Controlled Flight into Terrain (CFIT)
Pacific Coastal Airlines
Grumman G-21A C-FPCK
South Thormanby Island, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
At about 1013 Pacific Standard Time, the amphibious Grumman G-21A (registration C-FPCK, serial number 1187), operated by Pacific Coastal Airlines, departed from the water aerodrome at the south terminal of the Vancouver International Airport, British Columbia, with one pilot and seven passengers for a flight to Powell River, British Columbia. Approximately 19 minutes later, the aircraft crashed in dense fog on South Thormanby Island, about halfway between Vancouver and Powell River. Local searchers located a seriously injured passenger on the eastern shoreline of the island at about 1400. The aircraft was located about 30 minutes later, on a peak near Spyglass Hill, British Columbia. The pilot and the six other passengers were fatally injured, and the aircraft was destroyed by impact and post-crash fire. The emergency locator transmitter was destroyed and did not transmit.
1.0 Factual Information
1.1 History of the Flight
Pacific Coastal Airlines (Pacific Coastal) was hired by Peter Kiewit Sons Co. (Kiewit), a construction company with projects in various locations on the British Columbia coast, to transport Kiewit employees and cargo between Vancouver International Airport (CYVR)Footnote 1, British Columbia, and a work camp near the head of Toba Inlet, British Columbia, about 100 nautical miles (nm) north-northwest of Vancouver. All flights were conducted in a Grumman G-21A (Goose) amphibious aircraft under visual flight rules (VFR). Flights were conducted seven days a week, usually several times per day, and frequently involved en route stops at the Powell River Airport (CYPW), British Columbia, about 60 nm northwest of Vancouver, to pick up and drop off Kiewit employees.
The pilot arrived for work at the hangar at about 0900.Footnote 2 At 0930, he reported to the company dispatch centre where he was given the flight manifest and a weather information package. The pilot and dispatcher discussed the weather information package and the pilot was advised to proceed to Toba Inlet if the weather did not permit landing at CYPW.
The flight was scheduled to depart from the Vancouver International Water Aerodrome (CAM9) at 1000 with seven passengers. The aviation routine weather report (METAR) issued at 0900 for Vancouver recorded the wind as 110°T Footnote 3 at 10 knots and 2 ½ statute miles (sm) visibility in mist. Cloud cover formed a ceiling at 500 feet above ground level (agl). The temperature was 10°C, the dewpoint 9°C. The Environment Canada Weather Depiction Prognosis forecast low ceilings and visibility along the coast for the area of the flight route. Although the reported weather at the Toba Inlet destination was above VFR limits, weather at CYVR and CYPW was below VFR limits at the scheduled departure time. It is noteworthy that Pacific Coastal flights departing from CYVR that morning under instrument flight rules (IFR) had been delayed due to weather below IFR minima at coastal destinations near the accident flight route.
Following the weather briefing, the pilot proceeded to the aircraft to load the cargo and board the passengers. During his pre-flight briefing, he advised the passengers that the flight would be conducted at low altitude and that if anyone was concerned, they could deplane. No one deplaned. The aircraft was releasedFootnote 4 by dispatch at 1001.
The automatic terminal information service (ATIS) issued for CYVR at 1009 reported that the wind had decreased to 8 knots and visibility had decreased to 2 sm. The pilot requested and received authorization from Vancouver air traffic control (ATC) to depart under special VFRFootnote 5 via the SALMON NORTH departure. This published VFR floatplane route requires aircraft to be equipped with an area navigation system such as a global positioning system (GPS) to identify the SALMON VFR call-up/check-point, about 6 nm offshore. At approximately 1013, the aircraft departed CAM9 westbound towards the SALMON VFR check-point. The accident flight was the only fixed-wing VFR departure from CAM9 or CYVR before 1049 that day because other operators had cancelled or delayed their flights due to the low visibility. About three minutes after take-off, approximately 2 sm east of the SALMON VFR check-point, ATC approved a right turn out of the CYVR control zone (a modification to the published SALMON NORTH departure route). At this point, the aircraft turned onto a track of about 308°T. A slight course change to the west was made after which the aircraft resumed the 308°T track until radar coverage ended. About four minutes after take-off, the pilot reported to CYVR tower that the visibility was about 2 to 2 ½ sm, and that he could probably climb to 200 to 300 feet above sea level (asl). About six minutes into the flight, and about two minutes before exiting the CYVR control zone, the pilot reported his position as 7 ½ nm from CYVR and noted that visibility had improved to about 4 sm. The majority of the route was greater than 4 nm from land or other discernable features to assist navigation. The last communication from the pilot was at about 1021, when he advised ATC that he was clear of the zone.
The first nine minutes of the flight appeared on CYVR radar, ending about 21 nm northwest of CYVR, about 15 miles southeast of the accident site. Radar returns show that the aircraft's ground speed remained steady around 140 knots, normal cruise speed for this aircraft, allowing for the 8-knot to 15-knot tailwind encountered between CYVR and South Thormanby Island. Although there was no intervening terrain between the radar source and the aircraft, the radar coverage was likely limited because of the low altitude at which the aircraft flew. Of 110 valid radar returns, 10 returns (9 per cent) showed the aircraft's altitude as 0 feet asl, 96 returns (87 per cent) showed the altitude as 100 feet asl, and 4 returns (4 per cent) showed the altitude as 200 feet asl. No radar returns showed the aircraft's altitude higher than 200 feet asl.
Approximately 12 minutes after departure, Pacific Coastal dispatch tried unsuccessfully to contact the pilot to advise him that a special weather observation at CYPW indicated that visibility had deteriorated to 3/8 sm in fog and remained below VFR limits. Shortly after 1032, local authorities learned of a probable aircraft crash in dense fog on South Thormanby Island.
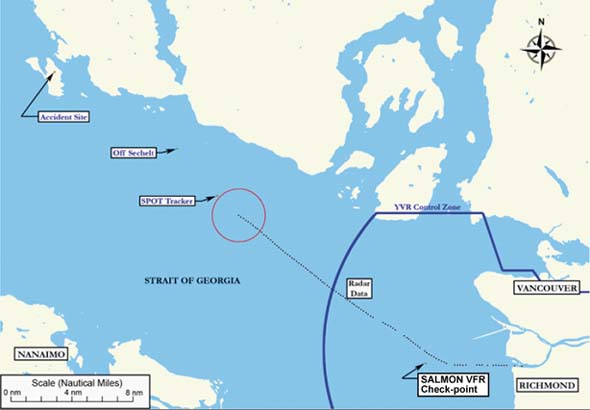
At 1110, 15 minutes after the aircraft's estimated time of arrival (ETA) at CYPW, Pacific Coastal employees at CYPW called their dispatch centre in Vancouver to say that the aircraft had not arrived. The Pacific Coastal dispatchers accessed the SPOT Satellite Messenger (SPOT)Footnote 6 website and mistakenly accessed the previous day's data and concluded that the aircraft had arrived at Toba Inlet. The dispatchers assumed that the pilot had bypassed CYPW due to poor weather conditions and continued on to Toba Inlet as per the alternative plan discussed before departure. However, when Kiewit contacted Pacific Coastal dispatch at 1145 to report that the aircraft had not arrived at Toba Inlet, the dispatchers rechecked the SPOT website and determined that the last recorded position was at 1025 near Sechelt, just over one third of the distance from Vancouver to Powell River. At 1210, Pacific Coastal dispatch contacted the Victoria Joint Rescue Coordination Centre (JRCC) to report the aircraft overdue. Poor visibility around the island due to fog and cloud prevented airborne search and rescue (SAR) efforts.
1.2 Aircraft Information
The accident aircraft was configured to seat the pilot plus nine passengers. Normal airspeed in cruise flight was about 130 knots. Equipment on board included the standard six flight instruments, one aviation band (VHF-AM) communications radio, one marine band (VHF-FM) radio, a portable Garmin GPSMAP 296, and a SPOT. Technical records indicate that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. No outstanding or deferred defects were noted in those records.
The weight and balance completed by the pilot indicated that the aircraft was within limits for the accident flight. However, incorrect passenger and fuel weights had been used and the pilot's weight was not included. Calculations made by investigators using correct figures indicate that, although the aircraft was within centre of gravity (C of G) limitations, it was likely about 75 pounds over maximum gross weight at take-off. However, because of the fuel consumed during the flight, it is likely that the aircraft was below its maximum gross weight at the time of the accident. Further calculations based on journey log book entries for previous flights indicate that, in 26 of the last 73 flights (36 per cent), conducted by the accident pilot and the other Vancouver-based Goose pilot, the aircraft had also been over maximum gross weight.
Pacific Coastal operates its Grumman Goose fleet under Canadian Aviation Regulations (CARs) Subpart 703, Air Taxi Operations. CARs Subpart 703 applies in respect of the operation, by a Canadian air operator in an air transport service, of a multi-engine aircraft that has a maximum take-off weight of 8618 kg (19 000 pounds) or less and a seating configuration, excluding pilot seats, of nine or less. The accident aircraft was equipped and approved for VFR flight only.
1.3 Wreckage and Impact Information
The aircraft wreckage was located at about 350 feet asl on the northeast side of an unnamed 400 foot peak, about one third of a mile south-southeast of Spyglass Hill on South Thormanby Island. The aircraft disintegrated during impact with trees and mountainside, and the fuselage was almost entirely consumed by a post-crash fire. The aircraft was carrying at least 528 litres (856 pounds) of fuel when it departed CYVR and would have had about 472 litres (766 pounds) on board when it crashed 19 minutes later, which accounts for the extensive burning of the wreckage. Burns to trees along the wreckage trail and to wreckage found well outside the aircraft's path through the trees indicated that an explosion had occurred about 400 feet after the aircraft first contacted trees. Tree and ground scars extend a further 200 feet. Measurements based on tree scars show that the aircraft was climbing between 5 and 8° on a track of about 296°T (within 12° of the track it flew after SALMON) when it first contacted trees. The upward angle of the aircraft's path through the trees remained constant for about 400 feet before decreasing along the remaining 200 feet of the wreckage trail. The wreckage was examined to the extent possible; no pre-impact mechanical failures were noted. The wingtip sponsons and wing flaps were found in the up (retracted) position, normal for cruise flight. All three blades had separated from the left propeller hub and two had separated from the right. All six propeller blades were extensively twisted, bent, scored and dented.
The emergency locator transmitter (ELT) was destroyed and no 121.5 megahertz (MHz) signal was received by overflying aircraft. The SPOT and the portable GPS were also destroyed in the crash. The aircraft was not equipped with cockpit voice or flight data recorders nor was it required to be by regulation.
High-speed impact with rugged terrain and the aircraft's consequent breakup, explosion and post-crash fire would normally have made the accident fatal for all occupants. However, one passenger was ejected from the aircraft and, although seriously injured, survived the crash and hiked for about two and one half hours to reach the island's east shore where he met ground SAR personnel.
1.4 Pilot Information
Records show that the pilot was certified and qualified for the flight in accordance with existing regulations. He was licensed to fly single- and multi-engine land and seaplanes and had accumulated about 12 000 hours of total flying time, about 8000 hours of which were in amphibious aircraft. He previously held an Australian airline transport pilot licence that included an instrument rating. He did not hold a current instrument rating nor was he required to. He had been employed as a pilot on the west coast of British Columbia for about four and one-half years.
The pilot was hired by Pacific Coastal in February 2008 to work on a seasonal basis but was upgraded to full-time status in July 2008. He had completed the company indoctrination exam on 19 February 2008, a pilot proficiency check (PPC) flight test on the Goose on 27 February 2008, and line indoctrination on 02 April 2008. Records show that controlled flight into terrain (CFIT) training was provided by the company to the pilot. On 29 August 2008, the pilot was assigned to fly the Kiewit project out of Vancouver. On the day of the accident, the pilot was working the tenth day of an 11-day rotation and had accumulated about 27 hours of flight time during those 10 days. He had flown 19 of the last 30 days. This was an exception to the normal schedule and occurred because the other Vancouver-based pilot on the Kiewit project was on vacation. The normal schedule resulted in the pilot flying about nine to thirteen days per month in rotations of two to four days at a time. However, the pilot's flight and duty time limits were not exceeded, and there were no indications of any health issues on the morning of the accident.
Pacific Coastal management had met with the pilot three times to discuss concerns they had with his decision making. The last meeting, about three months before the accident, was held because management was concerned that he was completing trips in what other pilots deemed to be adverse wind and sea conditions. The company believed that this behaviour was causing other pilots to feel pressured to fly in those conditions and was also influencing customer expectations. At least one fishing lodge owner favoured the accident pilot because he flew customers in and out when other Pacific Coastal pilots would not because they felt that the conditions were too risky.
At about 1230 on the day before the accident, the pilot of a float-equipped aircraft encountered a 400-foot ceiling and estimated 1 sm visibility near Powell River and made a precautionary landing on the water to wait out the conditions. That pilot subsequently observed a Pacific Coastal Grumman Goose fly by in these conditions. Records show that the Grumman Goose was piloted by the accident pilot.
1.5 Weather Information
One of the key challenges facing air taxi operations on the British Columbia coast is the often uncertain weather in mountainous terrain. Companies must ensure that appropriate safeguards are in place regarding weather-related decisions. This includes the decision to depart as well as how to cope with unexpected weather conditions. Regulations, company procedures, supervision, and weather information are tools to aid in the decision-making process. Pilots must ensure that their entire flight is conducted within the limits set by the company and Transport Canada (TC). Although a wide range of weather information is available to the pilot and company, at times this information is only available from sources that are separated by considerable distance along a route. As a result, the information obtained from these sources does not necessarily cover the entire route. In addition, the sources of information available are often of variable quality and conditions may change rapidly during the flight. Therefore, pilots often rely on their past experience in regions where weather information is lacking.
The company dispatch centre provides the pilots with telephones, computers and hard-copy weather packages that they receive by fax on a routine basis. These were made available to the pilot in addition to the discussion with one of the dispatchers. The pilot checked the weather via his laptop computer before leaving home but it is not known if he obtained any additional information via the telephones and computers that were available in the dispatch centre.
Weather information that was available to the pilot at the company dispatch centre before departure included:
- Weather Depiction Prognosis;
- Surface Analysis Chart;
- graphic area forecast (GFA) - Pacific region;
- local graphic forecast - Strait of Georgia;
- aerodrome forecasts (TAF) for Vancouver, Nanaimo, Comox, and Campbell River (relate to weather conditions within five miles of the centre of an airport);
- METAR and special observations (SPECI) for the above locations plus Powell River (METAR are issued hourly on the hour based upon observations taken up to six minutes before each hour. A SPECI describes changes that occur between regular observations);
- marine forecast for Pacific waters - Strait of Georgia north of Nanaimo;
- Merry Island lighthouse observation; and
- the Kiewit camp at Toba Inlet.
However, only four of these locations provided actual weather reports directly along the route:
- the Vancouver airport;
- the Merry Island lighthouse;
- the Powell River Airport; and
- the Kiewit camp at Toba Inlet.
The next closest weather reporting stations are located across the Strait of Georgia on Vancouver Island (see Figure 2).

The day before the occurrence, a warm front passed through the area of the flight. On the day of the occurrence, the warm front was lying on an east-west line north of Port Hardy, British Columbia, moving northeasterly. An area of continuous precipitation was present behind the front that extended south to the vicinity of Powell River. Warm fronts often produce a wide variety of weather and may include extensive areas of cloud and precipitation. Variations along a warm front may prohibit VFR flight in some areas while having no effect in other areas. Following the passage of a warm front, poor conditions may continue and the expected rise in temperature may also be accompanied by a rise in dewpoint, thereby prolonging the likelihood of fog.Footnote 7
The graphic area forecast (GFA) valid for the flight called for an overcast layer based at 1500 to 2000 feet asl with visibility of 6 sm or greater in mist. However, the GFA also called for extensive ceilings of 300 to 1500 feet asl with patchy areas of ¼ to 2 sm visibility in light drizzle, fog, and mist. To the northeast of the route (that is, the mainland side), forecast conditions consisted of local ceilings based at 800 feet asl with 1 sm visibility in mist.
1.6 Departure Weather
The CYVR ATIS received by the pilot just before departure reported a ceiling based at 500 feet agl with 2 sm visibility. While these conditions are below the minimum VFR criteria, they are above the minimum required for special VFR (SVFR) operation (that is, 1 sm visibility and clear of cloud) within a control zone (see Appendix A). As a result, CYVR tower approved the pilot's request for SVFR to depart the control zone. Contrary to the most recent ATIS report, the actual conditions on the river at the time of take-off were below both VFR and SVFR criteria. A photograph (see Photo 1) was taken of the aircraft as it taxied down the ramp into the river just moments before take-off. The photo shows the weather conditions in the direction of take-off. An island (bottom middle of photo) approximately 0.6 sm away is barely visible, and this visibility persisted beyond the time of take-off. A similar photo was taken on a clear day for contrast (see Photo 2 ).


The decision to depart a control zone under SVFR must account for weather requirements of the adjoining airspace. If the flight cannot maintain 300 feet agl and be clear of cloud with at least 2 sm visibility in uncontrolled airspace (twice that required inside the control zone under SVFR), a VFR pilot would be obligated to return or land.
1.7 En-Route Weather
An aerodrome forecast (TAF) is not issued for Powell River, and SVFR does not apply since it lies in uncontrolled airspace. At 0900, the reported weather at the Powell River Airport was below minimum VFR criteria for uncontrolled airspace. A SPECI issued at 0925 indicated winds of 110°T at 4 knots with 1 ½ sm visibility in mist. Cloud formed a ceiling at 400 feet agl. The temperature was 9°C and the dewpoint was 8°C. The remarks section reported that the visibility to the west was 6 sm. This SPECI showed a slight improvement since the last METAR but conditions at the airport remained below VFR minima.
The Powell River Airport is located 425 feet asl. Adding the elevation of the airport to the ceiling height can provide a rough estimate of ceiling heights above sea level. If the pilot remained over the sea, it is possible that the conditions near the Powell River Airport could have exceeded the minimum VFR criteria for uncontrolled airspace (that is, clear of cloud and at least 300 feet agl plus 2 sm visibility). The pilot had three likely sources to determine the Powell River weather while en route: radio the company base at Powell River, radio the Campbell River flight service station (FSS) for the latest information, or radio other traffic flying in the area. Investigators could not find any information to indicate that the pilot attempted to get the latest Powell River Airport weather, and there was no known VFR traffic in the area.
The Merry Island lighthouse is along the intended route about 3 miles southeast of the accident site. Weather observations are taken and reports issued every three hours. The reports are primarily intended for use by mariners, and are not certified for aviation use. However, these reports contain a supplementary section with information pertinent to pilots. The lighthouse keeper who issued the weather reports on the morning of the accident did not have instruments such as a ceilometer or weather balloon to accurately measure all the parameters contained in the report. In addition, it had been more than 10 years since the lighthouse keeper had last received any type of formal weather observer training. According to NAV CANADA, there exists no requirement for refresher training or any other type of formal weather observer training to be provided to weather observers after initial training and certification. However, NAV CANADA has an agreement in place with Environment Canada to inspect meteorological equipment and the observation program. Remedial issues regarding weather observer's performance (if any) are identified in the yearly inspection. The last inspection for this site before the accident was conducted in August 2007. No issues were identified.
The report issued for Merry Island at 0940 recorded the visibility as 2 sm in fog, even though the Environment Canada marine definition of fog implies visibility of one mile or less. Winds were from the southeast at 15 knots producing sea conditions described as a two-foot chop. The supplementary weather information recorded the temperature as 9°C, dewpoint 9°C (similar temperature and dewpoints are one of the conditions necessary for fog to form) and ceiling 600 feet overcast. Investigators found that the shoreline reference used to estimate the 600-foot ceiling was actually at an elevation of about 300 feet asl.
Visibility in Welcome Passage (the channel located immediately north of Merry Island between South Thormanby Island and the mainland) at the time of the accident was about one mile. Visibility on South Thormanby Island varied from about 100 m at sea level to about 20 m in fog at the elevation of the accident site.
The unofficial weather observation from the camp at Toba Inlet shortly after 0900 was consistent with the local graphic forecast for that area, which indicated that conditions were suitable for VFR flight at that time.
Locations (on Vancouver Island) nearest to the route included the Comox Airport, which is just above sea level and was reporting instrument meteorological conditions (IMC). It was forecast to remain in IMC except for a temporary (one hour or less) period when conditions suitable for SVFR may exist. The other pilot who routinely flew this route used the Comox weather report as an indicator of the suitability of the weather for the planned route.
The conditions at the Campbell River Airport were below SVFR minima and were forecast to remain that way for the duration of the accident flight. Like Powell River, the Campbell River Airport is a few hundred feet above sea level.
1.8 Previous Accident
On 03 August 2008, a Pacific Coastal Grumman Goose was in an accident (TSB report A08P0241). The aircraft was operating as a charter flight and departed Port Hardy Airport on a VFR flight to Chamiss Bay, British Columbia. When the aircraft did not arrive at its destination, a search was initiated. The wreckage was located on a hillside near Alice Lake, approximately 14 nm from its departure point. The aircraft had crashed into a mountainside and was destroyed. A post-crash fire occurred. Of the seven occupants, the pilot and four passengers were fatally injured, one passenger suffered serious injuries and another sustained minor injuries.
The TSB investigation found no airframe or system malfunctions before or during the flight. The investigation focused on the following causes and contributing factors: weather, decision making, aircraft performance, ELT performance, and flight-following.
In the aftermath of the 03 August 2008 accident, Pacific Coastal's own investigation resulted in safety action taken in several areas, including pilot decision making, standard operating procedures (SOPs), flight-following, training and standards, safety management system (SMS) documentation, minimum VFR limitations, and risk management processes.
1.9 Pacific Coastal Management of VFR Operations
The perspective of Pacific Coastal management on VFR flight operations was that its pilots did not have to fly in bad weather for the company to remain competitive, and this attitude was encouraged in all staff. For its CARs Subpart 703 operations, the airline operated a Type D operational control system where operational control was delegated to the pilot-in-command of a flight.Footnote 8 Under this system of self-dispatch, pilots make their own weather decisions with the aid of information provided by dispatch.
The company believed that the weather limits published in the CARs were sufficient information for their pilots to make decisions concerning flight in marginal weather conditions. The company operations manual (COM) highlighted the CARs that pertained to weather limits; however, it did not specify minimum altitudes for VFR flight until after the 03 August 2008 accident. Additionally, the COM did not outline procedures to follow in marginal weather conditions.
Air taxi operators are not required by regulation to provide Pilot Decision Making (PDM) or GPS training to VFR pilots. Subsequent to the 03 August 2008 accident, the company initiated PDM training for its VFR pilots—initially an off-the-shelf course then, later, a customised course that included peer critique of weather choices.
Consistent with the company's desire to discourage pilots from flying in bad weather, Pacific Coastal decided not to adopt an available TC reduced-visibility operations standard of 1 sm visibility in uncontrolled airspace. Pacific Coastal management believed that the reduced-visibility minima would add unwarranted risk to its existing flight operations. Operation under this standard requires a company to implement additional measures to manage the associated risks. This includes PDM training, one hour annually of basic instrument flight training, and training in low-speed manoeuvring such as low-altitude escape turns. Additionally, a GPS and other navigation equipment are required along with appropriate training in these devices and specific company procedures and standards for flying in reduced visibility.
The accident pilot's previous employer also had not adopted the reduced-visibility operations standard, and did not provide the associated training to company pilots. While employed by Pacific Coastal, the pilot had requested IFR training to enhance his ability to contend with poor weather encountered en route. Pacific Coastal management believed that such training might encourage flying in bad weather. As a result, this training was not provided to Pacific Coastal's VFR pilots.
Pilot adherence to regulations and company expectations was monitored by the Director of Flight Operations and the Chief Pilot in Vancouver and by the VFR Chief Pilot in Port Hardy. The Director of Flight Operations is responsible, among other duties, for ensuring that air operations are conducted in accordance with current regulations, standards, and air operator policy. The VFR Chief Pilot of Air Taxi Operations, based in Port Hardy, is responsible for the professional standards of the flight crews under his authority, and in particular the supervision of flight crews. However, unless a customer specifically complained about unsafe operating practices, supervisory personnel found it very difficult to assess pilot performance of single-pilot operations in Vancouver and Port Hardy. Analysis of GPS data from Pacific Coastal Goose flights before the accident showed that some flights undertaken by three other aircraft, none involving the accident pilot, were flown for extended periods below 300 feet agl.Footnote 9
From February to August 2008, the accident pilot was based in Port Hardy, where he was under the direct supervision of the VFR Chief Pilot. While at Port Hardy, he was assessed as being an experienced pilot who was not conforming to the company expectations of flying conservatively. In particular, there was concern that the accident pilot was willing to assume an unacceptable level of risk when it came to making weather-related decisions. In July 2008, the VFR Chief Pilot in Port Hardy became unable to fulfill his job functions due to a personal issue. As an interim measure, the duties of VFR Chief Pilot were performed by several of the Vancouver management staff who visited the Port Hardy office regularly. In August 2008, the accident pilot bid on and was selected to join the pilot already flying the Kiewit charter out of Vancouver. At the time, it was taken into account that there had been occasions where the accident pilot had not adhered to company norms. Management from the Port Hardy and Vancouver bases discussed their concerns with the accident pilot, and were satisfied by his response that he would conform to company expectations. No records were made of these discussions and no formal follow-up actions were put in place.
While flying out of Vancouver, the two VFR pilots were informally monitored by the Vancouver management team whose offices were adjacent to the crewing room. However, no formal reporting method was established for these pilots and neither of them attended pilot meetings in Port Hardy or Vancouver.
Following the 03 August 2008 accident, Pacific Coastal initiated a risk analysis of its VFR operations. This risk analysis was not completed because of insufficient in-house skill in formal risk analysis methodologies. Shortly after the 16 November 2008 accident, the company carried out a risk analysis that focused on the circumstances of that event. That risk analysis identified the accident as a hazard rather than a consequence.
1.10 Safety Management at Pacific Coastal
The Pacific Coastal air taxi operation is based in Port Hardy but one Goose was operated out of the main base in Vancouver to support the Kiewit camp at Toba Inlet. The Vancouver base principally supports CARs Subpart 704 (Commuter) and Subpart 705 (Airline) operations, which operate some flights under VFR but are primarily IFR operations. The accident aircraft was the only one operating exclusively under CARs Subpart 703 VFR air taxi rules out of Vancouver.
The traditional approach to safety management relies primarily on regulatory compliance and reacting to undesirable events by identifying the underlying causes and prescribing specific measures to prevent their recurrence. Modern safety management principles promote a proactive search for hazards, identification of risks and the best defences to reduce risk to an acceptable level. These principles must be embedded within an organization's management system so that safety policies, planning, procedures, and performance measurement are integrated into day-to-day operations.
The International Civil Aviation Organization (ICAO) defines a safety management system (SMS) as "an organized approach to managing safety, including the necessary organizational structures, accountabilities, policies, and procedures." Footnote 10 Under SMS, the operator is responsible for the safety of operations, and TC is responsible for regulatory oversight. SMS implementation has not been without its challenges as TC and operators continue to learn how to operate under this new system. In this environment, TC's oversight of Pacific Coastal revolved around documentation review to identify trends and/or weaknesses in the company's SMS, and verification that company processes were in place to address deficiencies.Footnote 11
As a CARs Subpart 705 operator, Pacific Coastal was required to have an SMS. Although not yet required by regulation, CARs Subpart 705 operators had been encouraged by TC to extend their SMS to aircraft deployed under other operating certificates and Pacific Coastal elected to voluntarily apply SMS to its CARs Subpart 703 and Part 704 operations as well.
Pacific Coastal's company-wide Phase 1 SMS was validated by TC in September 2005. This included the voluntary implementation of SMS for Pacific Coastal's air taxi operations. Phase 2 SMS validation was completed in July 2007 and Phase 3 SMS validation was completed in June 2008. Phase 4 SMS documentation had been submitted for review before the Process Validation conducted by TC on 21 August 2008 as a result of the 03 August 2008 Pacific Coastal accident. However, phase 4 SMS had not been validated by TC at the time of the 16 November 2008 accident. During the Process Validation, Pacific Coastal successfully demonstrated that it had a process for the reactive reporting and analysing of hazards, and a means of investigating and analyzing occurrences.
Before SMS implementation, TC's Commercial and Business Aviation (CBA) Division's Operations Sub-Division carried out oversight functions through routine monitoring (such as formal audits), inspections, PPCs, ramp inspections, in-flight inspections, and Special Purpose Inspections.Footnote 12 Special Purpose Inspections are carried out when there are significant or unusual changes in an air operator's operations. When an accident or incident occurs, the CBA manager decides on whether an investigation is required, and what type of investigation, in order to determine if there has been any regulatory violation or deficiency to prevent a recurrence of the same type of accident or incident.Footnote 13
Issues involving significant or complex safety concerns in civil aviation require the appropriate use of risk management techniques, and the proper documenting of risk decisions.Footnote 14 In response to the 03 August 2008 Goose accident, a Process Validation was convened by the Regional Director, Civil Aviation on 21 August 2008 instead of a Special Purpose Inspection that is normally carried out following a fatal accident. This decision was made because TC's overall assessment of the company at that time was that Pacific Coastal had a good safety record and was proceeding well with SMS implementation. The Process Validation was selected by TC in order to look at systems recently added to the company as a result of the phased-in SMS requirement and to confirm that the systems/components targeted were in place and were being used.
TC does not have a staff instruction for a Process Validation. However, it does have a staff instruction for a Program Validation, designed to examine effectiveness as well as compliance with regulation. TC selected a few of the elements normally reviewed during a Program Validation and applied them to the Process Validation that occurred on 21 August 2008. For example, TC assessed the company's reactive reporting process as acceptable; however, it did not verify that the company's methods suited the complexity of its organization. TC also examined the company's investigative processes, but did not apply several minimum criteria when making its assessment. The Process Validation report concluded that all regulatory expectations were met; however, it also included observations regarding the company's investigation and hazard analysis processes that Pacific Coastal should consider for enhancement. These outstanding items were considered to be pending due to ongoing work by the company. Consequently, the results of the Process Validation were deemed acceptable, with expectations noted as being met, and no findings regarding the Pacific Coastal's SMS were identified.
Following the 16 November 2008 Pacific Coastal accident, TC convened a Special Purpose Inspection on 19 November 2008 that focused on Pacific Coastal's air taxi operation. The inspection consisted of a review of regulatory compliance and the company's response to the 03 August 2008 accident. The process used was a combination of "old" and "new" regulatory oversight tools. The "old" inspection tool determined compliance with operational control and technical dispatch regulations. The "new" tool included follow-up of the company's SMS-related response to the 03 August 2008 accident. TC wanted to confirm that the company's initiatives, undertaken as a result of the 03 August 2008 accident, were still on track and that basic regulatory compliance was not being neglected due to company resources being focused on SMS activities. During this Special Purpose Inspection, TC applied several of the criteria that were not used in the 21 August 2008 Process Validation. It was noted that the company's procedures for carrying out a comprehensive investigation needed more definition, that investigation timelines had not been established, and that the staff might not have been sufficiently equipped with training and procedures to carry out a major accident investigation. None of these issues were examined in the Process Validation that occurred following the 03 August 2008 accident. TC also found that it was unclear if the company had examined supervisory and organizational factors following the 03 August 2008 accident.
1.11 Transport Canada Oversight of VFR Minima Compliance
Between November 1999 and January 2009, TC's Aviation Enforcement Section initiated 20 actions in the Pacific Region pertaining to contraventions of regulations concerning VFR Minimum Visual Meteorological Conditions.Footnote 15 Of these, no punitive actions resulted. Compliance with a regulation requires both operator acceptance of the required behaviours and effective enforcement by TC. Identifying pilots and operators that fly below VFR minima is difficult unless a customer reports an issue or a TC inspector is present when the violation occurs. In addition, TC has delegated the majority of PPC rides to approved check pilots. As a result, TC inspectors have fewer opportunities to identify such hazardous practices through regular contact with, and observation of, pilots.
Some pilots and operators challenge the interpretation of the minimum weather regulation. For example, the regulation refers to a minimum height "above ground level." Some operators assert that this does not apply in the case of floatplane flights because they operate above water. Additionally, because the regulation states that clearance must be maintained from obstacles "or" ground, it is argued that one clearance is sufficient rather than both. Finally, when flying over water, some operators contend that they are above an aerodrome and, as such, may fly for extended periods at low altitude as long as they are configured for landing. This is referred to as the infinite runway concept and, although not a factor in this accident, is often used to skirt the intent of the regulations and continue flight in conditions below legal weather minima.
Such operators have a different assessment of the risks of low flight than the regulator. For instance, some operators believe that the critical safety factor in poor weather conditions is the forward visibility rather than height above obstacles. As a result, they feel it is acceptable to fly below minimum approved operating altitudes to gain increased visibility.
These beliefs, combined with competitive pressures and the difficulty of enforcement, lead to situations where some pilots and operators are willing to take risks by flying in marginal weather conditions. Left unchecked, these practices become accepted norms and are adopted by new pilots. This has also led to a growing concern among operators that the difficulties in regulatory enforcement give an unfair advantage to operators who are willing to place the safety of their passengers at risk.
The issue of flying in poor weather conditions was noted in a 1998 TC Safety of Air Taxi Operations Task Force (SATOPS) study. The study made recommendations to improve the accident rate by identifying the culture, attitudes, problems and safety practices in air taxi operations. Several of the recommendations involved increasing TC's monitoring and enforcement. The study included the following statement:
The operating conditions on the west coast require VFR pilots to push into, through or above fog and cloud. The Task Force was told that if pilots don't operate in these conditions, the companies can't survive because these are typical coastal weather conditions. It has become an acceptable (to industry), though illegal, way of operating.Footnote 16
Another study into this issue was published by TC in 2007.Footnote 17 This report identified hazards clustered around four themes: mountainous terrain, coastal terrain, weather, and equipment. In an effort to highlight potential areas for significant safety pay-off, the report states:
The greatest gains are to be made in the area of providing better support to decision making in operational settings. For instance, self-dispatch, a common practice in the air taxi sector, leads to contact with the geographical hazards (mountainous terrain, coastal terrain, and weather), especially when the self-dispatching pilot lacks extensive experience.Footnote 18
The report also highlighted that the "geographical hazards are particularly dangerous when combined with low pilot experience, self-dispatch protocols, and less-than-stringent supervisory practices."Footnote 19 Client and business pressure were also cited as factors that further elevate risk to operations.
1.12 Development of the Route
Pacific Coastal's first flight to Toba Inlet for Kiewit was in the summer of 2007 from Powell River. At that time, Kiewit's Toba base was located on a barge adjacent to the dock at the head of the inlet.
Midwest Aviation (a division of Kiewit) carried out an initial audit of Pacific Coastal as a supplier of charter aviation services when a Powell River-to-Toba Inlet agreement was put in place. This audit checked for the presence of key factors such as a current operations manual, insurance coverage and financial stability. This was the first operation that Kiewit had carried out in its Western Canada division where such extensive air taxi services were required.
During the development of the route by Pacific Coastal and Kiewit, informal discussions were held between both companies concerning guidance on the required weather information, the need for better weather reporting, and the need for a second pilot. At the time, the route was not considered particularly risky and no special provisions were deemed necessary. As Kiewit's use of Pacific Coastal's services grew, neither company's management controls triggered a formal risk analysis of the operation.
As the passenger volume increased, the route changed and Vancouver became the base for this VFR operation to Toba Inlet. As construction of the Toba Inlet project progressed, the Kiewit camp was moved from the dock to a site 30 km up the valley, closer to the project. Before the relocation of the camp, Kiewit personnel monitored all aircraft arrivals and departures. After the camp was relocated, Kiewit personnel were briefed on the need for the camp bus driver to stay at the dock until the plane had successfully taken off in case of emergency but this practice was not consistently carried out.
There were no reliable means to obtain weather reports at the dock. Several internal requests were made to Kiewit management for a remote weather monitoring station so that pilots could directly observe the conditions at the Toba dock from the Vancouver base. These requests received approval shortly before this accident.
After the 03 August 2008 Pacific Coastal accident, Kiewit carried out a more extensive study of its transportation needs and the Pacific Coastal operation. The resulting report was reviewed over the subsequent months and no significant changes were deemed necessary.
Passenger volume on the occurrence route of 03 August 2008 grew to approximately 300 passengers per week with 2 to 3 flights per day, 7 days a week. In September 2008, Pacific Coastal added a second pilot (the accident pilot) to the route. SMS guidance material suggests a risk assessment following significant operational changes or when hazards are identified.Footnote 20 However, incremental growth in passenger volume is not identified as a trigger for a risk assessment.Footnote 21
Water aerodromes are not certified and are not subject to the same standards as airports. In the case of Toba Inlet, the aerodrome was not serviced by a qualified weather observer, there was no safety boat, and no formal means of flight watch at the dock. As a result of the potentially unique hazards at a particular water aerodrome, scheduled commercial air service is not permitted at uncertified aerodromes unless a hazard identification and risk mitigation process has been conducted by TC. Despite possessing many of the associated qualities and risks of a scheduled passenger route, the Kiewit route was considered by TC and Pacific Coastal as a charter. Had it been considered a scheduled passenger route, TC would have been required to carry out a risk assessment of the Toba Inlet aerodrome that included weather reporting, safety equipment, training of personnel, and emergency procedures.Footnote 22
Following the 16 November 2008 accident, TSB investigators conducted an informal review of the operation along this route, and identified the following hazards: single aircraft radio operation in and out of the Vancouver control zone, inadequate weather reporting at Toba Inlet, inconsistent monitoring and reporting of aircraft departures at the Toba dock, and the lack of a safety boat at the dock.
1.13 Customer Pressure
The 1998 SATOPS study also identified that customer pressure can lead pilots to attempt flights in conditions that they would otherwise view as unsafe. This pressure can be overt, in the form of specific demands from customers and threats to use other operators who may be more willing to accept the risks, or less obvious as companies and pilots try to please customers by being perceived as highly dependable.
In the case of flights for Kiewit, three types of pressure existed. Firstly, the strong desire by Kiewit employees to return home from the Toba camp placed considerable pressure on the Kiewit travel coordinator to ensure that flights met these needs and were scheduled in time to connect with flights out of Vancouver. At times, the travel coordinator directed this pressure to Pacific Coastal, as seen by attempts to hire another operator to complete when Pacific Coastal would not due to concerns about the weather. Secondly, Pacific Coastal employees were aware that Kiewit operations might be affected if key employees or parts did not arrive on time. Thirdly, the pilots might have felt pressure to keep the customer happy.
Before the 16 November 2008 accident, the Kiewit travel coordinator had requested a different airline after Pacific Coastal had cancelled a second flight into Toba due to unsafe weather conditions encountered during the previous flight. Pacific Coastal management communicated the need for Kiewit to provide counselling to the travel coordinator concerning the importance of respecting a pilot's decisions about weather and this issue was documented in the Kiewit audit. Despite these efforts, similar pressure was applied to another operator following the accident.
The TSB investigation did not identify any overt pressure on the accident pilot to fly, by either Pacific Coastal or Kiewit, on the day of the accident.
Recognizing the role that customers can play in aviation safety, the United States Federal Aviation Administration initiated a customer education program to improve flight safety in Alaska.Footnote 23 This program educates passengers on the dangers of pressuring pilots to fly in poor weather, and also encourages them to report operators that unnecessarily push the weather. Currently, there is no education program in Canada to ensure that the public is aware of VFR flight regulations, or the actions to take if they have a concern.
1.14 Communications
On the day of the accident, radio communication between Vancouver ATC and the accident aircraft was normal. Aircraft operating within the Vancouver control zone are required to communicate with and monitor ATC on an aviation band radio. The aircraft's single aviation band radio could be used for this purpose or used to communicate with other aircraft, Pacific Coastal's Vancouver dispatch centre, and some company bases such as Powell River. The aircraft was also equipped with a marine band radio, which could be used for communication with the company's Port Hardy dispatch centre and with some customer bases but could not be used to communicate with ATC, non-company aircraft, or the company's Vancouver dispatch centre.
On the morning of the accident, Pacific Coastal Vancouver dispatch was unable to contact the pilot to inform him that the weather at Powell River had deteriorated.
1.15 Dispatch and Flight-Following
Pacific Coastal conducted VFR air taxi operations under the self-dispatch system (that is, Type D) and pilots were the sole decision makers as to whether they would conduct a flight or not. Pacific Coastal's Type A dispatch system for its airline (CARs Subpart 705) operations gave the dispatchers co-authority for departure decisions. The TC Special Purpose Inspection concluded that Type D self-dispatch was sufficient for VFR air taxi operations.
Because of delays in initiating SAR operations and finding the accident site after the 03 August 2008 accident, Pacific Coastal expedited the temporary installation of personal satellite trackers (that is, the SPOT Satellite Messenger) in all VFR aircraft. SPOT uses commercial satellites to transmit a GPS position and rudimentary, pre-programmed status messages. If a user subscribes to the real-time tracker feature, the system can be programmed to send a GPS position report every 10 minutes to pre-determined recipients. Designated personnel can access the SPOT website, via a password-protected login, and see the position reports on a digital map. SPOT is capable of sending an intentional emergency signal but, unlike an ELT, the unit is not designed to provide an automatic alert message in the event of an accident.
Despite dispatchers initially consulting the wrong SPOT Satellite Messenger data, the search area was reduced as was the time required for SAR personnel to locate the injured survivor and the accident site.
1.16 Decision Making
Pilot decision making (PDM) is critical to flight safety. PDM can be defined as a four-step sequence: the gathering of information, the processing of that information, making a decision based on possible options, and then acting on that decision.Footnote 24 Once a decision has been implemented, the process starts over again as the individual now gathers information to monitor the effectiveness of the decision. Based on how that information is processed, the individual then continues through the rest of the process, and so on.
Each stage in the four-step PDM process is susceptible to error. During the information gathering step, misdirected attention can cause critical cues to go undetected. In addition, biases may prevent a pilot from recognizing cues that are different from those expected. The processing of information stage will introduce errors into the PDM process if the information is incorrect, distorted, incomplete, or misinterpreted. The assessment of the available options involves a subjective risk assessment based on experience and knowledge. Pilots usually decide on the option they perceive as most likely to result in the best outcome given their goals. The last step in the process is to implement the option that has been selected as the most appropriate. Errors at this step of the process are typically the result of implementing an inappropriate response or improperly carrying out the correct action.
Pilots' decisions can be influenced by a wide range of factors such as perception of the situation, experience, training, abilities, expectations, goals and objectives, organizational and social pressure, time-criticality and contextual elements. A VFR pilot's decisions are largely influenced by the assessment of existing weather information, the availability of additional navigational aids, and previous experience with a route. Once a decision is made to depart or continue along a route, pilots have a tendency to continue with the selected course of action unless there are compelling reasons not to do so. Additionally, pilots often seek out elements that reinforce, not contradict, the decision made (that is, confirmation bias).Footnote 25 Successful experience under similar circumstances can make pilots very reluctant to select a different course of action. If a pilot is suddenly faced with additional unexpected cues from the environment, there is a danger that the relevant cues go unnoticed.Footnote 26 This can occur due to mental processing limitations as information competes for a pilot's attention. Relevant cues can also be missed by a pilot if they are deemed less important than others, leading a pilot to focus on cues that may erroneously support the pilot's preferred course of action. In this occurrence, the pilot's safety significant decisions were the decision to take off and the decision to continue the flight into adverse weather conditions.
1.17 VFR-into-Instrument Meteorological Conditions Accidents
TSB data show that continued VFR flight into adverse weather represents a significant threat to aviation safety. While VFR-into-IMC accidents account for a relatively small portion (less than 10 per cent) of all reported accidents, approximately 55 per cent of those VFR-into-IMC accidents were fatal, compared to 10 per cent of all other accidents. An enormous amount of research and many studies have been conducted to identify the causes of continued VFR-into-IMC accidents. Some of the main causes of these accidents are as follows:
- VFR pilots can be overly optimistic on the probability of having to fly from VFR-into-IMC, and on their own abilities to fly out of IMC if encountered (ability bias);Footnote 27
- Incorrect situational assessment can cause pilots to prolong flight into deteriorating weather because they do not realize that they are doing so;Footnote 28
- Decision framing can play a role. If pilots frame their decisions in terms of potential losses (that is, revenue, etc.), they are more likely to prolong flight into deteriorating weather;Footnote 29
- Pilots are motivated to complete their flights;Footnote 30 and
- Pilots may exhibit greater risk-taking behaviour as more time and effort is invested in a flight.
1.18 Global Positioning System (GPS)
Pacific Coastal equipped each of its amphibious aircraft, including the accident aircraft, with a portable Garmin GPSMAP 296. Pacific Coastal did not, and was not required to, provide its VFR pilots with GPS training nor assess them for GPS proficiency. VFR pilots are only required to receive GPS training if the company is operating as per the TC reduced visibility operations standard. Also, in part, training was not provided because several of the pilots were already familiar with GPS usage and the new units were perceived as easy to operate. Pacific Coastal expected that the GPS was to be used as an aid to visual navigation but not as a primary means of navigation. This policy is consistent with the guidance provided in the Aeronautical Information Manual (AIM), which stipulates in part "VFR receivers, such as hand-held GPSs, may be used to supplement map reading in visual conditions, but are not to be used as a replacement for current charts." Footnote 31
A GPS or equivalent area navigation system was required on the Vancouver-based aircraft to navigate to call-up/check-points such as SALMON. Despite the low visibility and significant wind, radar data show that the aircraft made only one minor course correction after passing by SALMON and then flew a nearly straight track to the accident site. This is consistent with the use of GPS for navigation.
The GPSMAP 296 can provide automatic warning of obstacles and terrain within 100 vertical feet of the aircraft through a separate window that occupies about 1/6 of the screen. This feature is automatically activated upon power-up, requiring the pilot to acknowledge each warning when it appears. This feature can also be de-activated, via a user options menu, if the pilot does not want the warnings to appear. It is common practice to select the terrain warnings off if the flight is conducted at a low altitude. The accident aircraft's GPS was not recovered, so it was not possible to determine the settings at the time of the accident. However, given the altitude of the accident flight, if the GPS was functional and if the terrain and obstacles alert was in the active mode, it would have displayed a terrain and obstacle alert almost continuously.
In March 2010, the TSB released its Watchlist identifying the safety issues investigated by the TSB that pose the greatest risk to Canadians. In each case, actions taken to date are inadequate and concrete steps must be taken on the part of industry and the regulator to eliminate these risks. One of the safety issues identified in the Watchlist is collisions with land and water.Footnote 32
Collision with land and water occurs when an airworthy aircraft under the control of the pilot is inadvertently flown into the ground, water, or an obstacle. In these cases, pilots are unaware of the danger until it is too late. This type of accident often happens when visibility is low, at night, or during poor weather. Such conditions reduce a pilot's situational awareness of surroundings and make it difficult to tell whether the aircraft is too close to the ground. The risk is even greater for small aircraft, which venture further into remote wilderness or into mountainous terrain but are not required to have the same ground proximity warning equipment as large airliners.
Between 2000 and 2009, there have been 129 accidents of this type in Canada, resulting in 128 fatalities. Collisions with land and water account for 5 per cent of accidents but nearly 25 per cent of all fatalities. The TSB has investigated numerous collisions with land and waterFootnote 33 and has identified deficiencies, made findings, and issued recommendations such as installing ground proximity warning systems in smaller aircraft.
2.0 Analysis
2.1 Introduction
There were some similarities between this accident and the previous accident in the causes and contributing factors. The company initiated several safety actions as a result of the 03 August 2008 accident; however, several of those actions were not fully implemented when the 16 November 2008 accident occurred. For instance, while the company had carried out a first round of PDM training, the planned second round of training that was focused on decision making in poor weather conditions had not been carried out.
Examination of the aircraft wreckage maintenance records indicated that the aircraft was airworthy at the time of the accident. The analysis will focus on the decisions made by the pilot to depart, to continue in unfavourable conditions, and the consequent flight into terrain. Factors that affected this decision making, such as weather data, dispatch, company supervision, route development, and oversight by TC will be analysed to identity underlying causes.
2.2 Weather
Given the conditions at take-off and at the accident site, as well as the forecast and reported conditions for the en route section, it is likely that most of the flight was conducted below the required VFR minima. The conditions present on the day of the occurrence would have resulted in a high likelihood that IMC conditions would be encountered. The visibility portrayed in the photograph as the aircraft taxied into the river at Vancouver (see Photo 1) displays conditions below SVFR minima for fixed-wing aircraft.
The supplementary report from the Merry Island lighthouse indicated marginal visual meteorological conditions (VMC). Lighthouse reports have traditionally provided VFR pilots on the coast with a valuable resource; however, in this case, the report was inaccurate. This may have contributed to the pilot's conclusion that weather along the route was acceptable.
2.3 Pilot Decision to Depart
During his pre-flight briefing, the pilot advised the passengers that the flight would be conducted at low altitude and that, if they were concerned, they could deplane. This is not a normal part of the pre-flight briefing and indicates that the pilot was aware that the weather along the route was likely to be poor enough that, in order to maintain ground reference, the flight would have to be conducted at a lower altitude. However, the SPECI issued at 0925 for Powell River showed a marginal improvement that the pilot could have interpreted as the beginning of a trend. This is inherently risky because a single weather report does not confirm that a trend has commenced. Although the large majority of weather information indicated low cloud and poor visibility along the route, the marginal improvement at Powell River and inaccurate information from Merry Island may have contributed to the pilot's decision that weather along the route would be sufficient for a low-level VFR flight.
The pilot's commitment to the decision to depart would have increased after boarding passengers, loading baggage, and starting the engines. Once ATC approved the pilot's request for SVFR, the onus fell on the pilot to ensure that weather outside of the control zone would permit continued flight under VFR. When departing under SVFR, VFR pilots must have an alternate plan if below-VFR weather conditions are encountered when they leave a control zone. The pilot did not request the latest available weather reports (actual weather at 1000) to determine if the weather along the planned flight route was indeed improving. Had this been done, the deteriorating weather in Powell River would have given the pilot the opportunity to reconsider his decision to depart. When the aircraft departed, the visibility on the river was little more than ½ sm.
There are indications that the accident pilot had a tendency to push the weather. For instance, the day prior, the pilot was flying in below-VFR conditions. The pilot's decision to depart was likely affected by confidence gained through previous successes under similar conditions.
The investigation did not find any indication of pressure to depart from any passengers, Pacific Coastal, or Kiewit on the day of the accident. However, the physical presence of passengers can inherently create indirect pressure on a pilot to continue with his decision to depart, particularly when all are seated in the aircraft and are ready to go as was the case on this day.
2.4 Pilot Decision to Continue Flight
Once airborne, the options available to the pilot were to continue on the planned route, alter the route, return to CYVR, divert to another aerodrome, or land on the water. All these options involved risks. Since he had been navigating from SALMON using GPS, he likely relied heavily on the GPS for navigation in the absence of adequate visual cues. As he approached Thormanby Island, it is highly likely that the pilot expected that he would regain adequate visual reference with the ground. However, it is difficult to accurately assess visibility over a featureless water surface, and it likely was not apparent to the pilot that the visibility had become so poor that a change of plan was required. When the pilot finally sighted Thormanby Island, the aircraft was too close for the pilot to be able to avoid colliding with terrain.
Several of the factors that influence a pilot's decision to continue flight from VFR into IMC existed in this accident: previous successes in low visibility, difficulty in assessing actual visibility, commitment to a chosen course of action, the consequences of changing the chosen course of action, and ability bias.
It is likely that one or more of these factors were contributory to this accident.
2.5 Controlled Flight into Terrain (CFIT)
The accident flight was conducted in meteorological conditions below VFR minima. There is no indication that the pilot attempted to land on the water, or to turn around, in the face of extremely low visibility and ceilings. It is highly likely that the pilot was relying on the GPS for navigation and that, as he approached Thormanby Island, his attention shifted from the GPS to looking outside the aircraft. While flying in fog, a CFIT occurred during an attempt to avoid terrain. No evidence was found to indicate that the aircraft was out of control before impact.
Damage to the aircraft and to the trees at the accident site indicated the aircraft's speed and attitude immediately before impact. The long, straight, rising angle of the swath cut through the trees and the extreme damage to those trees and to the aircraft indicate that the aircraft was flying at relatively high speed and climbing rapidly before collision with terrain. Extreme damage to all the propeller blades indicates that high engine power was being developed. This combination indicates that the pilot reacted to sighting terrain seconds before impact and pulled the aircraft up into a rapid climb. However, the pull-up was initiated too late to out-climb the rising terrain that lay ahead. The wind recorded at Merry Island half an hour before the accident would have resulted in a 15-knot tailwind. Operating at cruise speed, the aircraft would have had an approximate ground speed of 145 knots. Given the 5° to 8° angle of climb, the aircraft's rate of climb would have been between 1300 and 2000 feet per minute, greater than can be sustained by the aircraft as loaded at the time of the accident.
The accident aircraft's flight at high speed while at low altitude and in low visibility entailed significant risks. These include: decreasing the available time to plan and react to an emergency, limiting the available options in the event of an emergency, increasing the likelihood of inadvertent descent into water or ground — particularly during a manoeuvre such as turning around — and increasing the likelihood of collision with ground-based obstacles and birds.
Following a previous CFIT occurrence,Footnote 34 in 1995, the TSB issued Recommendation A95-10, which read as follows:
The Department of Transport require the installation of GPWS on all turbine-powered, IFR-approved, commuter and airline aircraft capable of carrying 10 or more passengers.
Transportation Safety Recommendation A95-10 (issued March 1995)
TC's initial response (14 June 1995) was to refer the TSB's Recommendation to the Canadian Aviation Regulation Advisory Council (CARAC), Part VII Technical Committee for analysis. As TC did not indicate a position on the recommendation, TC's response was assessed as Unsatisfactory. In a December 2005 response to the TSB, TC indicated that a Notice of Proposed Amendment (NPA) for Terrain Awareness Warning Systems (TAWS)Footnote 35 had been presented to the CARAC in June 2003, which would require Class B TAWS installations on air taxi (CARs Subpart 703) and commuter (CARs Subpart 704) aeroplanes when configured between 6 and 9 passenger seats, regardless of power-plant type. In addition, any commuter (CARs Subpart 704) aeroplanes configured with more than 10 passenger seats would require Class A TAWS and a Terrain Awareness Display (TAD)Footnote 36 and aeroplanes in airline (CARs Subpart 705) operations would require a Class A TAWS and a TAD. In the package of proposed new regulations, there are also regulations under CARs Subpart 605 requiring turbine-powered aeroplanes configured with more than 6 passenger seats to be equipped with Class B TAWS. As a result of this action, the TSB's assessment of TC's response was changed to Satisfactory Intent. At the time of writing, the proposed regulations were still in the CARAC process and had not been put into effect. The TSB will continue to monitor TC's activity with respect to the risks associated with Recommendation A95-10.
2.6 Global Positioning System (GPS)
The aircraft's track towards SALMON and the subsequent turn towards Powell River indicate that the GPS was functioning properly. The availability of a GPS most likely influenced the pilot's decision to depart for SALMON. Further, following this decision, the GPS was then used to navigate without reference to the shoreline in below-VFR conditions as the aircraft approached Thormanby Island. This over-reliance on GPS for VFR navigation in low-visibility conditions likely made it very difficult, if not impossible, for the pilot to regain the necessary cues to continue visual flight.
Given the aircraft's planned route, it is likely that the terrain and obstacle warning was de activated before departure. If the warning had been left active, the GPS would have displayed continuous warnings that the pilot would have had to acknowledge (that is, cancel the warning).
Pacific Coastal's VFR pilots did not receive training in the operation of GPS and no baseline was established to measure their proficiency. Consequently, they also did not receive training in the risks of using GPS as the primary means of navigation, for instance attempting to navigate using GPS in low-visibility conditions.
2.7 Emergency Locator Transmitter (ELT)
The aircraft's ELT was destroyed during the impact and post-crash fire. Consequently, the ELT did not provide an alert that a crash had occurred nor did it assist in locating the accident site or the survivor. TSB Aviation Safety Advisory A08P0241-D1-A1 refers to the extremely high percentage of ELT failures (including TSB report A08P0241 on the 03 August 2008 accident also involving a Goose operated by Pacific Coastal) and also discusses alternatives to ELTs such as flight-following systems. TC is proposing that the existing regulations for ELTs be changed to require that all aircraft operated in Canada be equipped with ELTs that can broadcast simultaneously on 406 MHz and 121.5 MHz, or be equipped with an alternate means of emergency location that meets the performance standards of the satellite system/406 MHz ELTs.Footnote 37
Because the aircraft's ELT failed to operate after the crash, determining that a crash had occurred and locating the aircraft were delayed.
2.8 Communications
Radio communication between the aircraft, company dispatch and ATC was normal during the first several minutes of the flight, indicating that the pilot's radio was functioning properly. While within the CYVR control zone, the accident pilot would have been monitoring ATC. Once outside the control zone, the radio was likely selected to an en route frequency to monitor other traffic. It is also possible that, once outside the control zone, the radio was selected to the company frequency.
Pacific Coastal's dispatchers attempted to contact the pilot to pass along critical weather information to help make the decision whether to continue flight or to turn around. However, they were unable to establish contact with the pilot. Equipped with only one VHF aviation radio, the pilot would not have been able to monitor the en route frequency and Pacific Coastal's dispatch centre at the same time. It is possible that the pilot was monitoring an ATC or en route frequency when dispatchers attempted to contact him. However, it is also possible that the accident pilot was monitoring the company dispatch centre, but was out of VHF radio range due to the low altitude at which the flight was being conducted.
2.9 Weight and Balance
Although the aircraft departed Vancouver slightly over gross weight, it was within limits at the time of the accident. As a result, it is unlikely that the aircraft's weight contributed to this accident. However, weight and balance calculation errors on this and previous flights on the Toba Inlet route increased risk levels by operating outside approved limits.
2.10 Pacific Coastal Management of VFR Operations for this Route
While pilots are responsible for knowing the relevant regulations, company managers have a responsibility to set company and route specific standards and to ensure that flights are conducted accordingly.
The company philosophy was that pilots should not fly in marginal VFR weather; however, managers did not provide explicit procedures to ensure adherence. In addition, the company decided not to provide minimal IFR training to pilots, believing that it might cause them to push the weather due to an increased sense of confidence flying on instruments. IFR training increases the likelihood of a safe return to VMC if IMC conditions are inadvertently encountered.
Creating records of hazards, risks and mitigating actions is a cornerstone of any SMS. This allows actions to be tracked and trends to be identified. While Pacific Coastal management had held discussions with the pilot regarding his weather-related decision making, no formal safety management documentation existed. As a result, no formal risk analysis processes were initiated to define and mitigate the associated level of risk.
2.11 Dispatch and Flight-Following
The Type D self-dispatch system, used by Pacific Coastal, relied on the pilot for operational decisions. Aside from the CARs, there were no company procedures or decision aids (that is, decision tree, second pilot input, or dispatcher co-authority) to help the pilot decide whether or not to depart. This left flights exposed to risk, particularly if peers or management did not provide an additional defence against risky decisions because they were either not present or not aware of the pilot's intentions. Without adequate checks and balances to help ensure good decisions, this system left the pilot to make decisions subject to his own pressures, biases and risk tolerance.
Following the 03 August 2008 accident, Pacific Coastal recognized the need to supplement its existing flight-following procedures and ELT equipment. This was done in an effort to effectively track aircraft and, in the case of an accident, reduce the time for SAR operations. Pacific Coastal decided to use SPOT as an interim measure. The SPOT Satellite Messenger data transmitted before the crash helped narrow down the search area and reduced the search time required to find the aircraft. The fact that the wrong SPOT Satellite Messenger data were consulted caused an initial delay in reporting the missing aircraft.
2.12 Development of Route
The initial flights by Pacific Coastal in support of the Kiewit project were irregular charters with a low volume of passengers. Initial route assessments by Pacific Coastal and Kiewit did not identify any unusual hazards—there was no need to climb over terrain (that is, the flight remained largely over water), and landing at the Toba Inlet dock was viewed as relatively straightforward. Over two years, passenger volume gradually increased to about 300 passengers per week. A second pilot was added to the Vancouver operation to keep up with the demands of the project.
Without specific triggers to identify this type of growth, incremental changes in risk exposure may not be evident and a risk analysis not conducted. TC's guidance on risk assessment does not identify incremental operational growth as a potential hazard. The increased risk associated with the growth of the operation went largely undetected by Pacific Coastal and Kiewit.
The Toba Inlet route was conducted as an unscheduled commercial air service to an uncertified aerodrome. Had this route been considered a scheduled commercial air service, it would have been subject to an increased level of regulatory oversight. In particular, TC would have been required to carry out an on-site inspection of an uncertified aerodrome such as Toba Inlet to ensure an "equivalent level of safety"Footnote 38 to a certified aerodrome. Instead, the onus was on the operator to assess potential hazards and mitigate risk to an acceptable level. This means that there is an increased risk for high-volume charter flights at uncertified aerodromes.
2.13 Customer Pressure
Kiewit had previously applied pressure to complete the flights by pursuing other operators when Pacific Coastal cancelled flights due to weather. This practice continued after the 16 November 2008 accident on Thormanby Island and can greatly influence pilot and operator decision-making processes.
2.14 Transport Canada Oversight of VFR Minima Compliance
Some operators continue to carry out operations below VFR minima because they believe that they can safely operate below the regulated minima and that there is commercial pressure to continue doing so. VFR minima have been established because they are considered by the regulator to be the minimum safe limits. Risk increases significantly when pilots decide to accept poorer conditions rather than turn back. Despite this increased risk, some pilots practice the technique of continuing to fly, often for miles, at a reduced speed in a landing configuration rather than deciding to turn back or land once it is apparent that VFR limits cannot be maintained. This so-called infinite runway concept demonstrates faulty decision making. This represents a very dangerous situation because the concern then becomes how much additional risk the pilot will accept on his own, and what needs to happen for the pilot to take appropriate action.
TC is aware that some operators and pilots are willing to accept increased risk levels by intentionally skirting regulations. Some operators and pilots continue to interpret the regulations in favour of operating a flight in unsafe conditions rather than lose the revenue to a competitor. Ten years after the SATOPS study, these infractions continue within the air taxi industry for the same reasons cited in the study and continue to result in unacceptable risk and loss of life. Clear and enforceable regulations help maintain a level playing field within the industry by discouraging deviation from regulation. The current situation may lead some operators to accept reduced safety margins to remain competitive.
2.15 Safety Management at Pacific Coastal
The Special Purpose Inspection conducted following the 16 November 2008 accident identified SMS deficiencies that went undetected by the Process Validation. Deficiencies related to the skills of Pacific Coastal's own investigators, the company's ability to identify supervisory and organizational factors, and the lack of processes to ensure the timely implementation of safety actions placed the company at increased risk.
The following TSB Laboratory reports were completed:
- LP 158/2008 – GPS Analysis
- LP 025/2009 – Flight Instruments Analysis
These reports are available from the Transportation Safety Board of Canada upon request.
3.0 Conclusions
3.1 Findings as to Causes and Contributing Factors
- The pilot likely departed and continued flight in conditions that were below visual flight rules (VFR) weather minima.
- The pilot continued his VFR flight into instrument meteorological conditions (IMC), and did not recognize his proximity to terrain until seconds before colliding with Thormanby Island, British Columbia.
- The indication of a marginal weather improvement at Powell River, British Columbia, and incorrect information from Merry Island, British Columbia, may have contributed to the pilot's conclusion that weather along the route would be sufficient for a low-level flight.
3.2 Findings as to Risk
- The reliance on a single VHF-AM radio for commercial operations, particularly in congested airspace, increases the risk that important information is not received.
- Flights conducted at low altitude greatly decrease VHF radio reception range, making it difficult to obtain route-related information that could affect safety.
- The lack of pilot decision making (PDM) training for VFR air taxi operators exposes pilots and passengers to increased risk when faced with adverse weather conditions.
- Some operators and pilots intentionally skirt VFR weather minima, which increases risk to passengers and pilots travelling on air taxi aircraft in adverse weather conditions.
- Customers who apply pressure to complete flights despite adverse weather can negatively influence pilot and operator decisions.
- Incremental growth in Pacific Coastal's support to Kiewit did not trigger further risk analysis by either company. As a result, pilots and passengers were exposed to increased risks that went undetected.
- Transport Canada's guidance on risk assessment does not address incremental growth for air operators. As a result, there is increased risk that operators will not conduct the appropriate risk analysis as their operation grows.
- Previous discussions between Pacific Coastal and the pilot about his weather decision making were not documented under the company's safety management system (SMS). If hazards are not documented, a formal risk analysis may not be prompted to define and mitigate the risk.
- There were no company procedures or decision aids (that is, decision tree, second pilot input, dispatcher co-authority) in place to augment a pilot's decision to depart.
- Because the aircraft's emergency locator transmitter (ELT) failed to operate after the crash, determining that a crash had occurred and locating the aircraft were delayed.
- On a number of flights, pilots on the Vancouver-Toba Inlet route, British Columbia, departed over maximum gross weight due to incorrectly calculated weight and balances. Risks to pilots and passengers are increased when the aircraft is operating outside approved limits.
- The over-reliance on global positioning system (GPS) in conditions of low visibility and ceilings presents a significant safety risk to pilots and passengers.
3.3 Other Finding
- The SPOT Satellite Messenger data transmitted before the crash helped to narrow the search area and reduce the search time to find the aircraft. The fact that the wrong data were consulted caused an initial delay in reporting the missing aircraft.
4.0 Safety Action
4.1 Action Taken
Immediately following the accident, Pacific Coastal suspended air taxi operations and implemented several actions to reduce risk before resuming operations. Since then, the company has implemented several other voluntary safety actions that exceed Transport Canada's (TC) requirements for visual flight rules (VFR) air taxi operations. These additional safety actions include:
- Raising the minimum departure visibility from the TC-regulated 2 statute miles (sm) to a company limit of 3 sm from a base of operations for VFR aircraft.
- Providing a pilot decision making (PDM) course, including how global positioning system (GPS) affects decision making, to all the VFR floatplane pilots and adding PDM training to the company VFR training syllabus.
- Implementing a dispatch procedure that gives the dispatcher/flight-follower co-authority over the release of the aircraft.
- Conducting risk assessments of VFR routes and operations (including reviewing weather, wind, and water condition limitations) and developing a destination-specific risk rating system.
- Conducting line checks at least three times a year on each VFR pilot.
- Regularly monitoring the stored data of the GPS carried on the aircraft to ensure that pilots are flying within company and Canadian Aviation Regulations (CARs) limits.
- Installing aviation-specific satellite tracking systems in all VFR aircraft to replace the SPOT satellite messengers previously installed in those aircraft and eliminate the need to monitor GPS data.
- Conducting annual company culture surveys to identify areas needing improvement.
- Providing accident investigation training for key company personnel.
- Revising the company's safety management system (SMS) manual to include revised risk assessment procedures and accident investigation training.
- Having pilots and dispatchers document circumstances where poor weather affects a flight and using those data for track monitoring and to determine risk exposure over an extended period.
In December 2009, after completion of the Safety Study on Risk Profiling the Air Taxi Sector in Canada, TC developed a Pilot Decision Making Simulator to allow people to practice aviation-related decision making in a low-risk environment. The simulator can be found on TC's website at http://www.tc.gc.ca/civilaviation/regserv/safetyintelligence/airtaxistudy/simulation/menu.htm (website address confirmed accessible as of report release date).
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
Appendix A - VFR Weather Minima
As per the Canadian Aviation Regulations (CARs), the applicable visual flight rules (VFR) weather minima are as follows:
| AIRSPACE | FLIGHT VISIBILITY | DISTANCE FROM CLOUD | DISTANCE ABOVE GROUND LEVEL | |
|---|---|---|---|---|
| Control Zones | VFR | Not less than 3 miles | Horizontally: 1 mile Vertically: 500 feet | Vertically: 500 feet |
| Control Zones | SVFR | Not less than 1 mile | Clear of Cloud | n/a |
| Uncontrolled Airspace | 1000 feet agl or above | Not less than 1 mile (day) | Horizontally: 2000 feet Vertically: 500 feet | 1000 feet agl |
| Uncontrolled Airspace | Below 1000 feet agl – fixed wing | Not less than 2 miles (day) | Clear of Cloud | Vertically or horizontally: 300 feet ** |
| ** Criteria in this box applicable to CARs Section 703.27 fixed-wing operators | ||||
Appendix B – Glossary
- AARM
- Aerodrome Safety Branch (Transport Canada)
- agl
- above ground level
- AIM
- Aeronautical Information Manual
- asl
- above sea level
- ATC
- air traffic control
- ATIS
- automatic terminal information service
- CAM9
- Vancouver International Water Aerodrome
- CARAC
- Canadian Aviation Regulation Advisory Council
- CARs
- Canadian Aviation Regulations
- CBA
- Commercial and Business Aviation (Transport Canada)
- CFIT
- controlled flight into terrain
- C of G
- centre of gravity
- COM
- company operations manual
- CYPW
- Powell River Airport
- CYVR
- Vancouver International Airport
- ELT
- emergency locator transmitter
- ETA
- estimated time of arrival
- FSS
- flight service station
- GFA
- graphic area forecast
- GPS
- global positioning system
- ICAO
- International Civil Aviation Organization
- IFR
- instrument flight rules
- IMC
- instrument meteorological conditions
- JRCC
- Joint Rescue Coordination Centre
- Kiewit
- Peter Kiewit Sons Co.
- km
- kilometres
- m
- metres
- METAR
- aviation routine weather report
- MHz
- megahertz
- nm
- nautical miles
- NPA
- Notice of Proposed Amendment
- Pacific Coastal
- Pacific Coastal Airlines
- PDM
- pilot decision making
- PPC
- pilot proficiency check
- SAR
- search and rescue
- SATOPS
- Safety of Air Taxi Operations Task Force
- sm
- statute miles
- SMS
- safety management system
- SOPs
- standard operating procedures
- SPECI
- special observations
- SPOT
- SPOT Satellite Messenger
- SVFR
- special visual flight rules
- TAD
- Terrain Awareness Display
- TAF
- aerodrome forecast
- TAWS
- Terrain Awareness Warning Systems
- TC
- Transport Canada
- TP
- Transport Canada publication
- TSB
- Transportation Safety Board of Canada
- VFR
- visual flight rules
- VHF
- very high frequency
- VHF-AM
- aviation band radio
- VHF-FM
- marine band radio
- VMC
- visual meteorological conditions
- °
- degrees
- °C
- degrees Celsius
- °E
- degrees east
- °T
- degrees true