Collision with Terrain
Helicopter Transport Services (Canada) Inc.
McDonnell Douglas Hughes 369E (Helicopter) C-FHMF
Davy Lake, Saskatchewan, 29 nm E
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The pilot of the McDonnell Douglas Hughes 369E helicopter (registration C-FHMF, serial number 0370E) was transporting a team of two line-cutters from their company's base camp in the vicinity of Davy Lake, Saskatchewan, to nearby line-cutting operations. The pilot was flying at altitudes from 300 to 500 feet above ground level in the vicinity of a small, unnamed lake when a caribou was spotted swimming across the lake. The pilot turned and descended toward the animal. The helicopter subsequently struck the lake at about 100 knots, at approximately 0830 central standard time. The helicopter sank soon after impact, but the three occupants were able to egress from the submerged wreckage. The pilot and one passenger, who had both sustained serious injuries, were able to swim to shore. After removing their work clothing, they swam back to rescue the second passenger who was in difficulty in the water. Their attempt was unsuccessful and the second passenger drowned. The two survivors were rescued later that afternoon.
Factual information
At the time of the accident, 0830 central standard time,Footnote 1 the weather was sky condition clear. There was a slight ripple on the surface of the lake indicating very light wind. In very light winds, the patches of the water surface can change quickly from a rippled to a glassy appearance and back again, called "cat's paws." The temperature was estimated to be approximately 10°C. The water temperature of the lake was 12°C.
The pilot held a commercial helicopter pilot licence validated by a Category 1 medical certificate and endorsed for the Hughes 369 series helicopter, and was restricted to daylight flying only. He had been hired by the company in 2005 after completing his basic helicopter training. The company policy for hiring pilots directly from flight school was to employ them first as a loadmaster to assess the individual's potential as an employee. The company then provided a successful candidate with training on aircraft type as well as training on company procedures and values.
The pilot followed this process and started employment as a loadmaster. After successful completion of this observation period, he was selected to undertake the company's pilot training program in March 2006, which included a pilot decision making course. After a recurrent training flight in early July, he completed his first deployment, and following a short break in mid-July, deployed to Davy Lake Camp. Both deployments were with helicopter C-FHMF. At the time of the accident, the pilot had approximately 225 hours of total flying experience, all on helicopters. In the last 90 days, he had flown approximately 100 hours, most of which was flown in C-FHMF.
About 48 hours before the accident, the pilot received treatment for a minor infection. According to medical authorities, the medication prescribed would have had no effect on the pilot's ability to fly, and the treatment would normally minimize symptoms of the infection within 48 hours. The pilot met the appropriate flight time limitations and time free from duty requirements of the Canadian Aviation Regulations (CARs). The pilot had 7 ½ hours of sleep on the night before the accident flight and was well rested. He flew two short flights before the accident flight.
Section 602.62 of the CARs requires that an aircraft operating over water, beyond a point where the aircraft can reach shore in the event of an engine failure, be equipped with a life preserver or personal floatation device for each person on board. As there was no requirement for C-FHMF to be operated beyond gliding distance to shore, passengers were not provided with personal floatation devices.
The pilot was flying the helicopter from the left seat. One passenger was in the front right seat and the other passenger was seated in the right rear seat. When the caribou was spotted in the water, the pilot began a right turn toward the lake, leaning forward during the turn to keep the caribou in view. A steep descent developed over the trees and the pilot initiated recovery. The flight path of the helicopter continued over the water, paralleling a portion of the shoreline approximately 100 feet from the shore. The pilot continued levelling the helicopter but did not perceive that collision with the water was imminent and flew the helicopter into the water. For the operating conditions at the time of the accident, the helicopter's never exceed speed (Vne) was 130 knots. There was no report of any unusual control forces, warning lights, or warning horns before or during the descending turn.
Fascination is a condition in which the pilot fails to respond adequately to a clearly defined stimulus situation, despite the fact that all of the necessary cues are present and the proper response is available to him.Footnote 2 This is commonly referred to as "target fixation" and is fundamentally perceptual in nature. The individual concentrates on one aspect of the total situation to such a degree that he rejects other factors in his perceptual field.
A second perceptual problem occurs over water in conditions of very light or no wind. The water surface is featureless without wave action, commonly called "glassy water," and makes accurate judgement of height above the water impossible. The pilot can experience the illusion that he is higher than he actually is. The pilot had no knowledge of the glassy water phenomenon.
TSB investigators did not attend the accident site. The wreckage was recovered from the lake by the company and photographed extensively. It was intended to move the wreckage to a remote airstrip for examination by investigators, and the wreckage was transported by helicopter as a sling load. En route, the sling was cut by a sharp piece of wreckage and the load dropped about 1500 feet to the ground. The wreckage was then placed in a net and transported to the airstrip for examination.
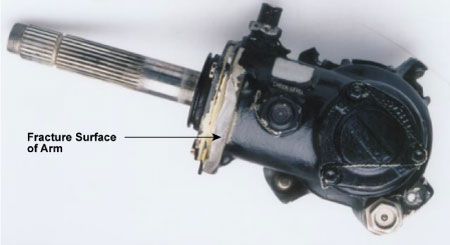
While examination of the wreckage was hampered by the second impact, it was possible to establish that the engine was operating at high power and that continuity of controls existed during the accident sequence. Main and tail rotor blades showed impact damage consistent with high rotational energy. All breaks were found to be overload failures due to impact forces, except for a fracture found in the tail rotor bell crank support arm. The tail rotor assembly and instrument panel were taken to the regional wreckage examination facility and subsequently examined at the TSB Engineering Laboratory in Ottawa.
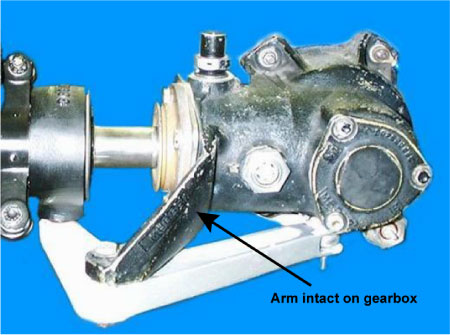
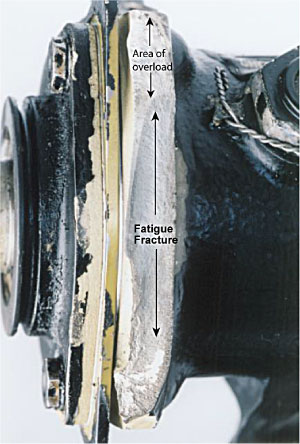
Examination of the instrument panel indicated that the generator-out warning light was illuminated before the filament was stretched by impact forces. No other warnings were illuminated. The examination of the instruments did not provide any reliable information for analysis. The fracture in the bell crank support arm was found to be a fatigue fracture that had developed through 75 per cent of the support arm. A photograph taken of the wreckage immediately after it was recovered to shore, and before the second impact, revealed that the bell crank support arm was still intact. The photograph also showed that paint was missing along the fracture line. The photographs in Appendix A were taken after the second impact. The remaining section of the bell crank support arm failed in overload due to the secondary impact. The entire fracture surface can be observed.
Two days before the accident flight, a 100-hour inspection was completed on C-FHMF by a contract aircraft maintenance engineer (AME). The inspection was started during daylight hours and completed during the hours of darkness with the aid of a flashlight. The area of the tail rotor was inspected in darkness. The missing paint in the area of the fatigue fracture in the bell crank support arm was not noticed by the AME during the 100-hour inspection or by the pilot during daily pre-flight inspections.
A slight vibration or buzz in the tail rotor pedals had been reported before the accident flight, and, therefore, the tail rotor pitch bearings were closely inspected by the AME during the 100-hour inspection. The inspection revealed slightly worn tail rotor pitch bearings. Pitch bearings are located in the grip of each tail rotor blade and allow blade pitch movement around the hub. It was decided that the bearings were still serviceable but should be closely monitored.
Pitch bearing wear is determined by the amount of play measured at the tail rotor blade tip and should not exceed 0.250 inch as referenced in Chapter 64-10-00 of the McDonnell Douglas 369E maintenance manual. Play measurements of each blade tip taken by TSB investigators after the accident revealed blade tip movements of 0.110 and 0.120 inch. No other anomalies were found with the tail rotor gearbox.
A review of the aircraft maintenance records indicated that the aircraft was maintained and certified in accordance with the operator's maintenance control system. There were no deferred items or defects that may have contributed to the accident. The condition of the wreckage was found to be consistent with the description of the accident sequence.
The autopsy indicated that the non-surviving passenger drowned. The autopsy indicated that the type of injury that this person sustained during the impact would have made breathing difficult in conditions requiring physical exertion. The non-surviving passenger was dressed in work clothing and heavy boots.
No signal was received from the emergency locator transmitter (ELT) following the crash. The ELT was not recovered and could not be examined. Aircraft maintenance records indicate that the aircraft was equipped with a non-submersible type of ELT. It was likely rendered inoperative by the water when the helicopter sank.
Analysis
Although the pilot had completed pilot decision making training, he did not apply these principles when deciding to manoeuvre and observe the caribou. The decision was made without consideration of the safety issues for over-water flight or knowledge of the hazards of the glassy, or near glassy, water phenomenon. The pilot likely fixated on the caribou and lost situational awareness, thereby allowing the helicopter to enter a high rate of descent at low altitude. When the pilot became aware that the helicopter was in a steep descent over the trees, he attempted to stop the descent but the helicopter continued out over the water surface. It is likely that difficulty with height judgement over glassy or near-glassy water impeded his recovery. As a consequence, he flew the helicopter into the lake at high speed while attempting to level off.
The pilot's medical condition had been under treatment for about 48 hours. It is unlikely that the symptoms were a source of distraction for the pilot.
It was not possible to determine when the generator-out light illuminated. However, the loss of the generator capacity would not have affected the flight characteristics of the helicopter. The illumination of the light indicated that battery power was available.
Since photographs revealed that the tail rotor bell crank support arm was still intact and had not broken apart before the crash, the developing fracture in the bell crank support arm likely did not contribute to the accident. Operation of the helicopter resulted in some movement of the bell crank support arm and caused paint to flake along the fractured area. The flaking of the paint was probably missed during the inspection because the tail rotor area was examined in darkness with the aid of a flashlight.
It is likely that the slightly worn pitch bearings resulted in the reported vibration of the tail rotor pedals. The vibration would not have affected the pilot's ability to control the helicopter in the turn.
The non-surviving passenger was impeded by injuries, heavy work clothing, and low water temperature. Personal floatation equipment could have assisted in the rescue of this passenger.
The following TSB Engineering Laboratory reports were completed:
- LP 087/2006 – Analysis of Instruments
- LP 090/2006 – Tail Rotor Gear Box Examination
These reports are available from the Transportation Safety Board of Canada upon request.
Findings
Finding as to Causes and Contributing Factors
- The pilot lost situational awareness while turning and entered a high rate of descent at low level. The recovery stage continued over glassy or near-glassy water and the pilot flew the helicopter into the water at high speed.
Finding as to Risk
- Serviceability inspections of the helicopter did not detect the fatigue crack developing in the support arm.
Safety action
Safety action taken
On 20 February 2007, the TSB issued Safety Information Letter A06C0131-D1-L1 - Pre-Crack/Fatigue Crack of the Tail Rotor Gearbox Bellcrank Support Horn, to the Director General, Civil Aviation. The Safety Information Letter stated that, in this occurrence, an inspection of the wreckage revealed a suspicious fracture surface of the tail rotor gearbox bell crank support horn. Analysis of the fracture revealed a pre-crack/fatigue crack extending across approximately 75 per cent of the entire cross section of the bell crank support horn. The fractured horn did not contribute to the accident.
On 30 March 2007, the Director General, Civil Aviation responded to the Safety Information Letter indicating that the letter had been provided to the appropriate Departmental officials for their information and use.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on 03 May 2007.