Runway Excursion on Landing
Aviation CMP Inc.
Beech B300 (Super King Air) C-FMHD
Saint-Georges, Quebec
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
A Beech B300, registration C-FMHD, serial number FL-87, operated by Aviation CMP Inc., was on an instrument flight from Saint-Hubert, Quebec, to Saint-Georges, Quebec, with two pilots and one passenger on board. At 1126 eastern standard time, following a Runway 06 RNAV (GPS) instrument approach, the aircraft was too high to be landed safely, and the crew carried out a missed approach. The crew members advised the Montréal Centre that they would attempt a Runway 24 RNAV (GPS) instrument approach. At 1146 eastern standard time, the aircraft touched down over 2400 feet past the Runway 24 threshold. As soon as it touched down, the aircraft started to turn left on the snow-covered runway. Full right rudder was used in an attempt to regain directional control. However, the aircraft continued to turn left, departed the runway, and came to rest in a ditch about 50 feet south of the runway. The aircraft sustained substantial damage. There were no injuries.
Factual information
At 1050 eastern standard time,Footnote 1 the Beech B300 operated by Aviation CMP Inc. departed Saint-Hubert, Quebec,Footnote 2 on a 30-minute flight to Saint-Georges, with two crew and with the owner/president of the company on board. The co-pilot was at the controls. It was a self-regulated flight (a flight during which pilots regulate themselves), and the departure was in accordance with instrument flight rules (IFR).
At approximately 1100, Saint-GeorgesFootnote 3 was advised that C-FMHD estimated arrival in 20 minutes. At 1110, Saint-Georges advised the flight that the winds were from the east at four knots and the altimeter setting was 29.65. At the same time, runway snow clearing started. At 1113, the Montréal Centre supplied the latest weather information for Québec. Vertical visibility was 500 feet, horizontal visibility was ½ mile in snow, and the altimeter setting was falling fast at 29.56. The aircraft was then cleared outside uncontrolled airspace for an approach, and the crew commenced a Runway 06 RNAV (GPS) instrument approach (see Appendix A). The crew went through the descent checks and the approach briefing, but did not discuss the possibility of a missed approach during the approach briefing.
At approximately 1115, Saint-Georges advised C-FMHD that the runway was cleared to a width of 60 feet. However, at 1125:16, over the aerodrome UNICOM frequency, it was stated that the runway was cleared to a width of 36 feet. At this time, the pilot-in-command could see the ground. The aircraft was 1.7 nautical miles (nm) from the runway threshold and 1300 feet above sea level (asl).Footnote 4
Forty seconds later, at about ¾ nm from the threshold, the pilot-in-command saw the runway lights and advised the co-pilot that there might be a snowplough on the landing area. At 1126:17, the aircraft was about 200 feet above the runway and too high to land safely. The pilot-in-command took control of the aircraft and commenced a missed approach.
The aircraft did not follow the published missed approach path.Footnote 5 Instead, the aircraft flew a heading of 062° magnetic (M), then followed a path that led it, six minutes later, to a point 18 nm north of the runway. The flight control system (FCS) was programmed for the Runway 24 RNAV (GPS) approach. Once the FCS was programmed, the aircraft turned around and proceeded to intermediate waypoint RIKAL, then to the initial approach waypoint ITRAL, from where the approach was initiated.
The approach profileFootnote 6 includes three levels: over ITRAL, the aircraft can descend to 1900 feet; at 5 nm from the runway threshold, over USDAK, the final approach waypoint (FAWP), the aircraft can continue descent to 1440 feet; and, at 2 nm from the threshold, at the descent waypoint (SDWP) VIXIP, it can descend to the minimum descent altitude (MDA) of 1280 feet (see Appendix B). The missed approach waypoint (MAWP) is over the runway threshold (see Figure 1).
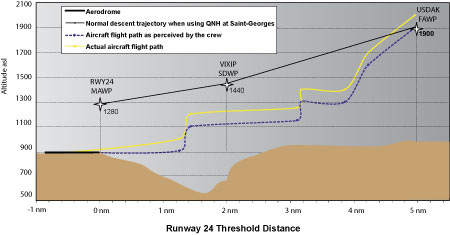
When planning the approach, the briefings were not completed in accordance with company standard operating procedures (SOPs). The crew did not discuss approach procedures or a missed approach procedure. About 3 nm from USDAK and 1900 feet asl (about 1000 feet above ground), the co-pilot saw the ground. He immediately reported the position of the aircraft in reference to the ground and reported the weather conditions. A few seconds later, the pilot-in-command set the altitude selector to 1100 feet, 200 feet below the MDA, and set the radio altimeter to 380 feet, the height above aerodrome (HAA) at the MDA. At a little over 3 nm from the threshold, the aircraft was 200 feet above the ground.
At 1143:08, conditions deteriorated significantly. At 1145:18, the landing check was completed except for the yaw damper, which was left ON. At 1145:24 and about 1.5 nm from the runway, the descent was continued. Five seconds later, the altitude warning sounded.
Approaching ¼ nm, the co-pilot saw the runway to the left. The pilot-in-command, who could not see the runway, followed the co-pilot's directions. The aircraft followed a zigzag path and flew over the precision approach path indicator (PAPI), the runway centreline, and the right-side runway lights, then turned left again. The pilot-in-command saw the runway and landed. The aircraft touched down over 2400 feet past the threshold, and as soon as it touched down, it turned left. Despite the application of full right rudder, the aircraft continued going left. Maximum reverse thrust was selected.
The left main gear, then the nose wheel, struck the snow bank that was left on the runway by the snowplough. The nose gear strut broke and the aircraft fell on its nose. The aircraft turned left and continued moving perpendicular to the runway. The aircraft left the runway and came to rest nose down in a drainage ditch 3600 feet from the threshold. The crew shut down electrical power and cut off fuel, then evacuated the aircraft with the passenger.
The emergency locator transmitter did not activate when the aircraft left the runway. The air transport coordinator/dispatcher could not see the aircraft land because of a slight elevation 2100 feet from the runway threshold. He tried to contact the crew but got no response, so he sent the snow-clearing vehicles onto the runway to find the aircraft. He then phoned 911. The first emergency response vehicle arrived at the accident site eight minutes later.
The crew members were qualified for the flight in accordance with existing regulations. The pilot-in-command and the co-pilot were hired in July 2004 and October 2004, respectively. After they were hired, they took a full training course at CAE Simuflite in Texas, United States, on a Beech B300 simulator. Since neither the pilot-in-command nor the co-pilot was trained with another pilot from Aviation CMP Inc., CAE Simuflite used its own SOPs rather than the company's SOPs.
Aviation CMP Inc. had asked CAE Simuflite to provide its pilots with complementary courses that were to cover 10 subjects, including cockpit resource management (CRM) and controlled flight into terrain (CFIT) risks. Although Aviation CMP Inc. records indicate that the pilots had completed that training, according to CAE Simuflite training records, neither pilot took CRM or CFIT ground-school training. However, CAE Simuflite assessed them as being competent in simulator exercises that included CRM and CFIT.
Before joining Aviation CMP Inc., the pilot-in-command was the chief pilot of a company that operated a Beech King Air. He had little experience flying as a member of a crew. When he began flying for the company, he was paired with experienced Beech B300 pilots. Beginning in mid-October, he flew mainly with the occurrence co-pilot. At the time of the accident, the pilot-in-command had about 4500 flying hours, including 250 hours on the Beech B300. This was his first flight to Saint-Georges in winter conditions. The information received indicates that the pilot-in-command was a conscientious pilot who followed the regulations and landing limits. The pilot-in-command had flown for the company owner twice before. Those flights were made in visual flight rules (VFR) conditions and were described as routine.
The co-pilot was hired as a co-pilot. He did not meet the company's experience requirements for a pilot-in-command position. At the time of the occurrence, he had about 1200 flying hours, including 90 hours on the Beech B300. This was also his first flight to Saint-Georges in winter conditions. He was considered a serious and professional pilot.
CRM is the effective use of all resources, including the aircraft and its systems, documentation, computer software, and persons, to achieve the highest possible level of safety. The term "persons" includes the pilots, flight attendants, air traffic controllers, maintenance personnel, regulators, and any other person who may interact with the flight crew. CRM has several elements that include communication, teamwork, and situational awareness. Neither the pilot-in-command nor the co-pilot had taken CRM ground-school training, nor is there any regulatory requirement for the pilots of private companies to take CRM training.
The aircraft was certified, equipped, and maintained in accordance with existing regulations and approved procedures. It had no known deficiencies before the flight, and it was being operated within its weight and balance limits. The width of the main-gear wheelbase is 18 feet, which is half the width of the cleared runway.
The aircraft is equipped with a Collins APS-65 flight control system. It is a sophisticated system that electronically collects the information provided by several instruments, inputs the information into a computer, and shows it on two visual displays. After a go-around, the APS-65 displays the itinerary for the published missed approach. The flight director is normally connected to the autopilot system.
The FCS includes an altitude selection system. When the aircraft is 1000 feet and subsequently 200 feet from the altitude displayed on the altitude selection panel, an audible warning signal sounds and an annunciator light comes on. Examination of the aircraft after the accident revealed that the altitude selection panel was displaying 1100 feet, the radar altimeter was set to 380 feet, and the pilot-in-command's and co-pilot's altimeters were set to 29.55 in. Hg (inches of mercury).
According to the company SOPs, the pilot-in-command is responsible for obtaining weather information before the flight. The pilot contacted the Québec flight information centre (FIC) at approximately 0700 on the morning of the accident and checked the NAV CANADA internet weather site. Because there is no Atmospheric Environment Service weather station at Saint-Georges, the information obtained was peripheral. IFR to marginal VFR conditions were forecast for southern Quebec. It was snowing lightly at Saint-Georges at 0935 on the morning of the accident when the aircraft took off from Saint-Hubert; the cloud ceiling was 200 to 400 feet above the ground. It started to snow heavily at Saint-Georges after the aircraft took off. It was raining at Saint-Hubert when the aircraft landed at 1012. On arrival at Saint-Hubert, the pilot-in-command did not call Saint-Georges to request weather information or runway conditions.
On the approach to Runway 06, the crew established visual contact with the ground at 1500 feet asl and saw the runway lights at approximately ¾ nm from the threshold. Later, on final for Runway 24, conditions had deteriorated to the point that it was becoming difficult to land. The observed ceiling was obscured, and visibility was ¼ nm to ½ nm in heavy snow showers.
The municipality of Saint-Georges owns Saint-Georges aerodrome. The aerodrome is not certified by Transport Canada and is not controlled. Emergency response services are provided by the Saint-Georges Fire Department. Aviation CMP Inc. operates the aerodrome under a contractual agreement. The Aviation CMP Inc. operations manager is responsible for overall aerodrome management. The Aviation CMP Inc. air transport coordinator is in charge of day-to-day aerodrome management. His duties include coordination of snow removal, and of sweeping and clearing the runway. In addition, he is the aerodrome UNICOM radio operator. Since he is not a qualified observer, he can provide only the altimeter setting, wind direction and speed, and runway condition. He could have given the ceiling height and visibility for information purposes only, but he did not do so. Aviation CMP Inc. had not developed a list of exterior references to enable the air transport coordinator to estimate visibility and the cloud ceiling height with greater accuracy, nor was it required to do so.
The aerodrome reference altitude is 893 feet asl. Runway 06/24 is asphalt-covered and is 5108 feet long by 75 feet wide. The final path for Runway 24 requires that the aircraft fly over a valley formed by the Chaudière River, with the runway at the top of the west bank. Saint-Georges is spread out on both sides of the river. Runway 24 is equipped with low-intensity runway lights, threshold and runway end lights, and a type-J aircraft radio control of aerodrome lighting (ARCAL) system. The ARCAL, which can control aerodrome lighting within a radius of 15 nm for 15 minutes, was activated the first time from 17 nm from the runway and again from approximately 10 nm from the threshold. The runway is equipped with category P1 PAPI with a slope of 2.5 degrees, which can usually be seen from a distance of at least 4 nm. When the Runway 24 PAPI became visible, the aircraft was less than ¼ nm from the threshold, and the four lights were white, indicating that the aircraft was too high in relation to the nominal approach slope.
A specialized company contracted by Aviation CMP Inc. does the snow removal at Saint-Georges aerodrome. Normally, snow removal starts immediately after a snowfall or at the request of an aircraft operator. After clearing the snow off the runway on the morning of the accident, the snow-removal vehicle operator left the aerodrome. Before leaving, it was agreed that the runway would be cleared again before C-FMHD returned, which was expected around 1100.
Because clearing snow off the runway normally takes 45 minutes, the air transport coordinator expected that snow-clearing operations would start around 1000. However, runway snow removal started at about 1110. Snow removal continued until C-FMHD was about 1 nm from the threshold of Runway 06. The snow-removal operator did not advise Saint-Georges when he left the runway, and the investigation could not determine whether the runway was clear of traffic when the aircraft reached the MAWP.
The investigation established that the air transport coordinator lost radio contact with the snow-removal vehicle several times during the snow-removal operation because the radio antenna in the snow-removal vehicles did not allow line-of-sight to be maintained for continuous communication with the air transport coordinator. A warning note in the upper left corner of the approach chart reminds the pilot to ensure that the runway is clear of obstructions.
At the time of the occurrence, the centre portion of the runway was cleared to a width of 36 feet with 2 to 3 cm of snow covering the surface. There was a snow bank about 30 cm high on both sides of the cleared area. The remainder of the runway was covered by 7 to 10 cm of snow. The runway information transmitted to the crew by the air transport coordinator indicated that the runway was cleared to a width of 60 feet.
Since Saint-Georges aerodrome does not have a device for measuring runway visual range, there are no regulations prohibiting the crew from attempting an approach. According to Section 602.128 of the Canadian Aviation Regulations (CARs), the pilot should not continue the descent below the MDA if he does not clearly distinguish at least one of the following references during the approach for Runway 24:
- the runway or runway markings
- the runway threshold or threshold markings
- the touchdown area or touchdown area markings
- the approach slope indicator
- the runway identification lights
- the runway edge lights on both sides of the runway
These visual references must enable the pilot to estimate the position of the aircraft and its rate of change of position in relation to the nominal path. The visibility published on the approach chart was 1¼ nm. This visibility is published only for information purposes. It indicates the visibility that should enable the pilot to establish visual contact with the necessary references during the approach and to judge whether it is possible to make a successful landing when he compares this value to the visibility available at the aerodrome.
Amendments to the regulations have been put forward that would constitute an approach ban preventing the flight crew of an aircraft operating a commercial service from continuing the approach if the visibility communicated is below the limit value during the approach.
When the aircraft was on short final, visibility was between ¼ nm and ½ nm. Since the PAPI was located about 500 feet west of the threshold, the co-pilot saw the runway threshold at a distance of ¼ nm. Consequently, at an approach speed of 120 knots, the aircraft flew over the runway threshold approximately 6 to 13 seconds after the pilot saw it.
Aviation CMP Inc. holds a private operator certificate issued by the Canadian Business Aviation Association (CBAA). The operation was subject to subpart 604 of the CARs, Private Operator Passenger Transportation. The company carries the executives and shareholders, and their families, for the six shareholder companies of Aviation CMP Inc. Aviation CMP Inc. operates out of its base at Saint-Georges.
To comply with CBAA requirements, Aviation CMP Inc. developed and implemented a safety management system (SMS) that requires the involvement of all company personnel. The primary objective is to try to manage all risks and situations that could degrade safety by being proactive. The company identified 16 situations and conditions with a risk factor equal to or greater than "moderate-low." The following six elements from the list of risks published in the SMS manual were present on this flight:
| Risk | Risk Evaluation | Means Suggested in SMS to Minimize Risks |
|---|---|---|
| Uncontrolled airport | Moderate | Maintain adequate communication of position reports Check weather by telephone with the airport resource persons |
| Controlled flight into terrain | Moderate | Comply with altitudes |
| Flight management | Moderate-low | Report any change in departure or arrival time |
| Runway maintenance | Moderate | Ground personnel must schedule start of snow removal early and must advise pilot of runway conditions |
| GPS approach | High | All pilots must know procedures and SOPs for GPS approaches |
| Weather | Moderate-low | Telephone reliable person for weather briefing |
The company had supplied each pilot with a cellular telephone so they could comply with the requirements set out in the company operations manual and the SMS manual.
Aviation CMP Inc. has an SOP manual for the Beech B300, which sets out clearly and precisely the tasks of the pilot-in-command and the co-pilot, and of the pilot flying and the pilot not flying, for each phase of flight and for certain specific situations. The company operations manual requires that its pilots follow the SOPs. In fact, the company SOPs and operations manual are integral parts of the safety program.
Among other things, the crew did not follow the procedures related to these elements of the operations manual and SOPs:
- weather briefing before flight
- weather information and runway conditions on approach
- altitude selector set to MDA
- continue the descent below the MDA without visual contact with regulatory references
- approach briefing
- standardized calls on GPS approach
- missed approach procedure
- prohibition on using a runway with over 2 cm of snow
Analysis
The decision to fly the approach was consistent with existing regulations because Saint-Georges aerodrome was not subject to an approach ban. It should also be noted that the proposed approach ban would not have prevented the crew from initiating the approach because the proposed approach ban does not apply to private companies and because the Saint-Georges aerodrome does not meet weather observation requirements. Therefore, it seems that the approach ban does not offer the same level of protection to private operators as it does to commercial operators.
The flight path was not stabilized on the final phase of the approach. Because the snow-covered runway provided little contrast with the surrounding terrain, it was difficult to align the aircraft on the runway centreline. At ¾ nm from the threshold, the aircraft followed an S-shaped path that took it to the south then to the north of the runway. It was not until six seconds before touchdown that the runway became visible. Consequently, given the short period of time between the path correction and touchdown, it is reasonable to conclude that the aircraft was drifting to the left when the wheels touched down. In these conditions, it was difficult to keep the aircraft in the centre of the contaminated runway and to avoid the snow banks created by the snow-removal vehicle and located barely nine feet on either side of the landing gear. The collision of the left gear with the snow bank led to the loss of control of the aircraft.
The Runway 06 approach, go-around, and missed approach were executed in an unsafe manner. The accident occurred after an unstabilized and unsafe approach to Runway 24, followed by a landing on a contaminated runway. Contrary to the company's operating requirements, the crew did not follow company SOPs. Specifically, flight planning was incomplete, the landing limits were not adhered to, the runway contamination limits were ignored, the approach briefings were not conducted in full, and crew coordination was deficient. Consequently, the analysis will focus essentially on the decisions and actions taken by the crew and by Aviation CMP Inc. ground personnel.
In view of the weather information obtained on the morning of the accident, it would have been prudent for the pilot-in-command, before departing Saint-Hubert, to request a weather update and a runway condition report from Saint-Georges. However, for an unknown reason,Footnote 7 the pilot-in-command did not contact Saint-Georges either on arriving at Saint-Hubert or before departing. As a result, the crew took off without knowing that weather conditions had deteriorated considerably and that the runway would not be cleared before their arrival.
If the pilot-in-command had contacted Saint-Georges before take-off, he could have expected to make an approach in heavy snow showers with visibility below the visibility published on the approach chart. He could have anticipated not seeing the runway on completion of the approach and could have planned either to hold at Saint-Georges until the weather improved or divert to another airport. In that case, it would have been reasonable to delay their departure so that they could arrive after the runway had been cleared.
Although they were in radio contact with Saint-Georges 10 minutes after taking off from Saint-Hubert, the crew did not update their information to gain a better awareness of the situation. Because they lacked information, the pilots were unable to assess the impact of the weather on the runway condition and on the chances of executing a successful approach. In fact, the pilot-in-command and the co-pilot never discussed the weather and the runway condition before the accident. Even though the air transport coordinator was not a qualified observer, the pilot-in-command could have asked him to describe the general conditions at the aerodrome. Moreover, the air transport coordinator could have taken the initiative and called the crew to advise that conditions had deteriorated considerably since their departure. He also could have advised the crew that conditions had gotten worse after the first approach was aborted. All the more so because a landing in such conditions was unusual. This information was essential for flight safety.
Both the pilot-in-command's and the co-pilot's altimeters were set to 29.55, whereas the barometric pressure at Saint-Georges was 29.65. Therefore, the altitude displayed by the aircraft's altimeters would have been 100 feet lower than the actual altitude of the aircraft. For that reason, when the aircraft was at the MAWP for the Runway 06 approach, it was 80 feet above the MDA and 100 feet higher than the crew thought. The aircraft was higher than the normal approach and could not descend fast enough to land safely.
After the go-around, the aircraft was not on the correct path in relation to the published missed approach procedure. The aircraft followed an improvised path until the crew was able to program the FCS for the Runway 24 approach. In the absence of approach briefings, it appears that the crew members did not follow the published procedure because they were inadequately prepared and did not follow the instructions displayed on the FCS. And yet, the existing environmental conditions dictated that a full briefing be conducted for each approach.
Because the altimeter setting for Québec increased all the procedure altitudes by 210 feet, it appears that the pilot-in-command set the aircraft's altimeters at what he believed to be the barometric pressure at Saint-Georges. If this is true, either the air transport coordinator transmitted the information incorrectly, or the pilot-in-command heard it incorrectly. Although the incorrect setting of the aircraft's altimeters increased the obstruction clearance margins, an altimeter error could also reduce them and lead to a catastrophe, particularly in the conditions that existed at the time of this occurrence.
The setting error was not noticed in the 36 minutes that preceded the accident. The error was not noticed because the altimeter setting was transmitted by Saint-Georges only once, 10 minutes before the start of the Runway 06 approach. Because the aircraft was in controlled airspace, the co-pilot was monitoring another frequency, that of Montréal Centre; consequently, he was unable to note an incorrect display. In any event, it would have been prudent to obtain an update of the altimeter setting on each approach, because the crew had been advised earlier that the barometric pressure at Québec was falling fast.
After the missed approach, the crew undoubtedly suspected that an RNAV approach for Runway 24 within the limitations would not enable them to land the aircraft in the existing weather conditions. It is probable that this reasoning led the crew to set the altitude selector to 1100 feet, 200 feet below the MDA, before arriving at the FAWP. Therefore, it is reasonable to conclude that the pilot-in-command decided to descend below the MDA even if visual contact with the required references had not been established in order to improve the chances of seeing the runway.
The chances of completing the approach safely diminished as the aircraft, in descent, got closer to the aerodrome without the crew having acquired the required ground references. As a result, another action plan was urgently needed. Since the crew was not following the published approach procedure, and no plan had been made, they had not determined the point at which the approach should be aborted. Therefore, they had no common plan regarding a possible missed approach, which is the most dangerous phase of an approach. These decisions suggest that, even before arriving at the FAWP, the pilot-in-command had resolved to land at the end of the approach.
Both pilots made basic flight management errors in accomplishing routine tasksFootnote 8 and in evaluating existing conditions. For these reasons, the crew's performance can be described as non-standard. Their performance was not consistent either with the level of performance expected of each one or with the fact that, as new employees, both had just been trained in the company's standards and procedures, nor was it consistent with the pilot-in-command's past experience as a chief pilot. Furthermore, their behaviour was not consistent with their reputations as conscientious and professional pilots.
Despite the indications that the weather had deteriorated, the crew never discussed the possibility of executing a missed approach, flying a holding pattern, or diverting to an alternate airport. It appears that the intention to land without delay distracted the pilots and, as a result, affected their ability to assess the situation correctly and make appropriate decisions. The situational stress and deficient management of cockpit resources appear to be at the origin of the crew's inadequate performance.
There is no indication that the company pressured pilots to descend below the minima. On the contrary, Aviation CMP Inc. had put in place recognized means for improving flight safety, including an SMS and SOPs, and contracted with CAE Simuflite to provide CRM and CFIT training for its pilots.
The flight did not result in a CFIT event. However, the decision to descend below the MDA in low visibility and heavy snow showers was conducive to a CFIT event. At 3 nm from the runway, the aircraft was a little more than 200 feet agl (1200 feet asl)Footnote 9 and at 1 nm, it was 100 feet above the runway elevation (1000 feet asl). At less than 100 feet agl above the threshold, relying on what the co-pilot indicated, the pilot-in-command decided to continue the descent even though he could not yet see the runway.
The crew's non-compliance with procedures and regulations as described reveals a lack of coordination and an absence of rigour. From these facts, it can be concluded that the crew did not follow CRM principles. During their training at CAE Simuflite, when they were operating with a pilot from outside Aviation CMP Inc., their CRM performance was deemed satisfactory. Since neither of them had theoretical CRM training, it is reasonable to believe that together they did not have the theoretical knowledge required to apply CRM principles.
The presence of 6 of the 16 risk elements from the company's SMS manual (as previously identified) should have made the crew members aware of the dangers of the situation and reinforced a prudent attitude. However, the pilots did not seem to recognize these conditions, and they did not adopt the company's risk reduction strategies. For that reason, the pilots demonstrated an inadequate knowledge of the SMS program.
To allow the aircraft to land after the Runway 06 approach, snow-removal operations were suspended 15 minutes after they had begun. Consequently, only half of the runway width was cleared, and 30 cm snow banks were left on either side of the cleared section. However, because he was relying on the information received at 1115, the pilot-in-command believed that the runway was cleared to a 60-foot width. This misunderstanding continued because the crew did not request an update and the air transport coordinator did not provide an update. The fact that the pilot-in-command asked the air transport coordinator to confirm that the runway was clear after the Runway 06 go-around indicates that he had decided to attempt a landing knowing that the snow-removal vehicle was perhaps on the runway. A landing in these conditions was risky because the visibility of ¾ nm and the physical characteristics of the runway restricted the pilots' visual range and, therefore, their ability to see the vehicle in time to avoid it.
Snow-clearing operations were not resumed because the crew decided to make another approach without delay. Since the crew did not request an update on the runway conditions, the decision to land was based on inaccurate, incomplete, and obsolete information.
The investigation established that the ground personnel suspected that the conditions were highly unfavourable for a safe landing. Under the SMS program, the accumulation of the following indicators ought to have induced the ground personnel to ask the crew to review their decision to land:
- low visibility
- obscured cloudy ceiling
- heavy snow shower
- runway half cleared of snow
- snow banks on the runway
- accumulation of snow on the cleared portion of the runway
The air transport coordinator, as the person in charge of day-to-day operations at Saint-Georges aerodrome, could have shut down the runway until the snow was removed. Consequently, it can be concluded that the Aviation CMP Inc. ground personnel did not put into practice the company's SMS philosophy and showed a lack of assertiveness by not intervening when the crew decided to land in unfavourable conditions.
Findings
Findings as to causes and contributing factors
- Because the aircraft's trajectory was not stabilized on the final phase of the approach, the aircraft was drifting to the left when the wheels touched down. The pilot-in-command was unable to keep the aircraft in the centre of the snow-covered runway, which had been cleared of snow to only 36 feet of its width.
- The left main landing gear, then the nose wheel, struck a snow bank left on the runway by the snow-removal vehicle, and the pilot-in-command was unable to regain control of the aircraft.
Findings as to risk
- Aviation CMP Inc. pilots and ground personnel demonstrated inadequate knowledge of the safety management system program by not recognizing the risk elements previously identified by the company.
- Neither the pilot-in-command nor the co-pilot had received training in cockpit resource management (CRM), which could explain their non-compliance with procedures and regulations.
- Knowing that a snow-removal vehicle might be on the runway, the crew attempted to land on Runway 06 and, after the missed approach, the aircraft did not follow the published missed approach path.
- On the Runway 24 approach, the crew descended below the minimum descent altitude (MDA) without having acquired the required references.
- The aircraft's altimeters were not set on the altimeter setting for Saint-Georges.
Other Finding
- The proposed approach ban would not have prevented the crew from initiating the approach because the proposed ban does not apply to private companies and because Saint-Georges aerodrome does not meet the meteorological observation requirements.
Safety action
Following this accident, Aviation CMP Inc. modified its company organization chart. The position of assistant director of operations was created to provide leadership at the company's main base when the director of operations is absent. Also, the company appointed a chief pilot for the Lear 60 responsible for the Montréal base, and check pilots were appointed for the Lear 45, the Lear 35, and the Beech B300.
Aviation CMP Inc. established new criteria for runway acceptability. No approaches will be allowed until the runway is fully cleared of snow and is clear of traffic. A runway report for Saint-Georges aerodrome will be provided to the flight service station and sent to the pilot where possible.
Aviation CMP Inc. established visual references to enable UNICOM personnel to estimate as accurately as possible the visibility and cloud ceiling at Saint-Georges aerodrome. Furthermore, to avoid any confusion as to the snow-removal need, a call sequence was established to reach snow-removal employees. Also, the radio equipment in the snow-removal vehicles at Saint-Georges was modified to allow communication with the base and aircraft at all times.
Aviation CMP Inc. will provide an annual winter operations awareness program for its pilots and ground personnel.
The Canadian Business Aviation Association modified its symposium education program to promote a better understanding of the factors that lead pilots (and others) to not follow established procedures.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .