Tail-Rotor Strike (External Load) - Loss of Control
Transport Canada
MBB BO 105 Helicopter C-GCHX
Bella Bella, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Canadian Coast Guard Messerschmitt-Bolkow-Blohm (MBB) BO 105 helicopter (registration C-GCHX, serial number S695), operated by Transport Canada as CTG357, was carrying out external load operations near Bella Bella. It had completed 27 external loads and was returning to the Canadian Coast Guard ship (CCGS) Bartlett from Dryad Point Lighthouse Station with an empty cargo bonnet.
En route over the water at an altitude of about 200 feet, the bonnet went above and behind the tail rotor, and the longline hung up on the back of the helicopter. The helicopter slowed, began to descend, turned right and then crashed into the water. It sank immediately. The pilot was able to exit the sunken helicopter but remained face down in the water. He was wearing an uninflated lifejacket. The pilot was rescued within three minutes and revived, but remained in critical condition for several days. The helicopter was found at a depth of 26 metres on an ocean floor slope.
Other Factual Information
The weather was as follows: scattered cloud at 2000 feet, visibility about 15 miles, winds calm, and the seas rippled.
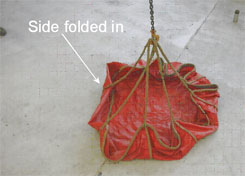
The sling equipment being used was a 33-metre synthetic rope line (longline) attached to the helicopter's belly hook, with a swivel hook at its end. Attached to that extended hook was a bonnet (see Photo 1) with some rope gear and slings inside. It was lashed closed with a polypropylene rope. The bonnet weighed less than 10 kg, and the total external load weight was less than 40 kg. The surface area of the external load was about 2.6 square metres. Photo 3 shows the actual gear and its configuration.
The pilot was flying from the right seat with the right door removed. The pilot was wearing the lap belt; however, he was not using the available upper-body restraint system, as it restricts pilots from leaning out to view the external sling load.
The helicopter was moving at about 60 knots when the pilot felt and noticed the bonnet open. The sling gear was still in it, but the bonnet was folded in (see Photo 1) between the one o'clock and the two o'clock position. About two seconds later, the bonnet and longline travelled to the port side of the helicopter, appearing at the pilot's ten o'clock position, slightly above eye level. It moved backwards and out of sight, then there was a bang followed by some thrashing noises, and the helicopter began to turn right. The pilot could see the line hanging from high on the tail, trailing down, back and out at about the four o'clock position. The bonnet was not evident on the line. As this was happening, the pilot slowed the helicopter and reduced power by lowering the collective and bringing the throttles to the engine idle position. Just before impact, the pilot increased the throttles to full and raised the collective a small amount. The helicopter hit the water sooner than expected, and the pilot had not activated the emergency floatation system.
The helicopter sank immediately after impact with the water. The pilot was wearing a helmet, and even though it was structurally damaged from impact, he remained conscious as the helicopter sank. The pilot unlatched his lap belt and swam to the surface. He did not remember having a life vest on and did not inflate it. At the surface, the pilot tried to grab items to hold onto, but they sank and he could not keep his head above the water. A boater saw the accident and was picking up some of the debris when he noticed the top of the pilot's helmet. The helmet was painted grey and the pilot was wearing a navy blue flight suit, which was hard to see in the ocean. The uninflated yellow floatation device was protected by a navy blue life-vest cover and thus not readily visible. As the boater got closer to the helmet, he recognized it as a helmet with a body attached. The boater was able to get the pilot's head out of the water until Canadian Coast Guard rescue boats arrived and attendants revived the pilot.
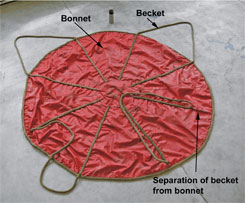
The helicopter wreckage was photographed and the sling gear was recovered. The longline was wrapped around the tail-rotor driveshaft, between the tail rotor and the 90° gearbox. The line had released from the helicopter's belly hook and lay about 2 metres away from the helicopter hook. The line was broken about 8 metres from its lower hook. All the beckets of the bonnet (see Photo 2) were secured in a short sling, which was secured in the lower hook. The polypropylene rope was still wrapped around the beckets, but it was loose (see Photo 3). Two of the beckets were partly separated, one about 23 cm from the lip of the bonnet (see Photo 2). Further examination of the helicopter wreckage on land revealed that the longline was released before the helicopter struck the water.
It was determined that persons seated in either of the front seats were able to hit their heads on a fixture between and behind the two front seats, installed to hold a liferaft. Only the liferaft support structure is near enough to be contacted by the front-seat occupants' heads, even when the occupants are secured in their seats with the available upper-body restraint devices. This modification was installed by the operator in accordance with an approved Limited Supplementary Type Certificate.
The pilot was trained and certificated appropriately. He had extensive experience in external load operations and had completed underwater egress training. Records indicate that the helicopter was maintained to the required standards.

In 1993, the TSB carried out an engineering analysis of helicopter sling aerodynamics and produced Engineering Report LP 51/93. At that time, in response to the engineering report and occurrence A92W0177, the Board issued recommendation A93-12, directed to Transport Canada. The recommendation highlighted the fact that, within the industry, there had been several helicopter accidents resulting from tail-rotor damage caused by contact with slings. Those accidents resulted in several fatalities, serious injuries and, in most cases, substantial aircraft damage. A large portion of the accidents involved flights with an intentionally empty, unweighted sling, even though the helicopter community recognized this to be a hazardous practice. It was recommended that Transport Canada coordinate the development and implementation of airworthiness standards and operational limitations for helicopter slinging equipment.
The response from Transport Canada indicated that the responsibility to ensure safe slinging would remain with operators, with a requirement that company operations manuals would include instructions on the type of equipment to be used for specific operations, procedures, equipment inspection and maintenance. The use of slinging equipment in an unsafe manner has continued, as demonstrated by this occurrence.
In 2001, the TSB Director of Investigations (Air) drew to Transport Canada's attention, in the form of Safety Advisory A010006, that although the seats in the cockpit of helicopters were equipped with four-point safety harnesses, pilots used only the lap-belt portion of the harness. This was only loosely fitted when carrying out vertical reference slinging operations, and the equipment provided is ill-suited to the task of vertical reference flying during external load operations. Moreover, an analysis of helicopter crash dynamics by ColtmanFootnote 1 showed that, of the personnel who experienced a helicopter crash, only 9 per cent of those who were wearing a shoulder harness had severe injuries, compared with 34.3 per cent of those who wore only a lap belt. Transport Canada's response to the safety advisory letter was that it was the industry's responsibility to comply with the regulations and, if warranted, apply for an approval of a configuration to meet its operational needs. The practice of operating without the use of upper-body restraint equipment continues, as demonstrated in this occurrence.
Slinging external loads using vertical reference techniques is common in helicopter operations around the world, and very common in Canada. Most helicopters are not designed to accommodate this practice, and certification for external load operations does not take these techniques into account.
Analysis
It is most likely that the polypropylene rope, used to snug the top of the bonnet, slid up the beckets and the bonnet opened in flight. The pilot described seeing the starboard front area of the bonnet folded in, likely because the separated becket allowed the formation of an asymmetric shape. The resulting shape and the bonnet's light weight and high drag allowed the bonnet to fly up and into the flight path of the helicopter, carrying the longline with it. The longline subsequently came into contact with the tail rotor and disabled it, rendering the helicopter uncontrollable.
At impact, it is likely that the pilot's upper body moved around the cabin. This would have been facilitated by the lack of an upper-body restraining device and is evident by the pilot's fractured helmet. The helmet protected the pilot's head from severe injury, thereby allowing him to extricate himself from the sunken wreckage. However, in this particular helicopter, even when persons occupying either front seat are properly secured, they risk hitting their heads on the fixture to which the liferaft is normally secured.
The colour of the pilot's helmet and flight suit (grey and navy blue, respectively) made it difficult to see him in the ocean, thereby increasing the risk of him not being found and rescued.
Findings
Finding as to Causes and Contributing Factors
- The rope used to snug the top of the bonnet most likely slid up the beckets, allowing the bonnet to open and fly into the flight path of the helicopter carrying the longline with it. The longline came into contact with the tail rotor and disabled it, rendering the helicopter uncontrollable.
Findings as to risk
- Most helicopters are not designed or certified to accommodate vertical reference external load operations; however, these operations are very common and pilots fly in this higher-risk environment without proper safety-restraint devices.
- It is likely that the pilot's unrestrained upper body moved around the cabin at impact. This increased the risk of injury and, in this case, the risk of drowning.
- Even when properly secured, persons in either front seat risk hitting their heads on a fixture to which the liferaft is normally secured.
- The colour of the pilot's helmet, life-vest cover and flight suit (grey and navy blue, respectively) made it difficult to see him in the ocean, increasing the risk of him not being found and rescued.
Other Finding
- The pilot's helmet protected his head from severe injury, allowing him to extricate himself from the sunken wreckage.
Safety action
Transport Canada
On 09 May 2005, Transport Canada Aircraft Services Directorate issued a safety notice, restricting operations with empty or light external sling loads.
On 25 May 2005, Transport Canada Aircraft Services Directorate produced draft Standard Operating Procedures (SOPs) for helicopter external load operations. These SOPs restrict the use of bonnets and caution pilots about light and unstable loads.
Transportation Safety Board
On 31 May 2005, the TSB Director of Investigations (Air) sent a Safety Information Letter to Transport Canada, outlining the facts of this accident that showed that, despite the Canadian Aviation Regulations (CARs) and the previous Safety Advisory to Transport Canada (A010006), helicopter slinging operations without upper-body restraint continue.
In response to the above-noted letter, Transport Canada provided the following:
- If the upper-body restraint equipment is used properly, and in accordance with the CARs, they will provide the protection intended by those requirements.
- It is the operations being conducted when these accidents occurred that led the pilots to loosen and/or remove elements of their restraint system. The existing CARs (Section 605.27(3)) require at least one pilot to have the safety belt, which as per the definition in Section 101.01 of the CARs, includes the shoulder harness fastened during flight time.
- If an operator discovers that installed equipment, shoulder harness in this case, is unsuitable for "Vertical Reference Helicopter Sling Operations" then Transport Canada has a well-established process in place for assessing and approving supplemental aircraft equipment.
- It is the responsibility of the industry to comply with the regulations, and, if warranted, apply for an approval of a configuration to meet the industry's operational needs. Transport Canada continues to welcome air operator and manufacturer initiatives to promote safe helicopter external load operations.
- Notwithstanding the current regulations and industry initiatives undertaken to date, Transport Canada has initiated the process to conduct research and development on the issue. A proposal has been submitted to the Civil Aviation Research and Development Committee to study crew restraint in vertical reference external load (VREL) operations. The objective is to develop a new restraint system and produce a safety education and promotion product on VREL operations.
On 31 May 2005, the TSB Director of Investigations (Air) sent a safety advisory to Transport Canada, indicating that, during this investigation, a test revealed that, even when properly restrained, persons seated in either of the front seats are able to hit their heads on a fixture installed to hold a liferaft. The advisory suggested that Transport Canada may wish to modify the fixtures that hold the liferafts in the Messerschmitt-Bolkow-Blohm BO 105 helicopters to remove the hazard or limit use of the front seats to persons wearing protective head gear. It also suggested that Transport Canada may wish to verify that other aircraft have not been modified to induce similar hazards.
In response to the above-noted safety advisory, Transport Canada provided the following:
- Transport Canada is undertaking a complete review of the applicable Limited Supplemental Type Certificate (LSTC) data package with regards to this occurrence. The data used to show compliance with Section 27.561 of the United States Federal Aviation Regulations are being reviewed and a determination will be made as to whether a design change is required. Although the review is not yet complete, it is possible that padding could be added to the fixture and a requirement be made that helmets are to be worn with this installation.
On 01 June 2005, the TSB Director of Investigations (Air) sent a safety information letter to Transport Canada, highlighting the facts of this accident and the continued operational practices of helicopters carrying empty or light slings. The letter pointed out that the Board had made a recommendation (A93-12) to Transport Canada in 1993 that it coordinate the development and implementation of airworthiness standards and operational limitations for helicopter slinging equipment.
In response to the above-noted safety information letter, Transport Canada provided the following:
- Chapter 527.865 of the CARs addresses external loads for normal category helicopters and Chapter 529.865 of the CARs deals with transport category helicopters. These standards state the certification basis for helicopters equipped with external slinging capabilities (cargo hook). Helicopter slinging equipment is considered part of the load rather than the helicopter; therefore, it is not subjected to a Technical Standard Order (TSO) or STC approval process.
- The responsibility to ensure safe slinging operations remains with the operator, and specific information on slinging and crew training is to be contained in the company operations manual. Transport Canada continues to welcome air operator and manufacturer initiatives to promote safe helicopter external load operations.
- Strategies to address helicopter rotor/sling strikes, and unsafe equipment and practices that lead to them, have included numerous articles in Transport Canada's safety publications such as the Aviation Safety Vortex newsletter.
- Transport Canada continues to be concerned with this area of operations. Currently, the Department is producing a new safety awareness video titled "Helicopter External Load Operations, Ground Crew Safety." The video's intended audience is ground crew operations and will address subjects such as occupational safety and health issues, briefings, protective equipment, communications and checking load and equipment such as straps and bonnets.
- Transport Canada is drafting another article based on this information letter for publication in Transport Canada's Aviation Safety Letter.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .