Runway overrun
Inter-Canadien
Fokker F28 Mk 1000 C-GTIZ
St. John's, Newfoundland
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content. Masculine pronouns and position titles may be used to signify all genders to comply with the Canadian Transportation Accident Investigation and Safety Board Act (S.C. 1989, c. 3).
Summary
The aircraft, designated Inter-Canadien Flight 2210, had completed a localizer approach to Runway 16 at St. John's Airport, Newfoundland, in night instrument meteorological conditions. Runway 16 had a displaced threshold that reduced the useable length from 7000 feet to 5530 feet, and the surface was wet, with no standing water. The aircraft touched down at 118 knots approximately 1200 feet past the displaced threshold. The crew were unable to stop the aircraft on the runway, and the aircraft came to rest approximately 420 feet beyond the runway end. During the runway excursion, the nose gear collapsed. Of the 56 passengers and the 4 crew members on board, 5 passengers and 2 crew members suffered minor injuries.
1.0 Factual Information
1.1 History of the Flight
1.1.1 Pre-flight
The crew reported to company dispatch in Halifax, Nova Scotia, at approximately 2015 Atlantic daylight time (ADT) and were provided with weather information, notices to airmen, weight and balance documentation, and a list of deferred maintenance items. One of the deferred maintenance items included the lift dumper system, which had been disabled, as allowed under the aircraft's minimum equipment list. The appropriate landing performance tables were provided.
1.1.2 En Route
The aircraft, Inter-Canadien Flight 2210 (ICN 2210), a Fokker F28 Mk 1000, departed Halifax at 2131 ADT on a scheduled flight to St. John's, Newfoundland. On board were 2 pilots, 2 flight attendants, 55 passengers, and a deadheading company pilot, who was in the cockpit jump seat.
The trip from Halifax to St. John's was unremarkable. The visibility favoured an approach to Runway 16; however, an approach to Runway 34 was available. ICN 2210 requested an approach to Runway 16.
At 2220 Newfoundland daylight time (NDT), a BAe 146 crew reported seeing the airport lights at 1000 feet above sea level (asl) on the approach to Runway 16. The crew of ICN 2210 notified the area control centre that they would continue with the Runway 16 approach and that they would attempt an approach to Runway 34 if they missed the first approach. The captain briefed for the Localizer 16 approach, specifying the beacon crossing altitude of 1600 feet and the minimum descent altitude (MDA) of 1000 feet. Upon being cleared for descent to 4000 feet, the descent checks were initiated, and the crew calculated a reference speed (Vref) of 120 knots indicated airspeed (KIAS).
1.1.3 Approach
The aircraft's flight profile was reconstructed using information from the flight data recorder (FDR) and air traffic control radar. At 2316, the aircraft was cleared for the straight-in localizer approach to Runway 16, and 11° of flap was selected. At 2317, the autopilot malfunctioned and was disconnected; the captain hand-flew the aircraft for the remainder of the approach. At about this time, the area control centre reminded the crew that the threshold was displaced and instructed them to switch to the St. John's tower frequency. The gear was extended, followed by flap-25 selection in descent through 2000 feet. The tower reported the winds at 240 ° magnetic (°M) at 5 knots. The tower also reminded the crew that the threshold was displaced by 1470 feet, with the edge lights and the threshold lights commencing from the displaced threshold. As part of the landing checks, the crew confirmed that the lift dumpers were not available and that the antiskid system was checked and armed.
The aircraft crossed the beacon at the crossing altitude, heading 169°M at 154 KIAS. The descent to the MDA of 1000 feet asl was initiated, and the descent rate reached a maximum of 1300 feet per minute (fpm). Two nautical miles (nm) from the displaced threshold, the aircraft levelled off briefly at the MDA, at 150 KIAS. The aircraft then descended to approximately 900 feet, which it maintained for the next 13 seconds. The crew sighted the runway environment 1 nm from the displaced threshold. The captain reduced power and indicated that they would land. Flap 42 was selected, and the descent for landing was initiated. The descent angle and rate varied, reaching maximums of − 5° and 1500 fpm. A normal descent angle and rate is about − 3° and 700 fmp. The ground proximity warning system (GPWS) repeatedly warned of excessive sink rate at approximately 300 feet above ground level (agl). The crew deactivated the GPWS warning and continued the descent. The power reached idle as the aircraft crossed the actual runway threshold at 200 feet agl, heading 164°M at 152 KIAS. In accordance with standard operating procedures (SOPs) for this aircraft, speed brakes were selected out at approximately 100 feet agl.
The aircraft crossed the displaced threshold at 80 to 90 feet agl, with the power at idle and speed decreasing through 138 KIAS; this was 35 feet and 18 KIAS above the desired profile. The aircraft touched down smoothly, at 118 KIAS, approximately 1200 feet beyond the displaced threshold.
1.1.4 Landing Roll
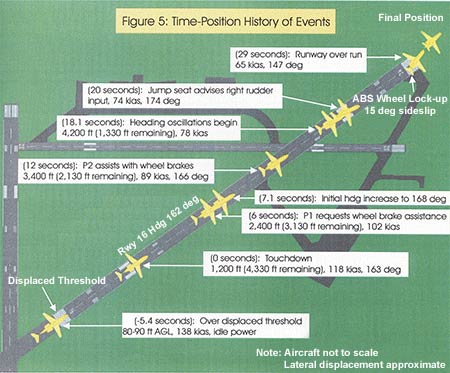
As the main gear touched, the aircraft's heading gradually began to increase from 163°M, reaching 168°M seven seconds after touchdown. The nose gear touched two seconds after the main gear, and the captain applied the brakes. Six seconds after touchdown, the captain perceived that there was no braking action and urgently requested wheel-braking assistance from the co-pilot. The aircraft was now approximately 2400 feet beyond the displaced threshold and decelerating through 102 KIAS, on a heading of 168°M. The aircraft continued down the runway, near the centreline, with the nose 4° to 7° to the right of the runway heading. Maximum toe braking was applied continuously throughout the roll, and the crew reported applying the alternate braking system approximately 2900 feet from the runway end; however, there was no discernable braking effect from either brake system. The co-pilot confirmed toe braking application about 12 seconds after main-gear touchdown, 3400 feet from the displaced threshold (2130 feet from the runway end) at 89 KIAS. Approximately 1330 feet from the runway end, the first of two heading oscillations began. The aircraft's heading increased from 170 °M to 178°M, then decreased to 147°M.The aircraft departed the end of the runway, slightly left of the centreline, on a heading of 147°M at 65 KIAS. (See Appendix A for a schematic of the landing.)
In response to the abnormal landing, the cabin crew gave "brace" commands from their seats after the initial touchdown. As the aircraft approached the runway end, the tower controller activated the airfield crash alarm.
During the overrun, the aircraft nose gear broke off, and the aircraft continued forward, skidding on its nose. The aircraft stopped 420 feet past the end of the runway, slightly left of the extended runway centreline. The engines were shut down, the engine fire extinguisher bottles were discharged, and the electrical power was turned off.
During the shutdown, the captain attempted to order an evacuation over the public address (PA) system and also attempted a radio transmission to air traffic control. These communications were not captured on the cockpit voice recorder and went unheard, likely because the electrical power had been previously turned off. Because the cabin crew did not hear an order from the cockpit to evacuate and no threat to life was observed, they told the passengers to remain seated. When the cockpit door was opened, the captain realized that the cabin crew had not heard his command to evacuate and ordered an evacuation. The forward left door would not open fully downward because the nose of the aircraft was resting on the ground; therefore, all passengers and crew exited via the forward right door. Emergency response vehicles arrived during the initial stage of the evacuation, approximately one minute after the overrun. The over-wing exits were opened as instructed by the aft flight attendant, but they were not used for exiting.
1.2 Injuries to Persons
| Crew | Passengers | Others | Total | |
|---|---|---|---|---|
| Fatal | - | - | - | - |
| Serious | - | - | - | - |
| Minor/None | 4 | 56 | - | 60 |
| Total | 4 | 56 | - | 60 |
1.3 Damage to Aircraft
The nose gear was torn off as it struck debris in the overrun area, and structural damage occurred in the area of the wheel well. The left wing received minor damage to the leading edge when it struck the localizer antenna. Several aircraft antennas were damaged, as was the skin on the aircraft belly.
1.4 Other Damage
The localizer antenna was knocked over when struck by the aircraft's left wing. Some hydraulic fluid spilled when the nose-gear hydraulic lines were torn.
1.5 Personnel Information
| Captain | First Officer | |
|---|---|---|
| Age | 39 | 42 |
| Pilot Licence | ATPL | ATPL |
| Medical Expiry Date | October 1999 | October 1999 |
| Total Flying Hours | 14 000 | 10 276 |
| Hours on Type | 350 | 301 |
| Hours Last 90 Days | 172 | 147 |
| Hours on Type Last 90 Days | 172 | 147 |
| Hours on Duty Prior to Occurrence | 4 | 3 |
| Hours Off Duty Prior to Work Period | 27 | 27 |
1.5.1 Flight Crew
The captain had been employed by the company for nine months and had qualified on the aircraft type in December 1998. His medical certificate and his pilot proficiency check were valid, and he had completed all the required training. The first officer had also been employed by the company for nine months and had qualified on the aircraft type in February 1999. His medical certificate and his pilot proficiency check were valid, and he had completed all the required training.
1.5.2 Cabin Crew
The forward flight attendant had approximately one year of experience and was qualified on ATR 42 and F28 aircraft. She was the designated in-charge flight attendant and was seated in the forward jump seat at the time of the accident. The aft flight attendant had similar experience and the same qualifications as the forward flight attendant. She was seated in the aft jump seat at the time of the accident.
1.6 Aircraft Information
| Manufacturer | Type and Model | Year of Manufacture | Serial Number | Total Airframe Time | Engine Type (number of) | Maximum Allowable Take-off Weight |
|---|---|---|---|---|---|---|
| Fokker | F28 Mk 1000C | 1976 | 11099 | 16 996 hours | Rolls Royce Spey MK 555-15 (2) | 66 500 pounds |
1.6.1 General
The Fokker F28 is a 65-passenger aircraft with twin turbofan engines mounted on the tail. The aircraft is equipped with a tail-mounted speed brake but no reverse-thrust capability. There are two main cabin doors, L1 and R1, on either side of the fuselage, just aft of the cockpit, and two over-wing emergency exits. The left cabin door (L1 door) is hinged on the bottom and has integral stairs. The R1 door is the service door on the right side of the aircraft. The aircraft cabin was configured for 10 business-class seats and 45 economy-class seats. There are two forward-facing jump seats: one adjacent to the R1 door, a second mounted on the rear bulkhead.
The wings are fitted with lift dumpers: the five panels on each wing can deploy automatically or be manually deployed after landing. The lift dumpers shed lift from the wings, increasing the weight on the wheels. This enables the wheel brakes to be used to full advantage during the entire landing run.
1.6.2 Aircraft Maintenance
Six flights before the occurrence flight, the occurrence crew had noted a problem with the lift dumpers' auto-deployment mode. Company maintenance personnel did not have sufficient opportunity to troubleshoot the system and elected to deactivate the automatic and manual deployment modes, as allowed under the minimum equipment list. As a result, the lift dumpers were unavailable for landing on the occurrence flight and on the previous five flights.
Other minimum equipment list deferred items included the following: the autopilot, which was "hunting" but which was usable during portions of the flight; the auxiliary power; and the N0 2-engine high-pressure-valve indicator. All minimum equipment list entries were made in accordance with recognized procedures. The crew were aware of the deferred items and received appropriate pre-flight documentation relating to the aircraft's decreased landing performance.
1.6.3 Braking Systems Description
The main-wheel brakes are controlled by two systems, designated "normal" and "alternate". Both systems are mechanically selected and hydraulically operated. Normal braking is selected by depressing toe brakes on either the pilot or co-pilot pedals. The normal brake system is supplied by hydraulic system N0 1 and contains an electrically controlled antiskid system. Alternate braking is selected by the captain through use of two hand-operated controls on the left side panel. The alternate brake system is supplied by hydraulic system N0 2 and does not have an antiskid capability.
The antiskid system incorporates touchdown protection circuits that prevent a locked wheel on touchdown by supplying a full "dump" signal to the brakes while the weight-on-wheels switches are in the flight position. This aircraft had been modified with Service Bulletin (SB) F-28/32-116 on 01 March 1983. This modification incorporates a seven-second delay for braking after weight on wheels to give further touchdown skid protection. The seven-second delay is cancelled as soon as the wheels spin up on touchdown. All Inter-Canadien / Air Canada Regional Inc. commercial F28 aircraft have been modified in accordance with SB F28/32-116.
1.6.4 Braking Systems Testing
After the accident, none of the brake assemblies exhibited signs of overheating, and there was no indication of a pre-occurrence fluid leak. Both sets of rudder pedals were unobstructed, and toe brake travel was normal on the pilot and co-pilot sides. The parking brake selector operated normally and was in the stowed position after the occurrence. The antiskid selector was found in the "armed" position. The normal and emergency accumulators both contained the required system pressure.
The following brake and antiskid components were tested and met the manufacturer's specifications: wheel speed generators, dual antiskid control valves, ground flight relay switches, antiskid control box, parking brake mechanism, and associated electrical circuits, hydraulic systems, and cable tensions. Individual components were removed and bench tested. Environmental conditions encountered during the flight could not be duplicated during the bench testing. The tests revealed that the antiskid control box was supplying an anomalous voltage to the right-hand inboard wheel antiskid control valve. This anomalous voltage would have reduced braking to this wheel by 30%. Anomalies were also found in other components; however, these other anomalies would not have resulted in a noticeable reduction in braking performance. No discrepancies were noted that would have resulted in a total lack of braking.
1.6.5 Main-wheel Tires
The four main-wheel tires were inspected after the accident. Each tire had a 0.37-inch tread channel, was properly inflated, and was in generally good condition; however, some damage was incurred during the landing roll and the overrun. Each tire had similar damage: a single flat spot approximately 12 inches long and 10 inches wide, worn down to the depth of the tread channel. The overall surface of the flat spots exhibited the mottled appearance of tread rubber that had undergone reversion due to moderate overheating. This damage was overlayed by cuts and abrasions that were offset 15° from the plane of tire rotation. The localized damage to all four tires suggests that the tires locked up simultaneously before the runway end. The overlaying cuts and abrasions indicate that the wheels remained locked during the overrun into the gravel.
1.6.6 Passenger Address and Interphone System
A public address (PA) system allows for communication from the flight crew and the cabin crew to the passengers. The interphone system permits private communication between the flight crew and the cabin crew. The PA/interphone handset in the cabin is next to the cockpit door. When the forward flight attendant is seated in the attendant's jump seat, the handset is out of reach. A PA/interphone was not available at the aft flight attendant station on this particular aircraft; however, some F28 aircraft have PA/interphone systems available at the aft flight attendant station.
1.6.7 Cabin Emergency Lighting
The cabin emergency lighting system functioned as designed and activated automatically. When the forward flight attendant is seated in the jump seat, the manual activation switch for the system is out of reach.
1.6.8 Exits
The flight attendant was unable to fully open the L1 door after shutdown. The R1 exit and both over-wing exits were available, but only the R1 exit was used. It was not necessary to deploy the R1 emergency slide because the nose of the aircraft was resting on the ground. There were no reported difficulties in evacuating passengers through the R1 door.
1.7 Meteorological Information
Before the approach, the pilots received a pilot report of weather conditions in flight, which reported visual acquisition of the Runway 16 landing lights at 1000 feet asl on approach. An aviation special weather report (SPECI) issued at 2256 for St. John's Airport was broadcast to the aircraft approximately 15 minutes before landing: surface winds 230°M at 5 knots; visibility 6 statute miles in very light rain showers and mist, with visibility northeast to south of 2 statute miles; ragged overcast ceiling at 400 feet; temperature 18°C, dew point 17°C; and altimeter setting 29.76 inches of mercury.
1.8 Aids to Navigation
1.8.1 Approach Types
Precision instrument landing system approaches are normally available in St. John's to runways 11, 29, and 16. Runway 29 was closed because of construction on the runways. The threshold to Runway 16 was displaced; as a result, the instrument landing system glidepath to the runway was not available. Only non-precision approaches to Runway 16/34 were available. A notice to airmen advised of these conditions.
1.8.2 Visual Approach Slope Indicator System
A visual approach slope indicator system (VASIS) consists of a series of lights designed to provide visual indications of the desired approach slope to a runway (usually 3°). Aerodrome Standards and Recommended Practices (TP312) states:
- 5.3.6.1 Standard - A visual approach slope indicator system shall be provided to serve the approach to a runway where one or more of the following conditions exist:
- the runway is not served by an electronic glide path and the runway is used by turbojet or other aircraft with similar approach guidance requirements;
- the pilot of any type of aircraft may have difficulty in judging the approach due to:
- inadequate visual guidance such as is experienced during an approach over water or featureless terrain by day or in the absence of sufficient extraneous lights in the approach area by night, or
- misleading information such as is produced by deceptive surrounding terrain or runway slopes;
- the presence of objects in the approach area may involve serious hazard if an aircraft descends below the normal approach path, particularly if there are no non-visual or other visual aids to give warning of such objects;
- physical conditions at either end of the runway present a serious hazard in the event of an aircraft under shooting or overrunning the runway; and
- terrain or prevalent meteorological conditions are such that the aircraft may be subjected to unusual turbulence during approach.
5.3.6.2 Recommendation - A visual approach slope indicator system should be provided to serve the approach to a runway where the runway threshold is temporarily displaced from the normal position and the runway is served by turbojet aeroplanes.
The approach charts for runways 11, 16, and 29 at St. John's all warn of moderate to severe turbulence. These runways are not equipped with a VASIS, and thus do not meet the standard (paragraph 5.3.6.1.e). Despite the displaced threshold, no VASIS was provided for the approach to Runway 16, contrary to the recommendation in paragraph 5.3.6.2.
1.9 Aerodrome Information
A reconstruction project for Runway 11/29 was under way at the time of the occurrence. The intersection of Runway 11/29 and Runway 16/34 was under reconstruction, and the threshold to Runway 16 had been displaced earlier in the day. This was the first night of flight operations with the displaced threshold.
A notice to airmen (990259 CYYT St. John's) advised that the first 1470 feet of Runway 16 were closed due to construction from 01 August 1999 to 15 August 1999. The threshold was temporarily displaced 1470 feet down the runway. The displaced threshold was marked by flags, cones, and wing bar lights. There was a lit, wooden sawhorse barrier across the runway before the displaced threshold. The landing distance available had been reduced to 5530 feet from 7000 feet. The runway was wet at the time of the occurrence, but there were no reports of standing water.
At the time of the occurrence, Runway 34 was equipped with visual vertical guidance, sequenced flashing approach lighting up to the runway threshold, normal runway end-lighting and markings, and an unobstructed threshold. The lowest MDA was 700 feet, 300 feet lower than the approach to Runway 16.
On 14 June 1999, six weeks before the accident, the runway surface friction for Runway 16 was checked using a Saab surface friction tester (SFT). The SFT friction index is calibrated on a scale of 0 to 100. Runway maintenance is required if the average runway friction index is less than 50 or if any 100-metre portion of the runway has an index less than 30. Maintenance is planned at index values 10% higher than these values. The friction measurement results indicated that Runway 16 had an average SFT index of 79. The lowest 100-metre SFT was 75, in the area of the touchdown zone.
TSB investigators inspected the runway the day after the accident for skid marks. No white streak/steam marks (indications of hydroplaning) or tire marks that could be associated with the aircraft were found. A helicopter, with TSB investigators on board, overflew the runway area three days after the accident, and pictures of the runway and overrun area were taken. Although not visible from the air, some of the photographs revealed faint black marks near the end of the runway. The runway marks joined with the aircraft tracks in the overrun and were only visible in the photographs taken from approximately 25 feet agl.
1.10 Flight Recorders
1.10.1 Flight Data Recorder
The FDR (Allied Signal, model 980-4120-GQUN, serial number 20025) was found to be in good condition, and the data stored in memory was fully recovered. The recording contained approximately 26 hours of data, including the occurrence. The quality of the data was very good, with no apparent losses.
The installation of the FDR was in accordance with the Canadian Aviation Regulations . Deactivation of the flight control lock activates the FDR. The company SOPs direct the crew to deactivate the control locks after the engines have been started; therefore, the engine start sequence is not captured. The European Organisation for Civil Aviation Equipment specification for FDR systems (EUROCAE ED-55 2.4.4) states: "It is recommended that, where practicable, the crew operating procedures should require the recorder to be switched on so as to record each engine start sequence."
1.10.2 Cockpit Voice Recorder
The cockpit voice recorder (L-3 Communications, model 93-A100, serial number 1057) was found to be in good condition, and the full 31 minutes of audio information was recovered. The cockpit voice recorder contained the pilot, co-pilot, and cockpit area microphone channels. Before the approach, during those periods when the intercom was not used, the internal communications were recorded only on the cockpit area microphone channel and were less discernable.
1.11 Wreckage and Impact Information
During the overrun, the aircraft nose gear broke off, and the aircraft continued forward on its fuselage, nose, and main gear. Concrete slabs and paving debris along the extended centreline caused the nose wheel to collapse.
1.12 Fire
There was no fire.
1.13 Survival Aspects
1.13.1 Audibility of Cabin Crew Brace Commands
Both flight attendants shouted the prescribed brace commands, "Emergency. Bend down. Stay down." The commands shouted by the aft flight attendant were heard only by those passengers seated aft of row 7. The area within which she could be heard was restricted due to the loud vibrations of the aircraft as it came to a stop. The commands shouted by the forward flight attendant were audible only in the first few rows of the cabin.
1.13.2 Commands from the Flight Crew to the Cabin
Standard terminology for flight crew commands after an accident is discussed in the emergency procedures portion of the operator's Flight Attendant Manual, under the title Crew Co-ordination. After the aircraft has stopped, a member of the flight crew can initiate an evacuation verbally through the PA system with "Evacuate, evacuate, evacuate," or by sounding the attendant call button five times in rapid succession. Upon receiving a call-button command, the flight attendants are to begin an evacuation. If the flight crew do not want an evacuation, the command "Remain seated" is broadcast over the PA system, directing the passengers to remain in their seats and indicating to the flight attendants that additional instructions are forthcoming.
1.13.3 Secondary Emergency Response
Normally, three St. John's Regional Fire Service fire rescue vehicles are in service and available to respond to an airport emergency. On the night of the occurrence, only one rescue vehicle was available; additional ambulance support was requested from the St. John's Health Care Corporation ambulance service. Because of miscommunication between the airport and the ambulance service, this ambulance did not arrive until about 40 minutes after the request. By then, the passengers and the crew had been bused to the terminal building, and four of the injured had been taken to hospital by the one rescue unit available at the airport.
Shortly after the evacuation was complete, emergency response personnel requested bus transportation from a local bus company for the uninjured passengers. The bus arrived approximately 40 minutes later. The TSB is aware of two other accidents where there was a significant delay in the provision of passenger ground transportation from the site to a holding area.
1.14 Tests and Research
During the investigation, the National Research Council conducted research into the deceleration characteristics of the aircraft during the ground roll to ascertain the effectiveness of the wheel braking. The results showed that there was no wheel braking evident.
Representative flights were flown in an F28 flight simulator. The simulator was not the same model as the accident aircraft, and adjustments were made to compensate for performance differences. With the brakes operative, the aircraft (simulator) consistently stopped within the confines of the runway. When brakes were not applied, runway departure speeds were similar to that of the occurrence aircraft.
1.15 Organizational and Management Information
Inter-Canadien was a regional carrier operating a number of F28 and ATR 42 aircraft. The company used a central dispatch system that provided crews with all pertinent pre-flight information. The company is no longer in operation.
1.16 Additional Information
1.16.1 Company SOPs
Company pilots received the following SOPs relating to the conduct of a non-precision approach:
- When making a non-precision straight-in approach, descend to Minimum Descent Altitude (MDA) as soon as practical after passing the final fix inbound with gear down, Flap 25 and [Vref] 42+ 20 KIAS. . . .
- When the runway is sighted and a straight-in landing can be accomplished, select the landing flap setting upon intercepting the landing profile and slow to [Vref] 42 + 10 KIAS. Cross the runway threshold at [Vref] 42.
- The pilot should not dive at the runway when breaking clear of the clouds at low altitudes from an instrument approach. High rates of descent that develop with this maneuver are not readily apparent on either the airspeed indicator or the vertical speed indicator, and may not be noticed until the flare point.
The company SOPs also state that any warning may be cancelled, with the exception of a GPWS warning. The correct response to a "sink rate" warning is to adjust the flight profile to remove the conditions that triggered the warning.
1.16.2 Stabilized Approaches
A stabilized approach has a constant rate of descent along an approximate 3° approach path that intersects the landing runway approximately 1000 feet beyond the approach end and begins not later than the final approach fix or the equivalent position. Flight from an established height above touchdown should be in a landing configuration with appropriate and stable airspeed, power setting, trim, and a constant rate of descent. Normally, a stabilized approach should be achieved no later than 1000 feet agl in instrument meteorological conditions.
The crew flew the non-precision approach as a step-down procedure, precluding a stabilized approach. Unstabilized approaches increase pilot workload and the risk that the approach will not be successful. The overwhelming majority of aircraft accidents occur during the descent, approach, and landing phases of flight, and most of these accidents occur during non-precision approaches.
1.16.3 Low-Energy Regime
The engines were reduced to idle thrust at 200 feet, placing the aircraft in a low-energy regime such that, if a rejected landing were to be attempted, there would be a delay in the engines responding to a power lever input by the pilot. Transport Canada's Commercial and Business Aviation Advisory Circular N0 0141, dated 13 May 1998, provides pilots and operators with guidance on the potential hazards associated with low-energy approaches, balked landings, and go-arounds. The circular states: "The decision to place an aircraft into the low-energy landing regime is a decision to land."
The engines were reduced to idle thrust at 200 feet, placing the aircraft in a low-energy regime such that, if a rejected landing were to be attempted, there would be a delay in the engines responding to a power lever input by the pilot. Transport Canada's Commercial and Business Aviation Advisory Circular N0 0141, dated 13 May 1998, provides pilots and operators with guidance on the potential hazards associated with low-energy approaches, balked landings, and go-arounds. The circular states: "The decision to place an aircraft into the low-energy landing regime is a decision to land."
1.16.4 Aircraft Performance
An aircraft take-off and landing chart for Runway 16 (wet) was provided to the crew before take-off. The chart is based on the use of 42° of landing flap, a threshold crossing height of 50 feet at Vref, and a touchdown point 1000 feet past the threshold. The chart indicates that the aircraft should have been able to stop in the runway available after touchdown with the lift dumpers inoperative. The accident aircraft had landed safely, in similar conditions (wet surface), on the same runway at 1302 that same day (Flight 4).
The FDR data of these two flights were compared, as shown in Figure 1. Based on FDR data and aerodynamic coefficients for the aircraft, it was estimated for the accident flight that, within approximately four seconds of touchdown, sufficient weight was transferred to the aircraft's main wheels to activate ground/flight relay switches and allow activation of the antiskid system.
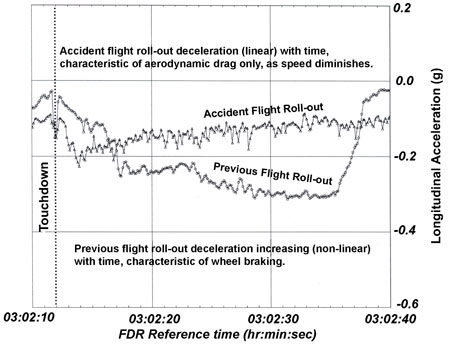
On both flights, a sudden increase in ground roll deceleration occurred immediately after touchdown (characteristic of wheel spin-up), followed by five seconds of relatively constant deceleration of about -4 feet/sec/sec. Flight 4 revealed two subsequent distinct deceleration segments attributed to effective wheel braking. During the accident ground roll, the deceleration was linear and decreased with time, characteristic of aerodynamic braking. The wheel braking on the accident flight was determined to be negligible, with most of the deceleration due to aerodynamic braking.
1.16.5 Hydroplaning
In general, three phenomena can result in very low braking friction coefficients on a wet runway surface: dynamic hydroplaning, viscous hydroplaning, and reverted rubber skidding (also referred to as a form of hydroplaning). Hydroplaning is a function of the water depth, speed, and in the case of dynamic hydroplaning, tire pressure. A non-rotating tire will begin to hydroplane at a lower speed than a rotating tire because a build-up of water under the non-rotating tire increases the hydroplaning effect. When hydroplaning occurs, the tires of the aircraft are completely separated from the actual runway surface by a thin water film. The tires will continue to hydroplane until a reduction in speed permits the tire to regain contact with the runway.
In Flight Theory For Pilots, Charles E. Dole describes dynamic and viscous hydroplaning as follows:
Dynamic hydroplaning is caused by the buildup of hydrodynamic pressure at the tire-pavement contact area. The pressure creates an upward force that effectively lifts the tire off the surface. When complete separation of the tire and pavement occurs, the condition is called total dynamic hydroplaning, and wheel rotation will stop. Total dynamic hydroplaning usually does not occur unless a severe rain shower is in progress. There must be a minimum water depth present on the runway to support the tire. The exact depth cannot be predicted since other factors, such as runway smoothness and tire tread, influence dynamic hydroplaning. Both smooth runway surface and smooth tread tires will induce hydroplaning with lower water depths. While the exact depth of water required for hydroplaning has not been accurately determined, a conservative estimate for an "average" runway is that water depths in excess of 0.1 [inch] may induce full hydroplaning.
Viscous hydroplaning is more common than dynamic hydroplaning. Viscous hydroplaning may occur at lower speeds and at lower water depths than dynamic hydroplaning. Viscous hydroplaning occurs when the pavement surface is lubricated by a thin film of water. The tire is unable to penetrate this film, and contact with the pavement is partially lost. Viscous hydroplaning often occurs on a smooth runway pavement or where rubber deposits are present, usually in the touchdown area where a thin water film can significantly reduce the coefficient of friction.
Reverted rubber skidding occurs when the tires lock on a wet runway surface. The heat generated by the friction causes reversion of the tread rubber to its uncured state, usually evident within the skid patch on the tire, and white streaks are formed on the runway due to build-up of steam in the tire/pavement contact area. When a runway surface changes from a smoother to a rougher texture, black skid marks may also be evident, due to erosion and depositing of rubber in the tire path over the rougher surface.
2.0 Analysis
2.1 Pre-flight
The pre-flight preparations were completed in accordance with normal procedures. The crew had all appropriate documentation required for the flight, and the aircraft was dispatched in accordance with company policy. The performance calculations showed that a safe landing could be effected in St. John's, despite the displaced threshold and the unserviceable lift dumpers. Furthermore, an uneventful flight in similar conditions had been made earlier that day. The captain's decision to conduct the flight to St. John's was informed and reasonable.
2.2 Approach
Before the approach, the crew had considered flying the approach to Runway 34. This would have provided the following advantages: a 300-foot lower MDA, visual vertical guidance to the threshold, a closer approach to the runway end, standard approach lighting, and standard runway touchdown zone markings. These advantages would have allowed a more stable approach and would also have allowed the crew to more easily acquire and fly a constant 3° approach angle from MDA to touchdown.During the final approach to Runway 16, there were deviations from the recommended airspeeds and required altitudes, and the approach flown was steeper than normal. When the decision to land was made, the aircraft was above the recommended airspeed and was 1 nm from the displaced threshold. The pilot assessed that he could continue the approach and arrive at the threshold at the required parameters. To achieve the required profile, the aircraft was placed on a steep descent in a low-energy regime. The steep descent and the manual silencing of the GPWS were not in accordance with company SOPs. The ability to perform a balked landing or a go-around was reduced by the low-energy state of the aircraft. At the displaced threshold, the aircraft was 35 feet higher and 18 knots faster than the recommended crossing height and airspeed.
2.3 Approach Lighting Standards and Recommended Practices
The recommended practice in TP312 to provide a VASIS to temporarily displaced thresholds is meant to lessen the risks associated with approaches to a non-standard landing environment. A displaced threshold increases the risk because the visual cues that a pilot would normally rely on to judge the approach to landing are frequently absent or may be misleading. The stopping distance available is also shortened. A VASIS would have assisted the pilot in maintaining the correct glidepath to the touchdown point.
2.4 Landing Roll
The deceleration data provided by the FDR showed that the aircraft did not decelerate in a similar manner to a flight landing on the same runway in St. John's earlier that day in similar conditions. Further, representative flights flown in a flight simulator consistently showed that the aircraft was capable of stopping within the confines of the shortened runway. Therefore, extensive testing of the brake system was carried out, and a comprehensive evaluation of the runway condition was undertaken to assess why the landing roll carried the aircraft beyond the end of the runway.For dynamic hydroplaning to occur, the water had to have been deeper than the tread channel. No standing water was observed after the accident, and the tires were in good condition with good tread depth. It is reasonable to conclude that dynamic hydroplaning did not occur. The extent to which viscous hydroplaning and/or reverted rubber skidding contributed to the lack of wheel braking could not be determined; however the conditions necessary for either were present, and there are indications for the occurrence of both. The lack of effective wheel braking during the application of normal braking is consistent with viscous hydroplaning, as is the negligible turning force displayed during yaw excursions on the landing roll. However, on the previous flight into St. John's, the same runway was used successfully under similar operating and environmental conditions, and no viscous hydroplaning occurred. This suggests that a successful landing should have been possible without encountering viscous hydroplaning. The damage to the tires indicates reverted rubber skidding during the alternate braking attempt and that the alternate braking system was functioning.
2.5 Braking
FDR analysis and performance calculations suggest that there was sufficient weight on wheels for the ground/flight relays to switch to the 'ground' position within four seconds of touchdown. FDR data also suggest that main wheel spin-up occurred shortly after touchdown. With these two parameters met, the normal braking system should have been available to the crew shortly after the aircraft touched down. The application of the alternate braking system caused the wheels to lock and resulted in the flat spots found on each tire. The locked wheels indicate that the alternate braking system was functioning. The lack of any discernable increase in deceleration indicates that poor braking conditions prevailed.It is possible that the normal braking system was functional during the landing roll but that effective wheel braking was unavailable due to a unique combination of factors, such as the following: reduced weight on wheels due to lack of lift dumpers, thus delaying the completion of locked-wheel touchdown protection circuits; antiskid cycling during viscous hydroplaning; reverted rubber skidding after the application of the alternate braking system; and the reduced braking to the right-hand inboard wheel. The extent to which any of these factors contributed to the lack of braking could not be determined.
2.6 Passenger Safety
2.6.1 Flight Attendant Actions
The flight attendants had no warning of the overrun yet surmised that an overrun was likely. Their commands to "brace" while still on the runway were entirely appropriate and demonstrated a high level of situational awareness. Their actions likely helped reduce the incidence of injury among the passengers.
2.6.2 Configuration of Flight Attendant Stations
The PA/interphone and the emergency light switch were not within reach of the forward flight attendant while seated. The PA system was not available to the aft flight attendant. While these conditions did not result in an adverse consequence in this occurrence, they represent a risk to passenger safety.Not all passengers could hear the "brace" commands issued by the flight attendants. The forward flight attendant's forward-facing seat resulted in her voice projecting forward, away from the passengers seated behind her, which is likely why the passengers had difficulty hearing her commands. The jump seat location and orientation are not unique to this aircraft. The aft flight attendant's commands were more audible; her jump seat, at the rear of the aircraft, was forward-facing. The high level of ambient noise created during the overrun further masked the flight attendants' commands.The aft flight attendant has no means to communicate with other cabin crew or the cockpit crew regarding commands or the status of the aircraft. In this occurrence, the aft flight attendant had no means to determine whether an evacuation or a rapid deplaning was required. It is important that the cabin crew know which commands are issued because these two commands require very different procedures.
2.6.3 Evacuation
The evacuation was conducted in an orderly and prompt fashion. It was, however, delayed slightly by miscommunication between the cockpit and the cabin and by the partially opened L1 door. This delay did not result in adverse consequences to the passengers or the crew.
2.6.4 Post-evacuation
The immediate response to the occurrence was prompt and effective. The tower controller expedited the emergency response by activating the airfield crash alarm before the overrun. The delayed provision of additional ambulance response and passenger transport did not result in adverse consequences in this instance; however, these factors could be critical in a more serious accident.
3.0 Findings
3.1 Findings as to Causes and Contributing Factors
- The aircraft could not be stopped on the runway because wheel braking was not effective.
- The following factors might have contributed to the lack of effective wheel braking: delayed completion of locked-wheel touchdown protection circuits; antiskid cycling during viscous hydroplaning; reverted rubber skidding after the application of the alternate braking system; and the reduced braking to the right inboard wheel during normal brake application. The extent to which any of these factors contributed to the lack of deceleration could not be determined.
3.2 Findings as to Risk
- A visual approach slope indicator system (VASIS) was not provided for the final approach to the displaced threshold, increasing the difficulty of visually acquiring and flying the final approach.
- The ability to perform a balked landing or a go-around on final approach was reduced by the aircraft's low-energy state.
- Miscommunication during the initial stages of the evacuation delayed the evacuation slightly.
- Flight attendants did not have access to communications equipment from their seated stations, increasing the risk of miscommunication or delay.
- There was a 40-minute delay in the provision of back-up ambulance support and passenger transportation.
3.3 Other Findings
- Performance calculations showed that Runway 16 at St. John's, with the displaced threshold, was of sufficient length to land the aircraft.
- The approach to Runway 34 would have provided a superior approach and landing environment.
- No antiskid/brake system anomalies were found that would have resulted in a total lack of wheel braking.
- The flat spots on each of the tires were due to locked wheels during the application of alternate braking.
- Engine starts are not captured on the F28 flight data recorder because company standard operating procedures state that flight control locks, which control the starting of the flight data recorder, be released after engine start.
- Debris on the overrun area was a major contributing factor in the nose-wheel collapse.
4.0 Safety Action
4.1 Action Taken
4.1.1 Approach Lighting Standards and Recommended Practices
On 15 October 1999, the TSB forwarded an aviation safety advisory to Transport Canada (TC) asking that TC consider means of further encouraging or requiring visual approach slope indicator systems (VASIS) at Canadian airports. TC's response on 03 April 2000 indicated support for broader application of VASIS. Before undertaking a complete regulatory review of the Aerodrome Standards, TC will recommend to the Part III Canadian Aviation Regulations Advisory Committee that paragraph 5.3.6.2 of Aerodrome Standards and Recommended Practices (TP312) be upgraded from a recommendation to a standard. The regional managers of Aerodrome Safety have been advised of the concerns raised by this advisory. They are additionally requested to consider these findings while processing the approval of airport construction plans.
4.1.2 Emergency Response - Secondary Vehicles
On 02 March 2000, the TSB forwarded an aviation safety advisory to TC suggesting that airport operators and applicable agencies review their emergency response plans with the view to ensuring the prompt provision of back-up and secondary emergency response vehicles. TC's response on 10 May 2000 indicated that a major revision to Part III of the Canadian Aviation Regulations (CARs) is expected to lead to the inclusion of material that is currently available only as guidance material. One such subject area to be affected is the emergency planning requirements. The TSB advisory will be considered in this CARs revision process. TC has also indicated that observed system deficiencies will be distributed to all airport operators to encourage evaluation of their own program shortcomings. Civil Aviation, Atlantic Region, has already taken action in this regard by distributing a letter to airport operators of that region, recommending that they add to their emergency response plan a section addressing transportation of uninjured passengers in the absence of on-site airline representatives.A notice of proposed amendment (NPA 2000-244) titled "Airport Emergency Planning Standard" is presently before the Department of Justice.St. John's airport has purchased a bus to ensure that passenger transport is available during emergencies. St. John's airport and the Health Care Corporation of St. John's (the ambulance provider) have revised their communication procedures to ensure direct communication during emergencies. The ambulance provider will no longer be notified of an emergency through a third party (the 911 operator). Communications will be direct from the control tower to the ambulance provider and will include more information to determine the potential resources required. In addition, the Health Care Corporation of St. John's has implemented a new on-call system that provides a representative for immediate response to airport emergencies.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .
5.0 Appendices
Appendix A - Schematic of Landing
Appendix B - List of Supporting Reports
The following TSB Engineering Laboratory Reports were completed:
- LP 88/99 - Flight Recorders and Aircraft Performance Analysis
- LP 096/99 - Examination of Tires
These reports are available upon request from the Transportation Safety Board of Canada.
Appendix C - Glossary
- ADT
- Atlantic daylight time
- agl
- above ground level
- asl
- above sea level
- ATPL
- Airline Transport Pilot Licence
- CARs
- Canadian Aviation Regulations
- deg
- degrees
- FDR
- flight data recorder
- fpm
- feet per minute
- ft
- feet
- GPWS
- ground proximity warning system
- hdg
- heading
- hr
- hour
- ICN
- Inter-Canadien
- KIAS
- knots indicated airspeed
- CMDA
- minimum descent altitude
- min
- minute
- NDT
- Newfoundland daylight time
- nm
- nautical mile
- P1
- pilot
- P2
- co-pilot
- PA
- public address system
- Rwy
- runway
- sec
- second
- SFT
- surface friction tester
- SOPs
- standard operating procedures
- SPECI
- aviation special weather report
- TC
- Transport Canada
- TSB
- Transportation Safety Board of Canada
- Vref
- reference speed
- VASIS
- visual approach slope indicator system
- °
- degree(s)
- °M
- degree(s) magnetic