Loss of Control and Collision With Terrain
Northern Air Support Ltd.
Bell 206L4 C-FVEF (Helicopter)
Three Valley Gap, British Columbia
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The Bell 206L4 helicopter, registration C-FVEF, serial number 52071, took off from Kelowna, British Columbia, at 1710 Pacific daylight time, with only the pilot on board. The helicopter was on a visual flight rules flight to Rocky Mountain House, Alberta, with an intermediate refuelling stop at Golden, and was expected to arrive in Golden at about 1830. The planned route from Kelowna to Golden was abeam Vernon, to follow the powerlines through Silver Star Provincial Park and Trinity Hills to Three Valley Lake, then to follow the published visual flight rules route to Revelstoke and on to Golden.
When the helicopter did not arrive in Rocky Mountain House that evening, company personnel alerted the Rescue Coordination Centre in Victoria, and a search was begun. The search was impeded by low cloud and reduced visibility. The helicopter wreckage was located three days after the accident at 3700 feet above sea level, about one nautical mile southeast of Three Valley Lake. The accident occurred at approximately 1749, in daylight and possibly poor weather conditions. The pilot was fatally injured and the helicopter was destroyed. The emergency locator transmitter activated upon impact and transmitted a signal; however, the antenna adapter was severed by impact forces and the signal was attenuated and thus ineffective. There was no fire.
Factual information
The helicopter was operated by Northern Air Support Limited based in Kelowna and was being ferried to Rocky Mountain House. After departing Kelowna airport in the afternoon on the day of the accident, the helicopter flew northeast through the Mabel Lake valley, about 45 nautical miles northeast of Kelowna, before following the powerlines that led to Revelstoke (see Figure 1). This route was not in accordance with the one originally planned during pre-flight briefings in Kelowna. It could not be determined why the pilot chose to deviate from this original routing. Weather conditions in the Silver Star area at the time leading up to the accident did not preclude the use of the planned route.
An analysis of the on-board navigation system data reveals that the last recorded track was 046° magnetic at 1749 Pacific daylight timeFootnote 1 on the day of the accident, at an altitude of 3730 feet above sea level. Furthermore, the data show that Revelstoke airport had been selected as the next (or destination) waypoint, and that it was 10.5 nautical miles (19 km) from the last recorded position. The Revelstoke airport is 053° magnetic and 10.5 nautical miles directly from the accident site.
About 50 minutes after C-FVEF took off from Kelowna, a second Northern Air Support helicopter (C-FAHS) took off from Kelowna to fly the same filed route to Rocky Mountain House. The pilot of C-FAHS obtained a weather briefing from the Penticton Flight Service Station at 1738. The only significant en route weather condition was expected to have been in the Revelstoke area, where the ceilings were forecast to have been at about 6000 feet. The pilot later reported that the weather conditions in Three Valley Gap, at the time he flew through that area, had been suitable for a visual flight rules flight, but the segment of the route that followed the powerlines up the rising terrain from the southeast valley had been marginally passable. As well, there had been a moderate upslope wind along the powerline route which had some turbulence associated with it.
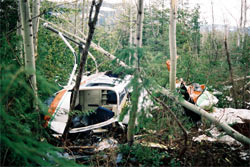
As a result, the pilot of C-FAHS abandoned the direct route along the powerlines to Revelstoke and followed the visual flight rules route along the road that passed through Three Valley Gap without further difficulty. The accident site was on the route segment that followed the powerlines upslope, and was about 100 metres west from the powerlines; in that area, the powerlines follow a path of about 040/220° magnetic (see Photo 1). The pilot of C-FAHS did not encounter any form of precipitation or icing conditions in the Three Valley Gap area. The pilot did observe that the ground in the higher elevations near the powerlines was partially covered with snow but that there was no freshly-fallen snow.

A review of the weather records for the area shows that the freezing level was between 10 000 and 12 500 feet above sea level, and that significant thunderstorm activity was forecast, with winds gusting to 40 knots and visibility four miles in rain and hail. To the west, embedded cumulonimbus clouds were expected, producing rain and low ceilings.
Actual weather reports from the automated weather recorder at the Revelstoke Airport (elevation 1453 feet above sea level) show that during the time surrounding the accident, the weather had begun to deteriorate. At 1800, clouds were recorded at 3800 and 4500 feet above ground level, with a ceiling at 5500 feet; the wind had changed from a southerly direction to 350° True at 12 knots, and the temperature was 19°C.
It was consistently reported by several ground witnesses that, at approximately the time of the accident, there were low clouds, thunderstorms, high winds, heavy rain, and low visibility in the vicinity of Three Valley Lake, which is at 1680 feet above sea level. This area, where the valleys narrow and merge, is known to be a local meteorological hazard area, producing low cloud, heavy snow, and unpredictable winds.Footnote 2
Although the wreckage was extensively damaged by impact forces, all helicopter and rotor system components were found at the accident site. The airframe had broken into three main sections: the main fuselage up to the cargo compartment bulkhead; the cargo compartment section; and the tail boom. No indication of either main or tail rotor blade contact with the airframe was found. In summary, no indication of any pre-existing airframe defect, engine malfunction, or system deficiency was found. The wreckage exhibited damage patterns characteristic of impact with trees and terrain while the helicopter was in a left-side-down attitude in the order of 60° to 70° angle of bank (see Photo 2).

The continuity of the flight controls and drive train components was established. The main rotor and tail rotor gearboxes, the engine freewheel unit, and the hydraulic flight control system were examined and functionally tested, where applicable; no malfunction, contamination, or mechanical anomaly was found. The fuel control unit has a pointer and markings at 0, 10, 40 and 100 that indicate throttle position. When the pointer is at 40 the engine is at idle. For flight power, the pointer would be at about 100. The pointer was found at what would be about 25 (below idle). At a throttle position of below 40, the engine shuts down.
The Transportation Safety Board (TSB) Engineering Branch examined the cockpit instruments and annunciator panel (LP045/2002) and found that the engine-out warning light was not illuminated. The following light bulbs exhibited damage characteristics consistent with them having been illuminated at impact:
| Light Caption | Indication | Likely Fault Condition |
|---|---|---|
| LITTER DOOR OPEN | Red | Litter door not latched |
| BAGGAGE | Amber | Baggage door not latched |
| GEN FAIL | Amber | Generator not ON |
| TRANS OIL PRESS | Amber | Transmission oil pressure below 30 psi |
| ROTOR LOW RPM | Amber | Rotor rpm below 92% |
The litter door open and the baggage door open caution lights are triggered by micro switches on the fuselage. The generator fail light illuminates if the engine or generator fails, if the generator switch is turned off, or if engine rpm (Ng) decreases below about 40%. The generator was bench tested and found serviceable, and there was no reason found for the generator fail light to have been on. The generator switch was found in the OFF position, but the first responders reported that they turned the battery and generator switches off as a precaution. By design, the transmission low-oil-pressure warning light in the Bell 206 helicopter illuminates when the pressure drops below 30 psi; this occurs at a main rotor rpm of approximately 50% or below. The rotor low rpm caution light comes on when the rotor rpm drops below 92%. The helicopter will become uncontrollable if the main rotor rpm drops below a certain rpm; this could be about 70 to 75%, depending on the skill of the pilot and the flight conditions.
The TSB Engineering Branch examination of the light bulbs identified that such light bulb filaments only need to be illuminated for a brief time before impact (in the order of 50 milliseconds) to show that they were 'ON' at impact.
The fuel tank had not ruptured and was found to contain jet turbine fuel. About 90 gallons of fuel was drained from the tank after the accident, and a fuel sample test revealed no contamination. The pilot had replenished the fuel tank to capacity immediately before departing Kelowna. Tests of the fuel samples taken from the airframe fuel system and engine fuel filters of the accident helicopter were unremarkable and revealed no contamination. The company helicopter following C-FVEF had refuelled from the same fuel supply in Kelowna that afternoon and experienced no fuel-related anomalies during the flight to Rocky Mountain House. Neither fuel quality nor quantity are considered contributing factors in this accident.
The cyclic and collective control sticks were fractured to the left, consistent with left-side impact, and the throttle twist-grip was severed from the collective by impact forces. The base and back to the pilot's seat had broken away from the attachment points on the fuselage, as had the 4-point seat restraint system, in a direction consistent with left-side impact with the terrain. The TSB Engineering Branch examined the seat restraint system and determined that the combined forward and sideward load experienced by the aircraft at impact was in the order of 19 to 24 g,Footnote 3 which exceeded the certification and design criteria. There was no indication of premature failure of the pilot's seat restraint system or its attachment points.
Damage to the helicopter is consistent with high deceleration forces - further evidenced by the seat restraint system damage - and a left-side-down attitude at impact. Such impact forces exceed human tolerance and, accordingly, the accident was not survivable.
The emergency locator transmitter (ELT) was permanently mounted on the inside left-hand nose section of the cockpit. Impact forces dislodged the ELT unit from its mounting cradle, shearing off the external antenna adapter. As a result, even though the ELT activated, the transmitted signal could radiate only a few feet, and thus prevented detection by SAR satellite or airborne search radio equipment.
C-FVEF was manufactured in 1994 in accordance with aircraft Type Certificate H-92 approved by Transport Canada on 02 February 1993. The helicopter was neither fitted with dual flight controls nor configured for flight in instrument meteorological conditions; it was not required by regulation to have been so equipped. The total airframe in-service time was about 5194 hours on the day of the accident. The most recent 100-hour mechanical inspection was completed at 5117 hours on 12 October 2001, 220 days before the accident. A review of the logbooks and maintenance records indicates that the helicopter had been certificated, equipped, and maintained in accordance with existing regulations and approved procedures.
The engine was a (Rolls Royce) Allison 250-C30P gas turbine (serial number CAE895748). Engine maintenance records reveal that the engine had been maintained in accordance with existing regulations and approved procedures. Impact signatures and the damage to the engine were characteristic of an engine striking terrain while delivering low power at impact. TSB investigators removed the engine from the airframe and conducted static and dynamic examinations and tests at an approved engine maintenance and overhaul facility. During the crash, the compressor had sucked in some pieces of aluminum; there was some melted aluminum in the burner cans, but it had not all melted. Engine performance in the test cell conformed with the engine manufacturer's specifications. Accordingly, it was concluded that the engine was capable of delivering rated power for the accident flight.
The maximum certificated all-up weight (MAUW) of the Bell 206L4 helicopter is 4450 pounds. Records show that C-FVEF was last weighed on 29 August 2001 and the aircraft empty weight was then calculated to have been 2561 pounds, with a centre of gravity of 128.58 inches aft of the datum. Weight and balance calculations performed by the TSB, using a full fuel load and the actual weights of the pilot and the cargo carried, show that at take-off from Kelowna, the helicopter was about 3700 pounds with a centre of gravity of about 126 inches aft of the datum, within the approved weight and balance limits. Weight and balance were not considered factors in this accident.
The pilot held a Canadian commercial licence-helicopter, issued by Transport Canada, and valid for Bell 47, Bell 206, Hughes 500, and Robinson R22 and R44 helicopters. The licence was endorsed for daylight flying only and the pilot did not hold an instrument rating, nor was it required for the type of flying in which he was engaged. The pilot held a Class 1 Medical Certificate which included a limitation requiring that glasses or contact lenses be worn. The pilot was wearing contact lenses at the time of the accident.
Records show that as of May 2002, the pilot had accumulated more than 1600 hours total helicopter flying time, of which about 650 hours were on helicopters similar to the accident type. About 980 hours were on other types, the majority of which was in heli-logging as a co-pilot on medium helicopters. The pilot had passed a pilot proficiency check on the accident helicopter in March 2002, and had flown a total of 20 hours on it. The pilot had flown most recently 17 days before the accident flight and had accumulated 22 hours in the last 90 days. A review of the pilot's flight and duty time record reveals that it was in accordance with existing regulations, and nothing remarkable was found regarding the pilot's activities in the previous 48 hours. Records of the pilot's flight experience show that most of his flying had been conducted in the mountainous regions of British Columbia, with a large portion in the Revelstoke-Mica Creek area.
The following TSB Engineering Branch projects were completed:
- LP045/2002 – Instrument Panel Examination
- LP046/2002 – Examination of Separated Safety Belts and Shoulder Harness
- LP060/2002 – Drive shaft Examination
Analysis
The characteristics of the damage to the helicopter and the damage found to the trees and terrain, at and around the accident site, indicate that the helicopter was in a steep, left-bank, and slightly nose-down attitude as it passed through the trees and struck the terrain. Such an extreme attitude is not consistent with controlled flight and indicates that the pilot had lost control of the helicopter before impact with the trees.
It is possible that the pilot encountered poor weather and lost visual reference to the ground. He did not have an instrument rating, and the helicopter was not equipped with an artificial horizon instrument or a stabilization system, greatly increasing the risk that the pilot would lose control of the helicopter if it entered cloud. Loss of control could also occur because the pilot, for unknown reasons, allowed the rotor rpm to decrease to the point where the helicopter could no longer be controlled. In either case, it is apparent that the helicopter was not high enough to allow control to be recovered before tree/ground impact.
The litter and baggage doors were, in all likelihood, closed and presumably the lights were out during flight; however, the lights for the litter and baggage doors were illuminated at impact. It is probable that the doors moved enough during the initial impacts with the trees/ground to cause the switches to activate the lights. The generator fail warning light would have illuminated in flight had the generator failed; however, no anomaly with the generator was found. The generator light could also have illuminated had the generator ceased to operate because of low engine rpm (below about 40% Ng), or as a result of fuselage break-up at impact with the terrain. The cause of the illuminated generator warning light could not be determined. The transmission oil pressure light would illuminate if the main rotor rpm dropped below approximately 50%, as could be the case during the rotor impacts with the trees and the ground. The rotor low rpm light would illuminate because the rotor rpm dropped below 92%, either before or after the pilot lost control.
It was determined that the engine was operating at low power during ground impact, as indicated by engine damage, the melted aluminum in the burner cans, and the engine-out light not being illuminated at the time of impact. The position of the fuel control pointer indicates that the engine was shut down at impact; however, it is probable that the pointer moved during ground impact and the break-up of the helicopter.
The helicopter entered the trees with enough rotor/engine energy to cleanly cut through some fairly large-diameter trees; however, it cannot be stated with any certainty what the rotor rpm was at the time of the initial tree strikes. The damage to the rotor blades was consistent with high coning angle and high blade pitch angle at the time the damage was made. In level flight, these would be an indication of low rotor rpm; however, as the helicopter entered the trees at a bank angle of about 60°, the rotor blades contacting the ground immediately before impact would also result in coning and high blade pitch angle. Although no definite value of the rotor rpm could be ascertained, the transmission low oil pressure light being on indicates that the rotor rpm, at or immediately before impact, was likely below 50%. The tail rotor damage indicates that the tail rotor rpm was fairly low at ground contact, although there are indications that it was higher during initial contact with the trees.
The permanent mounting position of the ELT on this helicopter exposed the unit to severe and unmitigated impact forces which rendered it ineffective. Had the ELT been mounted in an area which was less vulnerable to impact, it may have survived the accident and assisted the SAR efforts in locating the wreckage sooner.
Findings
Findings as to causes and contributing factors
- The pilot lost control of the helicopter for undetermined reasons, and it struck the ground.
Findings as to risk
- The mounting location of the emergency locator transmitter was vulnerable to impact damage, and, as a result, the external antenna adapter was sheared off at impact. The lack of an ELT signal prevented the SAR efforts from quickly detecting and locating the wreckage.
Other findings
- The degree to which weather conditions contributed to this occurrence could not be determined.
- The engine was found to have no mechanical defects and to operate normally, and it was operating at ground impact.
Safety action
Safety action taken
As a result of this investigation, the TSB issued a Safety Advisory to Transport Canada stating that Transport Canada may wish to review the regulations and standards regarding ELT mounting locations and how they are interpreted and applied.
Safety concern
Transport Canada responded to the advisory stating that they had determined that a relocation of the ELT in this case would not have necessarily made a difference with regard to the integrity of the antenna.
The Board remains concerned that the signal from an ELT is compromised by the location of its installation in some cases, and that the nose-mounting location of the ELT may be more vulnerable to impact forces than the centre-post location.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .