Loss of Control and Collision with Terrain
Bede BD5-J C-GBDV
Ottawa/Carp, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The pilot of the privately owned Bede BD5-J aircraft (registration C-GBDV, serial number 4672) departed the Ottawa/Carp Airport, Ontario, at approximately 1205 eastern daylight time to practice his routine for the air show scheduled for the following two days. At approximately 1210, the pilot radioed that he was starting his final fly-past before landing. The routine for this low-speed fly-past called for a number of quick extensions and retractions of the aircraft's landing gear while at a height about 500 feet above ground level. After several cycles of the landing gear, and while the landing gear was extended, the aircraft rolled sharply to the right. The nose dropped, and the aircraft descended rapidly and hit the ground. The aircraft was substantially damaged, and the pilot sustained fatal injuries.
Factual information
The accident occurred at about 1213 eastern daylight time,Footnote 1 in visual meteorological conditions.
The pilot held a valid commercial pilot licence (aeroplane). As of June 2006, he had accumulated approximately 350 total flying hours of which 44 hours were on the BD5-J. The pilot had also completed aerobatic training in 2004 and successfully passed a re-evaluation on 09 June 2005.
An amateur video of the occurrence flight was available. The video indicated that the engine was running and producing power before impact, and that the landing gear was down when the aircraft began the roll to the right. There were approximately three seconds from the beginning of the roll to when the aircraft struck the ground. The video also showed that the ailerons were deflected to counteract the right roll, but with no apparent effect.
The BD5 was originally designed by Bede Aircraft Incorporated in the early 1970s as a day visual flight rules (VFR) aircraft for use in sport and recreational flying. The aircraft had a limited aerobatic capability. It was sold as a kit plane to be built by the purchaser and was classified as an amateur-built aircraft. The original design incorporated a pusher propeller driven by a piston engine. Some of the original aircraft were later modified to incorporate a turbine-driven propeller (turboprop), and others were modified to use a turbojet engine.
The turbojet version of the aircraft, the BD5-J, incorporated a Microturbo Model TRS18-046-01 engine. At the time of the occurrence, there were only five other BD5-J aircraft in existence. It is not known how many BD5 aircraft were built, but approximately 5000 kits were sold, and there are an estimated 150 airworthy BD5 aircraft worldwide.
The kit for the occurrence aircraft was purchased by the accident pilot as a BD5-B piston-engine aircraft, and the pilot converted the aircraft during construction to a BD5-J with limited assistance from BD Micro Technologies. Construction was completed in 2002, and the aircraft had accumulated approximately 44 hours of total time before the occurrence. The aircraft was maintained by the pilot in accordance with Canadian Aviation Regulations (CARs) Standard 625, Appendices B and C. The last recorded maintenance was the annual inspection completed on 03 January 2006. No defects were identified. Seven flights were completed after the annual inspection and before the accident flight. No defects were recorded in the aircraft's journey logbook.
The pilot transported the aircraft to air shows in a custom-built trailer. The wings, flight controls and fuel system of the aircraft were designed with quick disconnects to facilitate disassembly for transport. The wing spar is tubular and consists of three parts that fit together. There is one tubular spar in each wing and one tubular centre section spar in the fuselage. To ensure a tight fit, the outer diameter of the centre section spar is slightly smaller than the inner diameter of the wing spars.
The wings are installed by sliding the outer wing spar tubes over the centre section spar tube using a ratchet mechanism that is a permanent part of the centre section spar. After the spar tubes are fully mated, a non-standard taper bolt is installed into a pre-drilled alignment hole on the top surface of each spar assembly, one on each side of the fuselage. These taper bolts secure the wing and prevent any movement. When installed properly, the taper bolts are threaded into a removable nutplate assembly incorporating a fibre locknut inside the centre section spar.
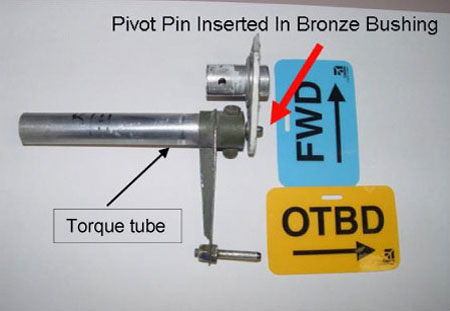
When the wings are installed, the pivot pin on the outboard end of the flap-drive torque tube must be guided into the bronze bushing on the flap arm (see Photo 1). The pin must be visually checked from underneath the aircraft to ascertain that the correct assembly has been accomplished. As a further check of the assembly, the flaps should be extended and retracted using cockpit controls.
If the pivot pin is not aligned with the bushing in the flap arm as the wing is ratcheted into position, the end of the torque tube will butt tightly against the flap arm. The flaps may move when selected from the cockpit because of the friction between the torque tube and flap arm. On the ground where there is no air load, the flaps could work correctly and remain in the down position when selected down. However, in the air, if the pivot pin is not in the bushing, vibration and air loads could cause the flap to partially or fully retract, resulting in a flap asymmetry. According to the kit manufacturer, a flap asymmetry would cause the BD5-J to roll rapidly, and full aileron input would be insufficient to counter the roll.
On the day before the accident flight, the aircraft had been transported to the Ottawa/Carp Airport and assembled by the pilot. Following the assembly, the pilot inspected the aircraft to ensure that the flight controls worked properly and that everything was ready for the planned practice flight the following day. On the morning of the accident flight, the pilot was asked to take the aircraft to the Ottawa/MacDonald-Cartier International Airport for a media event. The pilot disassembled the aircraft, loaded it into the trailer, and drove to Ottawa where the aircraft was re-assembled for the brief media event. The aircraft was then disassembled, moved back to Carp in the trailer, and re-assembled. The pilot checked the aircraft again before the accident flight, and no discrepancies were noted. The pilot reportedly checked the flaps for correct installation and function following the most recent wing installation.
The initial impact was 460 feet southwest of the button of Runway 10. The aircraft slid 23 feet and came to rest on a heading of approximately 200° magnetic (see Appendix A). The aircraft hit the ground in a slightly nose-low, left-wing-down attitude. The ground scars showed that the landing gear was down and that both wings separated from the aircraft at impact. When the aircraft was examined at the site, no discrepancies were found in the aileron, rudder, or elevator control systems.
The aircraft wreckage was transported to the TSB Engineering Laboratory in Ottawa where a detailed examination of the aircraft was performed. The examination indicated that both wing spars failed at impact approximately one foot outboard of their respective wing root ribs. The left wing had been bent slightly upwards. The left aileron was displaced upward, and the right aileron was displaced downwards. Both flaps were attached to the wings, and were free to move. The left flap torque tube had failed in bending overload about one foot inside the fuselage wall; it was found in the wreckage trail. The flap drive mechanism was basically intact, and alignment of the fracture surfaces in the torque tube revealed that the left flap was up at impact. The right flap torque tube was found in the flap-up position. Impact signatures on the flaps also indicated that the flaps were in the up position at impact.
When viewed through the fractured ends of the wing spars, neither taper bolt was in safety in the fibre nut.Footnote 2 The left-wing taper bolt had a space of approximately 0.04 inch between the head of the taper bolt and the spar and was readily removed from the spar and nutplate assembly using fingers only. The fibre locknut presented no resistance to the removal of the taper bolt as the locking feature of the nut was found to be unserviceable. The right-wing taper bolt, with a space of approximately 0.14 inch between the underside of the bolt head and the spar, was found bent forward and loose, and the bolt hole was slightly deformed. The taper bolt was removed using half-turn of a ½-inch wrench and then using fingers only. The locking mechanism of the fibre locknut had not been cut (that is, the threads of the taper bolt had never passed through the locking feature of the nut into safety).
Transport Canada recognizes Federal Aviation Administration (FAA) Advisory Circular 43.13-1B&2A as a resource for standard fastener practices. This document refers to aircraft fasteners, and on the subject of fibre locknuts, states the following:
After the nut has been tightened, make sure the rounded or chamfered end bolts, studs or screws extend at least the full round or chamfer through the nut. Flat end bolts should extend at least 1/32 inch through the nut. When fiber-type self-locking nuts are reused, check the fiber carefully to make sure it has not lost its friction or become brittle. Do not reuse locknuts if they can be run up finger-tight.
The BD5-J construction manual instructs the builder to drill a 0.25-inch hole for the taper bolt through the spars and carefully ream the hole using the BD-0052 tapered reamer. It cautions that proper diameter and depth of the reamed hole is attained when a space of approximately 0.05 inch is left between the top of the main spar and the bottom of the taper bolt head, when the taper bolt is properly torqued. The manual recommends that the taper bolts be torqued to 50-70 inch-pounds when installed, and the bolt threads should be examined after each removal to ensure they are not damaged. The manual also recommends that the taper bolts be replaced after the wing has been removed 8 to 10 times. Also, it recommends that the nutplate with the fibre locknut for securing the taper bolt be replaced after the wing has been removed 25 to 30 times.
There was no record that the nutplates on the accident aircraft had ever been replaced, and as indicated previously, the left nut was found to be unserviceable. Reportedly, spares were available and the pilot replaced them on a regular basis. The records indicate that the taper bolts were inspected and found to be within dimensional tolerance during the last two annual inspections. Reportedly, the pilot had a supply of replacement taper bolts available.
It is not possible to check the taper bolt after it is installed to ensure that it is in safety. The kit manufacturer indicated that the BD5 had been safely flown in the past, even without the taper bolts installed. The manufacturer also indicated that, because of the tight fit of the spars, the wing would not come off in flight, and that the wing incidence could not change because of the wing fitting into the fuselage-to-wing fillet.
As originally manufactured, the flap system on the BD5-J was manually activated. The flap system on the accident aircraft was electrically driven and consisted of a control switch mounted on the side stick, an electric motor, pushrods, bellcranks, torque tubes, and a flap attached to the trailing edge of each wing. With this modification, full flap extension or retraction occurred in three seconds. It appears from the amateur video that the flaps were partially extended when control of the aircraft was lost. Examination of the impact signatures on each flap, and the measurement of the extension of the flap actuator, indicated that the flaps were retracted (up) at impact.
A detailed examination of the right flap hinge arm assembly revealed indentations and a crack in the bronze bushing. There were circular score marks and indications of smearing on the material adjacent to the bushing. These marks had the appearance of being made recently and were consistent with damage that would occur during movement of the flaps. The indentations corresponded in size and radius to the guide pin installed in the end of the flap drive torque tube. The radius of the circular score marks and rubbing corresponded with the radius of the flap drive torque tube. The smearing indicated that the torque tube had moved upward and aft around the bronze bushing (see Photo 2).

The BD-5 community, through previous similar incidents, was aware that an incorrect assembly of the wing flap hinge arm to the flap pivot pin could occur during wing installation. An information document entitled "Pop goes the flap pin" was generated and promulgated to the owners/operators of the BD5, advising them as follows: "Be sure to check that your flap pivot pin is fully seated in the wing when you install it."
Analysis
The taper bolts that secure the wings were found to be not in safety. This contravenes standard aviation practice. The locking feature of the fibre nuts into which the taper bolts were installed was found to be unserviceable in the left wing, and not used in the right wing. Given the total thickness of the spars and the length of the taper bolts, the bolts were long enough to engage the fibre nuts in a manner for safe installation. However, the right taper bolt did not penetrate the wing and fuselage spars far enough to engage the locknut safely.
The taper bolts only pass through the top of the spar, and it is, therefore, not possible to visually inspect the inside of the spar with the wing installed. Although the taper bolts as found did not appear to be torqued, this could have been the result of the accident impact forces. Regardless, torquing the taper bolts ensures that they have engaged in the threads of the fibre locknut, but it does not ensure that they are in safety. Although the construction plans indicate a properly installed taper bolt will have a space of approximately 0.05 inch between the head and the spar, this would be difficult to check with the aircraft fully assembled, and there is no means of verifying that the taper bolts are in safety once the wings are installed.
The kit manufacturer was aware that it was possible to incorrectly install the flap during wing installation, and the manufacturer recommended guiding the pivot pin, on the inboard end of the flap drive torque tube, into the bronze bushing on the flap arm while installing the wing. The manufacturer also realized that an incorrectly installed flap could function normally on the ground, but under in-flight load conditions, the flap could retract, either partially or fully. As the uncommanded roll resulting from the flap asymmetry could not be corrected by opposite aileron input, the only means of correcting the uncommanded roll would be to retract the extended flap to remove the asymmetry.
Reportedly, the pilot checked the flaps for correct installation and function before the accident flight. However, an examination of the aircraft indicated that the right flap was incorrectly installed, in that the torque tube pin was not secured in the flap arm bushing, which would allow the flap to retract in flight.
It was determined that the flaps were up at the time of impact. Therefore, it is most likely that the pilot partially extended the flaps for the final slow-speed fly-past, and that the right flap retracted during the fly-past due to the improper installation. The pilot attempted to correct the problem with control stick input and by retracting the flaps. However, because of the altitude of the aircraft and the time required to retract the flaps, there was insufficient altitude to allow a successful recovery.
Findings
Finding as to Causes and Contributing Factors
- The right flap was incorrectly installed during the wing installation, which allowed the right flap to retract during the fly-past. This created a flap asymmetry that resulted in an uncommanded and uncontrollable right roll. The aircraft was at an altitude from which recovery was not possible before the aircraft struck the ground.
Findings as to risk
- The right-wing taper bolt did not penetrate deep enough through the spars to engage the fibre locking feature of the locknut. Therefore, the taper bolt was not in safety at the time of the accident.
- The fibre locking feature of the left-wing locknut was worn and did not secure the left-wing taper bolt in safety.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices
