findings of non-compliance; therefore, the company did not need to perform any further action on the quality assurance component.
On 24 June 2010, the day after the occurrence, TC mandated 4 inspectors to perform a special PVI on the Aéropro AMO. This PVI focused on the aspects of maintenance control and aircraft maintenance that have an impact on safety. At the end of the PVI, TC concluded that the Aéropro AMO met regulatory requirements.
1.17 Safety Programs
1.17.1 Voluntary Reporting Programs
Any individual can report safety concerns through voluntary programs such as the TSB SECURITAS program and the TC civil aviation issues reporting system (CAIRS).
The SECURITAS program, created in 1985, is a voluntary reporting program that anyone can use to report hazardous situations or dangerous practices or procedures. Legislation governing TSB does not require the organization to put in place a confidential voluntary reporting system. TSB receives approximately 60 aviation-related reports each year. TSB can only protect the confidentiality of the reporting party. The report will not be used against the reporting party in any legal, disciplinary or other proceeding. In the mid-1990s, budget cuts and a decrease in reports led TSB to significantly reduce promotion of SECURITAS. There was subsequently a significant reduction in the number of reports made under this program.
The CAIRS, created in May 2005, allows anyone to report a variety of issues, including safety issues. The system should not be used to report immediate risks or offences. The CAIRS is not designed to handle issues that should be reported through an air operator's SMS.
The SATOPS report recommended that TC establish a confidential, non-punitive system to encourage people to report safety concerns and infractions. The example given in the report is the aviation aafety reporting system (ASRS), established by the US Federal Aviation Administration (FAA) and administered by the National Aeronautics and Space Administration (NASA). The program allows anyone to report without reprisal any potentially unsafe actions, events and incidents in complete confidence, except in the case of accidents or criminal acts. The information is gathered to determine the allocation of resources for accident prevention and provide information on industry practices. In April 2011, the ASRS received 5071 reports broken down into the following categories (Table 4).
These reports resulted in 20 alerting messages: 10 concerning aircraft and their equipment, 4 concerning air traffic control equipment and procedures, 4 concerning airports and procedures, and 2 concerning aircraft maintenance procedures.
Table 4. Aviation Safety Reporting System report, April 2011
| REPORT INTAKE | |
| Air carrier/Air taxi pilots | 2,910 |
| General aviation pilots | 925 |
| Controllers | 716 |
| Cabin | 275 |
| Mechanics | 162 |
| Dispatcher | 56 |
| Military/Other | 27 |
| TOTAL | 5,071 |
In 2001, CARACFootnote 55 formed a working group to make recommendations on the development of a voluntary, non-punitive reporting system. Its final report, published in June 2002, determined that the program should embody the following:
- Stable, long-term government funding;
- Be insulated from traditional regulatory thinking;
- Ensuring confidentiality and privacy of the reporters;
- Provide waiver of sanctions / immunity from enforcement actions to operators and individual reporters;
- Have independent control over the allocation of resources;
- Provide data relating to emerging trends;
- Offer independence and impartiality from the regulator; and
- The program should have a management board and advisory board.
The working group considered the creation of a new voluntary reporting program to be the best method, and that a non-governmental organization should run the new program. The group did not think SECURITAS should be revitalized.
The investigation found only one follow-up on this issue since the publication of the working group's report. Non-punitive and voluntary reporting programs were on the agenda of the 10th CARAC Plenary, held on 19 May 2005. The meeting minutes stated the following:
- TC advised members that there are currently 2 systems in place to deal with the reporting of issues: the Civil Aviation Issues Reporting System (CAIRS), managed by TCCA, and/or SECURITAS, managed by the Transportation Safety Board (TSB).
- Transport Canada Civil Aviation (TCCA) would not support an independent voluntary, non-punitive reporting system, because TSB already has SECURITAS.
- Representatives of the Air Canada Pilots Association (ACPA) commented that the Working Group members were of the opinion that the systems currently in place were not adequate and that the Working Group did not support SECURITAS. ACPA was concerned that the work done by the Working Group would be lost.
- TCCA undertook to promote Civil Aviation Directive (CAD) 28, Civil Aviation Issues Reporting System (CAIRS), and advised that TCCA would provide feedback to the extent permitted by the Privacy Act.
There are a number of reasons and factors that contribute to employees not reporting their concerns or hazardous situations. The investigation determined that the following factors influenced some pilots at Aéropro:
- lack of knowledge of existing programs;
- fear that their identities would be disclosed to their employer;
- some dangerous practices not perceived as such;
- industry too small for voluntary reports;
- perception that TC would not follow up; and
- fear of reprisal.
Some pilots are said to have reported their concerns to TC. However, the investigation could not find documentation indicating that the pilots had made voluntary reports to TC before the occurrence. The investigation revealed that SECURITAS did not have any voluntary reports on Aéropro and that the CAIRS had one.
1.17.2 Safety Culture and Management
It is recognized that all members of an organization and the decisions made at all levels of a company have an impact on safety. The SATOPS study stated that management is responsible for the safety of day-to-day operations and must commit to promoting safe operating practices. Consequently, in the SATOPS study, TC identified the need to evaluate company management as part of an investigation in order to determine whether certain organizational factors contributed to the occurrence. The relevant recommendation was as follows:Footnote 56
The Transportation Safety Board should evaluate the management factors that contributed to the accident during the accident investigation.
A company's safety culture is demonstrated by its structures (procedures and processes), decisions and actions (behaviours) by management and employees, and safety-related perceptions (values and beliefs). A frequently cited definition of an organization's “safety culture”Footnote 57 is as follows:
Shared values (what is important) and beliefs (how things work) that interact with an organization's structures and control systems to produce behavioural norms (the way we do things around here) - Uttal (1983)."Footnote 58
A safety culture has an influence on all parts of an organization and is characterized by proactive initiatives for identifying and managing risks, commitment from management, and clear policies and procedures that are put into practice. A lack of a safety culture is associated with reactive initiatives rather than proactive risk-related initiatives. This can lead to non-compliant or unsafe practices. Management and employee decisions, actions and behaviour are indicators of an organization's safety culture. TC describes a safety culture as follows:Footnote 59
- An informed culture: people understand the hazards and risks involved in their own operation; staff work continuously to identify and overcome threats to safety.
- A just culture: errors must be understood but willful violations cannot be tolerated; the workforce knows and agrees on what is acceptable and unacceptable.
- A reporting culture: people are encouraged to voice safety concerns; when safety concerns are reported they are analyzed and appropriate action is taken
- A learning culture: people are encouraged to develop and apply their own skills and knowledge to enhance organizational safety; staff are updated on safety issues by management; safety reports are fed back to staff so that everyone learns the lessons.
The relationship between safety culture and management is reflected in part by the attitudes and behaviour of a company's management. Systemic safety management promotes a positive, effective safety culture. In an introduction to SMS,Footnote 60 TC presents the 4 P's of safety management: philosophy, policy, procedures and practices.Footnote 61 In this model, safety management begins with management, which establishes a philosophy acknowledging the existence of risks, sets the organization's standards and confirms that safety is everyone's responsibility. A company's policies determine how safety objectives will be met by clearly defining responsibilities; developing processes, structures and objectives to incorporate safety into all aspects of the operation; and developing the skills and knowledge of personnel. Procedures are directives for employees and set management's expectations. Practices are what really happens on the job, which can differ from procedures, in some cases increasing threats to safety.
1.18 Air Taxi Operations Under CARs Subpart 703
In the past decade, there have been 7 to 8 times more accidents involving air taxi (703) operations compared with other commercial passenger transport services: 704 (commuter) operations and 705 (airline) operations (Figure 5).
These accident statistics show a major difference between the total number of accidents for 703 operations and those for other passenger transport operations. This is a well-known situation and studies and interventions have been done with a view to reducing the risks.Footnote 62 There are significant differences between the types of operation, such as regulation, operating environment, equipment, and certain characteristics of pilot qualifications.
Regulation of air taxi operations is less stringent. For example, the recurrent training requirements are lower, SOPs are not approved by TC, the criteria for incident reporting are less restrictive, and air taxi operations are one of the last to be required to implement SMS.
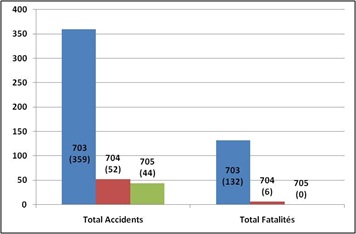
The operating environment for air taxi operations is more demanding: companies are smaller; flights are shorter and so there is a higher average number of take-offs and landings per hour of flight time; and the aircraft are exposed to more severe weather for most of the flight time because of the altitude of the flights. They also serve smaller airports and aerodromes in remote areas with minimal services such as navigation aids, emergency services, ground services, and flight planning.
Aircraft used by air taxi operations are often smaller and older. They are certified according to the safety standards that were in effect when they were manufactured, which are often less stringent than current standards. Flight simulators do not exist for most of these aircraft or are not available for crew training. These aircraft are often less well equipped, namely in the area of navigation aids and electronic safety equipment such as TAWS, GPWS, TCAS, RadAlt, WXR and autopilot.Footnote 63 Many of them are not equipped with a CVR or FDR. In addition, the flight parameter display and failure warnings are less sophisticated and can require greater cognitive effort from the pilot to understand the status of the aircraft. This can lead to errors during periods of high workload.
Pilots in air taxi operations are typically less experienced, have less training, and are younger than those in other operations. To obtain a position with an air taxi operator, pilots are required to complete a much lower number of flight hours than they would for commuter and airline operations. For a pilot, a position with an air taxi operator is generally an initial step toward accumulating enough flight hours for a position with a 704 or 705 operation. As a result, some pilots may not be committed to improving these operations. This is also a dilemma for the companies, because they invest in training pilots who leave for another operator shortly afterward. Pilot turnover is relatively high in air taxi operations.
The following laboratory reports were completed:
- LP080/2010 – Aircraft Performance Analysis;
- LP107/2010 – Throttle Quadrant and Propellers Examination;
- LP108/2010 – Annunciator Panel Examination;
- LP159/2010 – Image of Crash Site;
- LP171/2010 – Fuel Analysis;
- LP179/2010 – Fuel Pump Analysis;
- LP190/2010 – Documents Analysis;
- LP193/2010 – Audio Spectrum Analysis;
- LP014/2011 – Site Survey.
These reports are available from the Transportation Safety Board of Canada upon request.
2.0 Analysis
2.1 Introduction
The weather was not a factor in the occurrence. About 39 seconds after take-off, the crew reported a problem with the right engine. The aircraft stopped climbing, then lost speed and altitude before crashing 29 seconds later.
The destruction of the aircraft on impact and in the post-crash fire and the lack of a flight data recorder and cockpit voice recorder are factors that prevented the investigation from determining the exact circumstances of the occurrence. Nevertheless, the evidence gathered makes it possible to deduce what occurred.
The analysis will focus on the reported problem, management of the emergency, crew training, Aéropro management and culture, Aéropro surveillance by TC, and the lack of CVR data.
2.2 Condition of the Aircraft Before Take-off
Technical defects were not systematically recorded in aircraft journey logs and were often recorded only after repairs had been done. Also, because the low pitch stop failure warning system occasionally malfunctioned, pilots were asked to pull the LOW PITCH STOP warning light circuit breaker before take-off to avoid operational inconvenienceFootnote 64 in the event of a false alarm. Therefore, it was not possible to confirm the airworthiness of C‑FGIN before the flight.
Because APO201 was the first flight of the day, the pilots needed to check all of the aircraft systems using the pre-take-off checklist. It is reasonable to believe that these checks were done in the 11 minutes between boarding and the request to taxi to the runway. The crew did not report anything unusual on the radio to the company flight follower which suggests that the pilots did not notice any significant problems.
During this period of time, the pilot-in-command (PIC) would have reviewed the procedures for an abnormal situation during take-off. According to the PIC's course notes, the pre-take-off briefing would have consisted of listing each pilot's tasks in the event of an engine failure. However, in the absence of hard data and directives to this effect in the SOPs, the content of the briefing could not be established.
Next, the aircraft stopped for a few seconds at the taxiway holding position before entering the runway and performing a rolling take-off.
2.3 Take-off Run
The performance analysis of multiple take-off runs by C‑FGIN using ASDE radar data shows that engine power-up and aircraft acceleration were normal up to the rotation. The aircraft performance was essentially the same as the other take-off runs examined. However, the aircraft performance during take-off was lower than was published in the AFM. The aircraft travelled approximately 500 feet furtherFootnote 65 to reach the speed required for lift-off. If the crew had noticed a problem before rotation speed, the take-off could have been rejected without leaving the runway.
Based on the performance analysis of multiple take-off runs in June 2010 and the PIC's course notes, the crew would have initially set engine power to 1400 ft-lb of torque, possibly because of the effect of the increase in aircraft speed.Footnote 66 Next, the crew would have set the power to 1500 ft-lb as specified in the SOPs and not at maximum continuous power as per the AFM. It is likely that the crew complied with the Aéropro directive concerning take-off power limits. This directive, in contrast to the AFM, stipulated that the company parameters must be respected at all-time except for emergencies. The directive contained sanctions for pilots who did not comply.
2.4 Climb
It was not possible to determine the vertical flight profile from take-off to the first radar target at 160 feet agl. The Québec surveillance radar tracked the flight at 5-second intervals almost up to the site of the accident. Because the radar display is divided into increments of 100 feet and 10 knots, the exact trajectory and speed of the aircraft could not be re-created.Footnote 67 The limited precision of the radar data nevertheless provides an acceptable assessment of aircraft performance, albeit an approximate one.
Had the maximum continuous takeoff power been used, better climb performance could have been achieved. In the first 8 seconds of the climb, the aircraft accelerated to approximately 120 knots. The aircraft continued to climb to approximately 260 feet agl and then lost approximately 10 knots of speed when a right yaw was observed, suggesting a loss of thrust in the right engine.
After the take-off at reduced power, the aircraft performance during the initial climb was lower than that established at certification in the event of an engine failure on take-off. This meant the crew had less time to deal with the emergency situation.
2.5 Problem Reported in Flight
2.5.1 General
The co-pilot reported a problem with the right engine 39 seconds after take-off but did not specify the nature of the problem. A power lever was also pulled, as indicated by the gear warning sounding at that time. Two abnormal situations requiring a reduction in power were considered
- a failure of the flight low pitch stop system; and
- an engine failure/loss of engine power.
The possibility of an engine fire was ruled out because nothing to indicate this was observed in flight, during the examination of the wreckage or after the engines were examined.
2.5.2 Failure of the Flight Low Pitch Stop System
2.5.2.1 Flight Low Pitch Stop System Failure
According to the checklist, and the sequence of event timeline, it is likely that the crew would have functionally checked the system during the run-up systems check before flight. However, a flight low pitch stop system failure generally occurs on lift-off causing a change in propeller blade pitch, from its set position to a higher pitch and then starts to feather. The increase in pitch initially produces an increase in thrust on the affected side. Because of the increase in thrust, this type of failure does not have an abrupt and negative impact on aircraft performance.
According to the checklist, and the sequence of event timeline, it is likely that the crew would have functionally checked the system during the run-up systems check before flight. However, a flight low pitch stop system failure generally occurs on lift-off causing a change in propeller blade pitch, from its set position to a higher pitch and then starts to feather. The increase in pitch initially produces an increase in thrust on the affected side. Because of the increase in thrust, this type of failure does not have an abrupt and negative impact on aircraft performance.
Performing the first 3 items of the emergency procedure from memory is intuitive. As quickly as possible, the pilot pulls back on the power lever of the affected side to maintain engine torque within the prescribed limits, because exceeding the limits could lead to engine failure. The pilot then deactivates the low pitch stop system by pulling the PROP GOV-IDLE STOP circuit breaker. The propeller blade angle will then be controlled only by the propeller governor. The propeller governor will restore the pitch angle to maintain the selected propeller rpm. Finally, the crew sets the power lever to the desired power setting. However, the evidence gathered does not indicate if the engine and propeller controls had been repositioned to the appropriate power setting.
2.5.2.2 R PROP LOW PITCH Warning Light Circuit Breaker
Because it was common practice at Aéropro to pull the circuit breaker for the flight low pitch stop system warning light before take-off, and because the company did not offer practical training on this type of failure, the consequences of a flight low pitch stop system failure under these circumstances were analyzed.
Following a flight low pitch stop system failure on the right side, and without a warning light, the crew may have interpreted the initial left yaw as a loss of power in the left engine. On the other hand, the increase in right engine torque could also have meant a defect in the propeller governor or a mechanical fault in the propeller. In such a situation, it is reasonable to believe that the pilot would have instinctively pulled back the power lever to control the torque on the affected engine.
It can be concluded that, without the warning light, the identification of the failure and the carrying out of the appropriate emergency procedure would have been at least delayed. For these reasons, deactivating the flight low pitch stop system warning light or any other warning system would contravene the regulations and pose a significant risk to flight safety.
2.5.2.3 Probability of a Flight Low Pitch Stop Failure After Take-off
The system components retrieved at the accident site did not reveal any pre-existing defects. All damages to the right propeller and mechanism were caused by the crash. The wiring and some electrical components of the flight low pitch stop system were destroyed in the fire, so it was not possible to determine the condition of the system.
In the scenario involving a flight low pitch stop system failure on the right side after take-off, the aircraft would have been expected to briefly yaw left and indicate an engine torque increase or fluctuations while maintaining its acceleration and rate of climb. However, according to the radar data, the aircraft turned right, then stopped climbing at about 260 feet agl, its speed stabilizing at 110 knots before starting to decrease. Only the action of pulling back the power lever to decrease the engine power or a loss of power can bring the blades to low pitch as found.
If the crew had noticed a flight low pitch stop system failure and started to perform the low pitch stop failure procedure, they would have reduced the power of the affected engine, pulled the PROP GOV-IDLE STOP circuit breaker and returned power to the engine. If the low pitch stop had failed during take-off, the right propeller would have been found in a high (coarse) pitch position. The evidence indicates that engine power was reduced and that the PROP GOV-IDLE STOP circuit breaker was not pulled to regain control of the propeller.
These individual elements do not allow a flight low pitch stop system failure to be ruled out, but overall it is unlikely that the crew began the low pitch stop failure procedure in flight without finishing.
2.5.3 Failure/Loss of Engine Power
2.5.3.1 Engine Failure
All damage observed on the engines and their propellers was the result of the impact and the post-crash fire. It was therefore not possible to determine that there were pre-existing defects. Examination of the engines and their components did not reveal any signs of malfunction or defects that occurred in flight.
2.5.3.2 Left Engine and Propeller
The damage to the left engine was consistent with impact with the ground at medium to high engine speed. The ground scars from the left propeller suggest that it was rotating at approximately 2200 rpm. Examination of the warning lamp bulbs connected to the components of the left engine revealed that they were extinguished. This suggests that the left engine was operating normally during the flight and that the crew pulled the power lever of the right engine just before reporting the engine problem. However, the investigation was unable to determine whether the left engine was capable of producing the maximum power of 1628 ft-lb. The performance tests on the engines during routine inspections and the monitoring of engine performance trends documented by the pilots on a daily basis did not reveal any defects. It should be pointed out that the take-off power of 1628 ft-lb could only be tested by the crew on take-off. The procedure of not exceeding 1500 ft-lb of power limited the opportunities for crews to determine whether or not the engines were developing full power on take-off. The maintenance and operating practices did not allow them to determine whether or not the engines could produce the maximum power of 1628 ft-lb required at take-off and during emergency procedures.
2.5.3.3 Right Engine and Propeller
Examination of the right engine revealed that it was turning at very low speed or windmilling at the moment of impact. The damage to the right propeller and the ground scars it caused indicate that the engine was producing virtually no power. The right yaw on the flight trajectory indicates that this engine was developing less thrust. The crew noticed and reported a problem with the right engine. The tone heard in the radio communications indicates that the power lever for one engine had been pulled back. These observations are consistent with the right engine power being reduced by the crew in order to deal with an engine problem. The crew then had to deal with a loss of power in the right engine about 28 seconds after rotation speed was reached. The crew sometimes flew aircraft that were equipped with an autofeather system. The evidence from the right propeller confirms that it was not feathered, but was in the low pitch operating range.
Given these considerations, it is reasonable to conclude that the right engine experienced a problem in flight that led to a substantial loss of thrust.
2.6 Aircraft Performance with One Engine
In addition to the yaw and roll to the right, the right engine problem would be indicated in the cockpit by a rapid decrease in the performance readings of the right engine and probably a visual generator and fuel pressure alarm. The recommended procedure states that initial climb on one engine must be done at maximum continuous power with gear and flaps retracted and the propeller feathered, while maintaining Vyse.
At this point in the flight, the aircraft was likely configured for the climb: the flaps would have been retracted because no environmental or operational conditions required the flaps to be extended on take-off, and the gear would have been retracted once the aircraft reached a positive rate of climb. The flaps and gear were both up at the time of the occurrence.
It was not possible to conclude precisely how much power was being developed by the left engine when the right engine indicated a problem. Since the aircraft had not yet reached 400 feet agl, Footnote 68 the left engine power should have been the same as it was at take-off. The information gathered in the investigation, namely the analysis of aircraft performance during the ground roll, the company directives on take-off power, and the PIC's course notes, suggest that the crew performed a take-off with reduced power. It is therefore reasonable to believe that both engines were producing 1500 ft-lb when the problem occurred.
Because the left engine was not set at the take-off power specified in the AFM, the crew had to increase the power to 1628 ft-lb of torque.Footnote 69 According to calculations done by Hawker Beechcraft craft Inc., at 1628 ft-lb of torque with the right propeller at low pitch, the aircraft would be able to climb at approximately 100 feet per minute. However, the aircraft stopped climbing and its altitude stabilized briefly at 260 feet agl before losing speed and altitude. Based on the little radar data available, the aircraft trajectory suggests that the left engine power remained the same as at take-off and that consequently the flight continued at reduced power. If this was the case, either the crew did not increase power or the power lever adjustment did not provide 1628 ft-lb of torque. The investigation was unable to determine whether the lever setting would have made it possible to obtain maximum engine power.
The hypothesis that the crew did not set the power to maximum is not supported by accurate data, but by an optimum rate of climb calculated by Hawker Beechcraft Inc. and radar data that contains a certain margin of error. Taking the preceding information into account as well as the small gap between the rate of climb at 1500 ft-lb and 1628 ft-lb of torque, it was not possible to confirm one way or the other whether the flight continued at reduced power after the reported engine problem.
The additional step of applying full power added a delay during a very critical period. There is even a possibility that the crew could forget to do this, particularly when it is the opposite of what they usually do. TSB determined that this sort of procedure caused an accident on take-off in 2007.Footnote 70 TSB issued a safety advisoryFootnote 71 suggesting that TC take action to ensure that operators are aware of the need to use approved flight operations reference material, and that they ensure that crews use the correct flight operations reference material. TC subsequently published the safety advisory in Aviation Safety Letter Issue 2/2008.
2.7 Crew Management of the Emergency
2.7.1 General
It is important to stress that engine failure or problems at take-off is one of the most complex emergencies to manage on a twin-engine light aircraft. When an engine failure or problem occurs immediately after take-off, there is no time to consult the appropriate procedure before taking corrective action. In training, pilots learn the critical actions to be performed in this situation: apply full power, ensure that the landing gear is up, confirm identification of which engine has failed, and feather the propeller on the failed engine.
In this occurrence, the aircraft was flying close to the ground and trying to climb when the pilots were confronted with a significant loss of thrust. The pilots had to have memorized the emergency procedure and carried it out. Since the engine problem occurred relatively close to the ground, the crew had little time to identify the problem and then act in a co-ordinated manner. The items in the engine failure procedure were clearly listed in order in the AFM, the ECHKL and the Aéropro SOPs, as is required.
2.7.2 Crew Actions After the Engine Problem
When the problem arose, the pilots had to carry out the priority actions without being distracted. After the engine problem, the pilot flying would above all need to maintain control of and navigate the aircraft, while the pilot not flying would, at the request of the pilot flying, perform the actions specified in the applicable emergency procedure and then inform ATC of the situation. In the absence of a voice recording, we can only speculate as to what the crew did.
Taking into account the configuration of the aircraft and its speed and altitude when the engine problem occurred, the crew would have had to perform, in order, the following three critical actions:
- increase engine power to the maximum allowable power;
- confirm the identification of the affected engine; and
- feather the propeller of the affected engine if required.
Once the problem was identified, the PNF should have set the power to maximum once the PF called for maximum power. However, as discussed earlier, the power may not have been set to maximum. Three hypotheses may be put forward to account for the power levers not being set to maximum:
- the PF did not call for maximum power; he may have been overloaded in controlling the aircraft, which was destabilized by the engine failure, and thus focused his attention on flying;
- the PNF interpreted the call for maximum power as confirmation rather than a request to act. He may have thought that the PF was saying that he had set the power to maximum. However, if this were the case, the PNF would normally have had to verify that the power was actually set to maximum; or
- the Aéropro procedure for take-off at reduced power led the crew to believe that the power was already set to the maximum allowable.
Crew confirmation of the right engine problem is corroborated by the engine power lever being set to idle and the problem being reported to ATC.
2.7.2.1 Configuration of the Right Propeller
The last critical action required, feathering the right propeller, was not performed. Unlike the other aircraft flown by the PIC, C-FGIN was not equipped with an autofeather system. Even so, the emergency procedure was the same, regardless of whether this system was present. It is possible that the crew omitted to feather the propeller because they were used to having an autofeather function on other aircraft. The only indicators of automatic feathering for the crew are a reduction in propeller speed and the position of the propeller control lever on the console between the 2 pilots. The absence of specific task distribution was conducive to the omission of critical actions.
The co-pilot contacted the airport controller 11 seconds after the problem is presumed to have occurred, and spent 19 of the last 29 seconds of the flight talking to ATC instead of focusing on performing critical tasks. The interruption of the emergency procedure gives reason to believe that the crew placed a higher priority on informing ATC of the aircraft's return due to the problem with the right engine. The radio communications distracted the co-pilot's attention from his tasks at a crucial point in the emergency procedure. Of all of the items in the engine failure procedure, feathering has the greatest influence on the eventual outcome of the flight. It is essential for continuing the flight because it results in the best climb performance. The propeller in the low pitch position generated significant drag that increased with the speed of the aircraft. Therefore, if the pilot tried to accelerate to Vyse, the gap between the thrust and excessive drag would narrow and the rate of climb and speed would deteriorate. The right propeller was not feathered; therefore, the rate of climb was compromised by excessive drag.
2.7.2.2 Communications with ATC
It is likely that the PNF's call to the airport controller was conditioned by stress and the application of air traffic rules in a normal situation. Under normal conditions, pilots flying in controlled airspace must inform ATC before deviating from an instruction so that they can obtain a new clearance. However, in an emergency situation, pilots must take all measures considered necessary before contacting ATC. Still, pilots are very rarely confronted with this situation; there was no evidence that the co-pilot had dealt with such an emergency before. And because the pilots' flight training was done under normal conditions, they were accustomed to contacting ATC before changing heading, even in engine failure simulations.
With rare exceptions, emergency calls are issued under the authority of the PIC. Because the PIC is responsible for the operation and safety of the flight, it is unlikely that the co-pilot decided on his own authority to land back on Runway 30. It is therefore reasonable to think that the co-pilot contacted ATC after the PIC stated his intention to return to the airport. The co-pilot contacted ATC
- either on the orders of the PIC; or
- in response to the decision being made to return for a landing on Runway 30.
In either case, the priority given to the communications with ATC limited the crew's ability to manage the failure. The crew should have first performed the tasks required by the situation. ATC expects the pilots to perform the necessary actions before reporting the situation. However, ATC expects to be informed as soon as possible of any changes in direction or altitude, in order to minimize the possibility of conflict with other aircraft.
The co-pilot's last communication, 13 seconds before impact, indicates that the pilots were aware that the aircraft was not climbing. It appears that neither pilot had diagnosed the configuration problem, i.e., that the right propeller was not feathered. The PIC was quite likely overloaded with tasks. He had to control an aircraft at reduced power that was greatly unbalanced by the drag on the right propeller, which resulted in degraded aerodynamic performance that made it impossible to clear the rising terrain directly ahead. In such circumstances it can be imagined that the PIC's full attention was devoted primarily to controlling the aircraft and that this would have prevented him from noticing that the right propeller was not feathered.
2.7.3 Aéropro SOP for Emergency Situations
Because the Beechcraft A100 King Air can be operated with just one pilot, the AFM, CHKL and ECHKL specify only the sequence of actions to be performed in a procedure. The distribution of tasks between 2 pilots is not mentioned and there is no requirement to do so.
However, when an aircraft is operated with 2 pilots, both should know the tasks for which they are responsible and the order in which they are to be performed. This provides greater assurance that all prescribed actions are carried out at the appropriate time. Crew coordination measures should generally be covered in the SOPs. Taking its policies and the specific characteristics of its operation into account, the operator should define the tasks of each pilot in a multi-pilot crew. For the Beechcraft A100 King Air, Aéropro specified and published in its SOPs the tasks for each pilot only for normal procedures. The distribution of tasks between crew members was not specified for emergency procedures. Consequently, when the problem occurred, the 2 pilots could not rely on an established routine for performing the required tasks in a coordinated manner. The absence of written directives specifying which pilot was to perform which tasks may have led to errors in execution, omissions, and confusion in the cockpit.
2.7.4 Crew Training in the Event of Engine Failure
According to the information obtained, neither of the 2 pilots had previously dealt with a real-life engine failure. Carrying out the procedure for an engine failure at take-off required skills that were rarely used even in routine training. Because the pilots' training had not included the use of a twin-engine simulator, they had not been required to work as a crew in emergency conditions.
The 2 pilots could practise performing the engine failure procedure only during flight training. However, for obvious safety reasons, the training exercises consisted of a simulated engine failure at a minimum height of 400 feet agl. Because the engine was not shut off and the propeller was not feathered, the pilots were never required to perform the full procedure for an engine failure on take-off. Furthermore, the performance of a relatively light Beechcraft A100 King Air during a simulated engine failure is significantly higher than that of a loaded Beechcraft A100 King Air that has experienced engine failure at low altitude. This means that the pilots were never exposed to the performance they encountered when the engine problem occurred.
The lack of formal directives on task distribution also did not give Aéropro the opportunity to train its pilots to respond uniformly to an emergency situation in a coordinated manner when serving on a multi-pilot crew. The PF had practised engine failures and passed his PPC for single-pilot and multi-pilots, which included an engine failure exercise on a precision approach in single pilot condition. It is unlikely that the few hours of flight training devoted to crew coordination could have given pilots the opportunity to reinforce their knowledge of the concepts essential to effective crew resource management.
The crew needed to make decisions and act quickly but could not rely on previous experience, either in real life or in a simulator. Because the pilots' experience was limited to simulations during training, they were probably not prepared to switch within a fraction of a second from a routine flight situation to an emergency that required availability, coordination and extreme concentration. Although the crew had the training required by regulation, they were not prepared to manage the emergency in a coordinated, effective manner.
2.7.5 Crew Coordination
The investigation had to rely on the little radar data available, the analysis of ATS recordings, the examination of the markings on the ground, and the examination of the wreckage to assess the coordination between the 2 pilots. Without CVR data, it was impossible to determine the communications between the 2 pilots or their understanding of the situation. Using the established facts, the investigation can make inferences about the coordination between the 2 pilots.
The pilots were faced with a serious but known emergency situation. They had very little time to understand the situation and take the necessary action.
Because the aircraft could be flown with just one pilot, all of the procedures were designed to be carried out by only one pilot. While operating the plane with 2 pilots reduces the individual workload of each pilot, it requires effective resource management. Effective crew resource management requires that pilots agree to a mutual plan and that they both understand the situation. It also requires leadership, communication, and task coordination. In an emergency situation where time is short and the workload is high, these concepts become more critical to the success of the flight.
The right propeller not being feathered, the flight being continued with degraded performance, and the priority given to ATC communications indicate that the crew did not fully understand the situation and were not coordinating their tasks effectively.
2.7.6 Impact with Terrain
The established facts indicate that the crew did not attempt an emergency landing. The last radio communication 10 seconds before impact stated that the crew still intended to return to the airport. If the crew changed their plan following this radio exchange, there was very little time to choose a landing site and configure the aircraft. In the final seconds of the flight, the crew could perform only limited manœuvres to avoid obstacles. The slight deviation 5 seconds before impact was probably made to avoid the trees. The crew could not know that they were directing the aircraft toward a berm. The retracted flaps and landing gear and the asymmetry of the engine power indicate that the crew did not plan to land. Extending the flaps would have helped reduce speed at impact.
For emergencies involving engine trouble, crews on multi-engine aircraft are trained to land at the nearest airport (see Figure 2, which is from the SOPs) rather than land on a convenient surface. The aircraft are designed to be capable of flying on only one engine. There is no procedure to prepare pilots for conducting a forced landing on unsuitable terrain. The crew's intention to return to the airport was consistent with this training. There is a natural tendency to continue with a plan rather than consider alternatives, in spite of how the situation develops.Footnote 72 This probably influenced the crew to maintain their intention to continue the flight and return to the airport. In this tense situation, the crew had very little time to recognize the need to change their plan, consider an alternative for which they were not trained, and carry out this new plan. Landing in a field would invariably carry the risk of injury, damage to the aircraft and significant operational consequences. When a choice must be made between a known negative result and an unknown risk, there is a tendency to opt for the latter.Footnote 73 In the absence of a CVR, it is impossible to determine the crew's exact intentions with any certainty. However, in light of the established facts, it can be concluded that the crew was trying to return to the airport and the aircraft crashed. The impact with the berm caused worse damage to the aircraft.
2.8 Survival Aspects
The crash occurred shortly after take-off, when the fuel tanks contained approximately 388 gallons of fuel. The location of the crew members and the fact that all of the passenger seatbelts were unbuckled show that all occupants survived the impact. This also suggests that the crew tried to start evacuating the aircraft. The aircraft's upside-down position and the damage it sustained prevented the occupants from evacuating, causing them to succumb to the smoke and the rapid, intense fire.
2.9 C-FGIN Maintenance History
The documentation suggests that C-FGIN was maintained in accordance with existing regulations. However, defects were not always recorded in the aircraft journey log, and the work done on C-FGIN on 20 June was not recorded in the journey log until 22 June, after four flights. Given these established facts, it was impossible to determine the exact airworthiness of the aircraft before the flight. Besides being a breach of regulations, a lack of rigour in documenting maintenance work makes it impossible to determine the exact condition of the aircraft.
2.10 Safety Culture at Aéropro
Fundamentally, a safety culture requires a concrete, true commitment from management and a working environment that encourages prudent behaviour and decision making despite the economic impacts. A safety culture must be fair but must not tolerate wilful violations. A safety culture must also encourage all employees of an enterprise to report their safety concerns. Several practices, some of which were related to economic considerations, introduced significant safety risks. Because TC was about to require 703 operations to implement an SMS, Aéropro began the process. However, the structures and mechanisms of an SMS were not in place at the time of the occurrence. The company operated in a reactive rather than the proactive manner that is intended with an SMS.
Some of these organizational practices, which were known to management, were contrary to the company's written directives. The organizational and systemic nature of these practices indicates that they originated with management. These institutional deviations designed to circumvent safety requirements suggest that management was not fully committed to safety promotion. The following practices taken together demonstrate a poor safety culture at the company:
- Not all defects were recorded in the aircraft journey log, contrary to company procedures (section 1.6.3.2).
- The autopilot was not operational for over 120 days, contrary to the requirements of Aéropro's minimum equipment list (MEL) for the Beechcraft A-100 King Air (section 1.6.3.3).
- The repairs to the propeller de-icer were not recorded in accordance with the CARs and company procedures (sections 1.6.3.2 and 1.6.3.5).
- There was no task distribution between the crew members in the emergency checklists for the Beechcraft A100 King Air (section 1.6.5.1).
- The company SOPs of setting the engine power to 1500 ft-lb all the time, except for an emergency, was introduced without a formal assessment of the associated risks. The procedure was intended to reduce operating costs but came at the expense of procedures established by the manufacturer and approved by the regulator (section 1.6.5.2).
- There was no emergency procedure for low pitch stop system failure in the emergency procedure checklist (section 1.6.5.5).
- The flight low pitch stop system warning light was deactivated (sections 1.11.8 and 2.2).
- There was a conflict between the company safety culture, where all employees were encouraged to report safety concerns, and the existence of a penalty-based system.
- There was no documentation confirming that safety meetings were held.
- There were numerous findings made concerning training records and programs (section 1.16.2).
The practice of not recording all defects in the aircraft journey log was established in order to avoid grounding an aircraft for a problem that was not deemed essential for making a flight. The technical condition of the aircraft was not indicated in a single location; some defects were recorded in a parallel system.
In such a case, crews are unable to determine the actual condition of the aircraft at all times, and as a result are deprived of information that may be critical in an emergency.
Operators have the authority to devise their own flight assignment system. Nevertheless, remuneration based on hours flown has previously been identified as a safety issue because of the potential direct negative impact on a pilot's decision making. And with a monetary commitment of a training bond, this could put pilots in a difficult position: comply with practices or be punished; or leave the company and pay the balance of the training bond. The majority of pilots working for air taxi operators are generally less experienced and more vulnerable to operational and organizational pressures, and work in the most difficult conditions with the least safety measures. The organizational practice of a penalty-based system for limiting the number of flying hours can influence pilots' decision making and thus create a safety risk.
2.11 Surveillance of Aéropro Operations by Transport Canada
Fundamentally, TC's surveillance system is based on routine inspections for which advance notice is usually given. The enterprise is informed of shortcomings noted during these inspections and is required to submit a corrective action plan that must be approved by TC. Once this process is complete, surveillance is then conducted at a future inspection. This surveillance can therefore be described as routine and spot monitoring rather than ongoing.
The program validation inspection (PVI) manager in the October 2009 PVI noted that, in accordance with his interpretation of the inspection instructions, enhanced monitoring should have been conducted. However, it was up to the convening authority to decide what type of surveillance to apply. The convening authority opted for specific surveillance. Although “specific surveillance” is not mentioned in the PVI instructions, TC instructions state that it can be considered an additional option. Enhanced surveillance would have required more resources than specific surveillance, and TC inspectors already had a busy inspection schedule in the first year of the PVI. Enhanced surveillance would have involved monitoring all Aéropro systems as well as focusing on the shortcomings noted in the PVI, and consequently would have increased the likelihood of spotting shortcomings before the post-occurrence PVI.
Specific surveillance targeted the training program, which was previously found to have shortcomings. With the appointment of a new operations manager, TC expected a significant improvement in safe operations management. TC's decision to conduct specific rather than enhanced surveillance after the October 2009 PVI was in accordance with the standards of the new surveillance program.
The extended absence of a chief pilot is a significant regulatory violation given the responsibilities of the position. Other findings of non-compliance noted in the October 2009 PVI pertained to the operations manager. As a result, risk management targeted the work of this manager. Revoking the appointment of an operations manager is a relatively exceptional administrative action. Imposing additional surveillance is a concrete action that requires the enterprise to commit to resolving the non-compliant items in order to maintain its operating certificate and continue operations. After the October 2009 PVI, TC took significant measures to ensure that Aéropro complied with the CARs and more effectively managed risks associated with the safety of air operations.
A major accident is an impetus for a special (unscheduled) PVI. TC therefore convened and conducted a PVI following the accident on 23 June 2010. The inspection included all aspects, given the scale of the accident and Aéropro's history. In its risk management following the June to July 2010 PVI, TC considered all elements of Aéropro's record as well as the PVI findings. The findings of violations pertained to the management staff. With the same people in place, TC deemed the risk of recurrence unacceptable. TC cancelled Aéropro's operating certificate as a result of the findings of the unscheduled PVI and with the accumulation of prior findings dating back to 2001.
There was a major difference between the findings of the 2 PVIs, which were conducted 9 months apart. They were convened for different reasons and with different mandates. By definition, a PVI is a targeted inspection of 1 or more aspects of an enterprise. The October 2009 PVI was a routine inspection where the focus was on the responsibilities of the operations manager, prompted by findings made at the beginning of the inspection. The June and July 2010 PVI was a special, unscheduled inspection that lasted 4 weeks and had a broader mandate, as it
came after a major accident and the enterprise had already been under additional
surveillance. TC had a much larger team for this PVI, and pilot interviews were used as an inspection tool. The difference between the findings of the 2 PVIs, one held before and one held after the accident, is that the latter had no advance notice and involved more inspectors, was held over a longer period and had a broader mandate, and pilots were interviewed.
Although TC is not required to provide advance notice of a PVI, it usually lets the enterprise know a few weeks beforehand. This ensures that enterprise personnel will be available and is consistent with the principle of mutual cooperation between TC and air operators, which is a cornerstone of a risk management–based system where the focus is on making management of an enterprise accountable. A TC inspection can lead to severe consequences, even the cancellation of an operating certificate. This invariably has an influence on enterprises as they prepare for an inspection, and so they will take action if they receive advance notice of an inspection. The new inspection framework places the emphasis on risk management and processes with less auditing and operations-focused and in-flight inspections.
A number of shortcomings noted in the post-accident PVI were present before the accident but had not been identified by TC as part of its surveillance program, including specific surveillance. After the post-accident PVI, TC had more information available for its decision on whether to cancel the operating certificate. TC was expecting the replacement of the operations manager to have positive results, namely greater compliance with regulations, given the responsibilities of the position. The safety culture does not depend on just 1 manager, but all employees of the company, and begins with full commitment from the AE and other managers. The significant measures taken by TC did not have the expected results to ensure compliance with regulations, and consequently unsafe practices persisted.
SOPs and checklists for 703 operators are not approved by TC. Operators are responsible for complying with the manufacturers' flight manuals, which are approved by TC. TC may review these documents as part of its inspections. The reviews are not conducted systematically. TC inspections did not reveal that Aéropro had deviated from the take-off power procedure, as was the case in occurrence A07C0119.
2.12 Non-punitive and Confidential Voluntary Reporting Program
The Safety of Air Taxi Operations Task Force (SATOPS) report recommendation to put a non-punitive and confidential system in place has not yet been fully realized. The systems in place, such as SECURITAS and CAIRS, only partly meet the criteria of the ideal system. However, they do not guarantee absolute confidentiality and are all but unknown in the aviation industry. This provides some explanation as to why pilots and other employees who want to report dangerous actions or conditions do not do so. The absence of an effective non-punitive and confidential voluntary reporting program means that hazards in the transportation system may not be identified.
2.13 Lack of CVR Data for the Investigation
The intent of the CARs is that commercial aircraft with 6 or more seats and operated by 2 pilots are to be equipped with a CVR. CVR data are crucial in the event of an aviation occurrence. In November 2009, TC issued a Notice of Proposed Amendment (NPA) to CAR 605.33, which would make CVRs mandatory in aircraft operated by 2 pilots in conditions similar to
C-FGIN. As a result of the delay in amending the CARs, 3 Beechcraft King Air aircraft that were recently involved in occurrencesFootnote 74 did not have CVRs. The investigations were deprived of critical data to account for these occurrences, in which 9 people were killed and 2 were seriously injured.
Because of the major damage caused by the aircraft fire, the examination of the components of C-FGIN yielded few clues that would help determine the nature of the engine problem reported and the information available to the crew. In the absence of a CVR, the only recordings available were recordings from ATS, radar and the security cameras belonging to the airport and to Aéropro, which were extremely useful. However, given that the recordings were not designed to be used in an investigation, the quality, accuracy and quantity of data were limited. It should also be pointed out that if the accident had occurred after take-off at an uncontrolled aerodrome or outside of radar range, these recordings would not be available. The use of a CVR by air taxi operators, which often go to remote locations, is therefore essential in case of an accident.
CVRs do not just record pilots' speech; they also record cockpit noise, for example from the engines, propellers and switches being moved. Without audio information from the cockpit, the investigation was hampered by a lack of concrete data. For example, the crew behaviour at different phases of the flight, the coordination between the pilots and the management of the emergency could not be fully evaluated.
The lack of recorded information significantly impedes the TSB's ability to investigate accidents in a timely manner which may prevent or delay the identification and communication of safety deficiencies intended to advance transportation safety.
3.0 Conclusions
3.1 Findings as to Causes and Contributing Factors
- After the take-off at reduced power, the aircraft performance during the initial climb was lower than that established at certification.
- The right engine experienced a problem in flight that led to a substantial loss of thrust.
- The right propeller was not feathered; therefore, the rate of climb was compromised by excessive drag.
- The absence of written directives specifying which pilot was to perform which tasks may have led to errors in execution, omissions, and confusion in the cockpit.
- Although the crew had the training required by regulation, they were not prepared to manage the emergency in a coordinated, effective manner.
- The priority given to ATC communications indicates that the crew did not fully understand the situation and were not coordinating their tasks effectively.
- The impact with the berm caused worse damage to the aircraft.
- The aircraft's upside-down position and the damage it sustained prevented the occupants from evacuating, causing them to succumb to the smoke and the rapid, intense fire.
- The poor safety culture at Aéropro contributed to the acceptance of unsafe practices.
- The significant measures taken by TC did not have the expected results to ensure compliance with the regulations, and consequently unsafe practices persisted.
3.2 Findings as to Risk
- Deactivating the flight low pitch stop system warning light or any other warning system contravenes the regulations and poses significant risks to flight safety.
- The maintenance procedures and operating practices did not permit the determination of whether the engines could produce the maximum power of 1628 ft‑lb required at take-off and during emergency procedures, posing major risks to flight safety.
- Besides being a breach of regulations, a lack of rigour in documenting maintenance work makes it impossible to determine the exact condition of the aircraft and poses major risks to flight safety.
- The non-compliant practice of not recording all defects in the aircraft journey log poses a safety risk because crews are unable to determine the actual condition of the aircraft at all times, and as a result could be deprived of information that may be critical in an emergency.
- The lack of an in-depth review by TC of SOPs and checklists of 703 operators poses a safety risk because deviations from aircraft manuals are not detected.
- Conditions of employment, such as flight hours–based remuneration, can influence pilots' decisions, creating a safety risk.
- The absence of an effective non-punitive and confidential voluntary reporting system means that hazards in the transportation system may not be identified.
- The lack of recorded information significantly impedes the TSB's ability to investigate accidents in a timely manner, which may prevent or delay the identification and communication of safety deficiencies intended to advance transportation safety.
4.0 Safety Action
4.1 Action Taken
4.1.1 Transport Canada
Transport Canada has made significant changes to its surveillance program. These changes include updates to the methods used for surveillance planning and the introduction of tools that provide an improved capacity for the monitoring and analysis of risk indicators within the aviation system.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on . It was officially released on .