Controlled Flight Into Terrain
Wabusk Air
Piper PA-31 Navajo C-GKMW
Kashechewan, Ontario
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
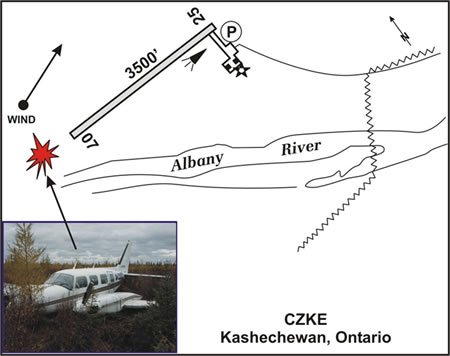
The Wabusk Air Piper PA-31 Navajo aircraft (registration C-GKMW, serial number 725) departed Runway 25 at Kashechewan, Ontario, at approximately 2130 eastern daylight time on a night visual flight rules flight to Moosonee, Ontario, 72 nautical miles to the southeast. The captain was the pilot flying and was seated in the left seat. The aircraft became airborne approximately halfway down the runway, and the flight crew lost sight of the runway lights and any visual reference to the ground shortly after take-off. The captain selected the landing gear up, and, at 200 feet above ground level, the first officer selected the flaps up, after which the captain set climb power. There was a slight drop in manifold pressure on the left engine, and the captain was readjusting the power when the aircraft struck the ground. The aircraft bounced into the air and came to rest approximately 300 metres past the departure end of the runway. The aircraft was substantially damaged by impact forces. The six passengers and two pilots were not injured.
Factual information
Wabusk Air is a charter company, operating three Piper PA-31 Navajo and one Piper PA-31-350 Chieftain aircraft, based out of Moosonee, Ontario.Footnote 1 It provides passenger and cargo service to many isolated communities in the Northern Ontario, James Bay, and Hudson Bay regions.
The captain and pilot flying (PF) had been employed with Wabusk Air for approximately six weeks. This was his first flying job in a northern remote area. The majority of his flying at Wabusk Air had been single-pilot visual flight rules (VFR) operations. He was certified and qualified for the flight in accordance with existing regulations. He held a valid airline transport pilot licence and was approved to fly the Piper PA-31 aircraft under single-pilot instrument flight rules (IFR). He had accumulated approximately 1600 hours of total flight time, including 200 hours at night, and a total of 245 hours on type. The captain started work at 1030 eastern daylight timeFootnote 2 on the day of the occurrence and was well rested. He had been on duty for 11 hours at the time of the occurrence and had accumulated 7.4 hours of flight time for the day. The day before the occurrence, he had also been on duty for 11 hours. He had had a day of rest five days before the occurrence, and had finished a week of rest eight days before the occurrence.
The first officer had been employed by Wabusk Air for approximately four months working primarily as a loader and dispatcher. He held a valid commercial pilot licence and was trained in accordance with the company operating manual. He often flew as a first officer to gain experience and accumulate flying hours. His instrument rating had expired and, therefore, he was only approved to act as a flight crew member for VFR operations. The first officer started work at 0830 on the day of the occurrence, and the occurrence flight was his only flight that day.
Records show that the aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. There were no reported mechanical abnormalities on previous flights that day.
The aircraft was fitted with a Boundary Layer Research, Inc. modification (STC SA00047SE). This supplemental type certificate (STC) increased the maximum take-off weight (MTOW) of the aircraft from 6500 pounds to 6730 pounds if equipped with wing lockers, or to 6840 pounds if not equipped with wing lockers. C-GKMW was equipped with wing lockers. However, Wabusk Air was incorrectly using an MTOW of 6840 pounds. Two aircraft inspection reports from Transport Canada, dated 05 June 2003 and 19 July 2004, list the MTOW as 6500 pounds and 6840 pounds respectively, even though the correct MTOW was 6730 pounds. An aircraft inspection report from Transport Canada dated 04 April 2005 indicated that there were no carry-on baggage restraints in the back of the aircraft.
Aviation routine weather reports (METARS) are not available for Kashechewan. The nearest weather reporting station is in Moosonee, which reported the weather at 2100 as follows: wind 200° True at seven knots, visibility nine statute miles, ceiling 6800 feet above ground level (agl), temperature 12°C. It was reported that the visibility was unrestricted, and the sky was dark without any moon or stars visible.
Before departing Moosonee for the round trip to Kashechewan, the flight crew calculated the aircraft's weight and balance using a computer program. The information was entered into the operational flight plan, including standard weights for the passengers and an estimated baggage allowance of 30 pounds per person for the departure from Kashechewan. The calculated aircraft weight for the departure from Kashechewan was 6530 pounds.
On arrival at Kashechewan, the aircraft was reconfigured from a cargo to a passenger configuration. All the baggage that would not fit into the nose compartment was loaded inside the aircraft cabin behind the rearmost seat. Neither tie-down rings nor cargo nets were available, and no attempt was made to secure this baggage. A scale was carried on board the aircraft to weigh the baggage, but it was not used. Therefore, it was not possible to ascertain an accurate cargo weight. Based on passenger-reported weights obtained after the accident, it was estimated that the actual total weight of the passengers exceeded the standard weight by approximately 135 pounds. Despite these inaccuracies, it was determined that the aircraft was likely within the weight and centre of gravity limits at the time of take-off.
The pre-flight briefing, including how to open the exit, as required by Section 703.39 of the Canadian Aviation Regulations, was not given to the passengers. The briefing is intended to explain the use of seat belts, and to describe the location of the emergency locator transmitter, survival equipment, and first-aid kit. It also refers passengers to the on-board safety briefing card, which explains the location and operation of the emergency exits.
Because the lighting on the ramp was poor, the captain used a head lamp to help load and start the aircraft. Once the aircraft was started, he removed the head lamp and used the aircraft lighting. Runway 25/07 at Kashechewan Airport is 3500 feet long and is equipped with aircraft radio control of aerodrome lighting (ARCAL) type K, medium-intensity runway edge lights, and threshold and runway end lights. All the lights were on for the take-off. Kashechewan is located in a sparsely settled area, and the airport is located southwest of the community. When departing at night from Runway 25, the lights from the community are not visible, and there is little or no visual reference to the ground, particularly on a dark, moonless night. Flight into these "black hole" conditions exposes pilots to a higher risk of sensory illusion.
High acceleration during take-off and initial climb can cause an illusion of increasing pitch. Somatogravic illusion is an erroneous sensation of pitch (rotation in the vertical plane) caused by linear acceleration. Under normal conditions, this sensation can be recognized and corrected visually. However, when a take-off is being made on a dark night and toward an area that provides few visual references, this illusion will remain a powerful influence. A pilot's normal response to this pitch-up illusion is to apply forward pressure to the control column to reduce the aircraft's angle of climb.
Wabusk Air standard operating procedures (SOPs) include procedures for flight crews to follow when operating in a two-crew environment. These SOPs are intended to ensure commonality among flight crew members and to ensure safe operation of the aircraft. The Wabusk Air SOPs state that, on take-off, the aircraft will be rotated to 10° nose-up to ensure a positive rate of climb and the climb speed set at best rate of climb to best rate plus 10 knots (112 to 122 knots). The pilot not flying (PNF) will select gear up and, at 400 feet agl, retract the flaps to the up position and set climb power. This procedure allows the PF to concentrate on flying the aircraft to maintain the correct attitude and airspeed.
After the aircraft came to rest (see Appendix A), a passenger seated ahead of the exit kicked the door until it opened, after which the passengers evacuated the aircraft. The flight crew exited last. The bags that were not tied down were strewn about the rear of the cabin, but did not delay the evacuation.
Analysis
It was determined that the aircraft was likely within the weight and centre of gravity limits at the time of the flight, the aircraft systems were functioning correctly, and the engines were producing the requested power during the take-off. This analysis will therefore focus on operational and human factors associated with the two-crew operation and the night-time take-off.
During his time at Wabusk Air, the captain had flown mostly single-pilot VFR flights and, therefore, had had little opportunity to use the two-crew SOPs. Rather than follow unfamiliar SOPs, he elected to retract the landing gear and set climb power himself, as he would have done during a single-pilot operation. It could not be determined if the captain commanded the PNF to retract the flaps or if the PNF performed this task without prompting. In any case, the flaps were retracted below the 400 feet agl specified in the SOPs. While raising the landing gear and setting climb power, the flight crew's attention was focused on secondary controls, the engine instruments, and the airspeed, instead of on the aircraft attitude. As a result, the aircraft developed an undetected sink rate and struck the ground.
Under the prevailing night conditions and with restricted outside visual references, a somatogravic illusion could have caused the pilot to erroneously perceive an increase in the aircraft pitch attitude. While the pilot's attention was diverted from the attitude indicator during gear and power selection, the aircraft entered a descent and struck the ground.
Findings
Findings as to causes and contributing factors
- The flight crew did not follow the Wabusk Air standard operating procedures and ensure that a positive rate of climb was maintained after take-off. The aircraft developed an undetected sink rate and struck the ground.
- During the night visual flight rules departure into "black hole" conditions, the flight crew likely experienced a somatogravic illusion, giving them a false climb sensation. This likely contributed to the captain allowing the aircraft to descend into the ground.
Findings as to risk
- Wabusk Air was using a maximum take-off weight of 6840 pounds, when the actual maximum take-off weight was 6730 pounds.
- Tie-down rings and cargo restraints were not installed in the aircraft. The baggage that was loaded inside the aircraft was not secured, resulting in it being strewn about the rear of the cabin during the crash sequence.
- A pre-flight passenger briefing was not conducted, and the passengers were unfamiliar with the operation of the aircraft exit.
Other findings
- A scale was carried on board the aircraft but was not used. Because the flight crew estimated the baggage weight, the actual weight of the baggage was undetermined.
- The total weight of the passengers, using self-reported weights, exceeded the standard weights by approximately 135 pounds.
- The maximum take-off weight of the aircraft was incorrectly documented during two Transport Canada audits.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
Appendices