
Railway Investigation Report R08W0219
Employee injury
Canadian National
Mile 150.70, Sprague Subdivision
Symington Yard, Winnipeg, Manitoba
22 October 2008
The Transportation Safety Board of Canada (TSB) investigated this occurrence for the purpose of advancing transportation safety. It is not the function of the Board to assign fault or determine civil or criminal liability. This report is not created for use in the context of legal, disciplinary or other proceedings. See Ownership and use of content.
-
Table of contents
Summary
On 22 October 2008, at 0250 central daylight time, at Symington Yard in Winnipeg, Manitoba, a Canadian National mechanical employee was working at a derailment site near track CO31. While monitoring a crane that was lifting a derailed car, the employee was struck by a beltpack yard assignment, which was travelling westward on the switching lead track adjacent to the work site. The employee was injured and was transported to hospital and subsequently released.
Ce rapport est également disponible en français.
Factual information
The accident
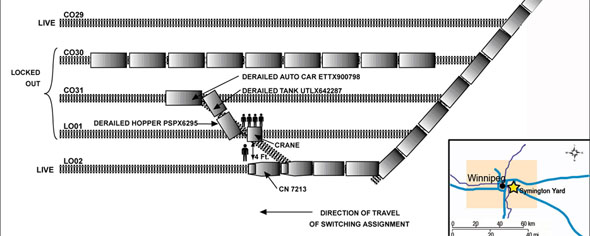
On 21 October 2008 at approximately 1400,Footnote 1 a three-car derailment occurred at the Canadian National (CN) Symington Yard, located in Winnipeg, Manitoba, near the centre of the hump yard at the crossover between track LO01 and track CO31 (see Figure 1).
A mechanical wrecking crew and several pieces of heavy equipment were assembled to re-rail the derailed cars. The wrecking crew consisted of a senior mechanical officer, two mechanical supervisors, and three employees, including a crane operator. All employees were qualified for their positions. At approximately 1430, after a job briefing was conducted, re-railing activities commenced in the middle of the switching yard.
During wrecking operations, tracks CO29, CO30, CO31, and LO01 were initially locked outFootnote 2 from switching activity. However, tracks LO02 and R09 were not locked out because these were the only switching leads left that could access a majority of the local classification tracks (see Figure 2).

Once the mechanical wrecking crew and heavy equipment accessed the work site, track CO29 was unlocked and switching resumed on this track. During the re-railing process, the crane and wrecking crew moved eastward towards track LO02 after re-railing each car.
The work at the derailment site continued into the next day. On 22 October 2008 at approximately 0250, while in the process of making a lift on hopper car PSPX6295, an employee was positioned south of the hopper car on the west side of the crane to monitor the outriggers for the lift. During the re-railing procedure, the crane operator geared up the crane's engine to increase the lifting ability of the crane. With the crane's engine operating, noise immediately adjacent to the crane was in excess of 100 decibels. The employee was wearing a hard hat and had his jacket hood up to protect himself from the weather. He also had his back to track LO02.
While monitoring the crane, the employee noticed his fellow employees on the north side of the track waving and yelling at him. With noise from the operating crane, the employee could not hear what the other employees were saying. However, assuming that there was a problem with the lift, the employee turned to move around the crane outrigger and was then struck by the front of locomotive CN 7213 on the yard assignment. The employee was thrown several metres and landed just clear of the north rail of the switching lead track LO02 that CN 7213 was travelling on. The injured employee was able to walk and was immediately transported to hospital in a company vehicle. At the hospital, it was determined that the employee had a broken left wrist, a facial laceration, and bruising about the right knee. The employee was treated, released, and referred for follow-up.
Canadian National yard assignment
The yard assignment (with the slave unit trailing the lead locomotive) was being operated by beltpack and was travelling westward on track LO02 at approximately 10 mph as it approached the location of the wrecking operations on track LO01. The locomotive bell was sounding and the headlight was on dim as the assignment moved up the lead. The assistant yard conductor was on the south side of the locomotive and was therefore unable to see the wrecking operations. The yard conductor at the tail end was controlling the movement.
The two-person crew operating the beltpack yard assignment was unaware that their train had struck the employee. Because they were not informed about the accident, they continued their switching activities. Once the injured employee was transported off site, wrecking operations at the derailment site continued.
At the time of the occurrence, the temperature was 4°C. The wind was at 30 km/h, gusting to 40 km/h, and it was raining.
Track lockout procedures during wrecking operations
Switching operations do not generally stop in rail yards when wrecking operations are taking place on adjacent tracks, subject to appropriate protective measures.
During wrecking operations within a live rail yard, the decision as to how many tracks are locked out and blue flagged is left to the discretion of the senior officer on site, in discussion with the yard production coordinator. If a track that is locked out is needed for switching operations, wrecking operations may stop while the track block is temporarily lifted, or wrecking operations will continue with less work space.
Track R09 extends from track LO02 just east of the derailment area and was available to be used as an alternate route to conduct switching operations. During wrecking operations, tracks CO30, CO31, and LO01 were locked, while tracks LO02, CO29, CO30, and R09 were not.
As the wrecking crane was preparing to lift the east end of the derailed car (PSPX6295), it was in close proximity to a live switching lead. The outrigger for the crane was within four feet of the north rail of track LO02. Under these circumstances, occupancy, access to, and exit from the worksite were confined by the positioning of equipment and the live tracks. From where the injured employee was positioned, the employee was unable to move a safe distance from the car being lifted without encroaching upon live tracks.
Job briefing
Prior to commencing the wrecking operations, a job briefing was conducted by the senior mechanical officer with the wrecking crew. The briefing covered how the lift was going to be made to re-rail the cars, which tracks were protected, and who was to do what. However, the job briefing did not establish a safety perimeter for the wrecking site or a contingency plan in the event of an accident. In addition, as the work progressed, the job plan was not updated.
The yard switch crew working on the beltpack yard assignment was not provided with a job briefing. They were not made aware of the work plan at the derailment site nor of any safety precautions that should be taken. However, the yard conductor on the assignment had made his own inquiries to the control tower because he was concerned with the close proximity of the crane to track LO02. He was advised to use the locomotive bell if necessary when approaching the work site.
Training and procedures for wrecking crews at Symington Yard
CN Mechanical employees are trained on the specifics of re-railing equipment, crane lifting techniques, and heavy equipment operations. CN training material for wrecking crews does not contain specific policies, procedures, or standards for wrecking operations in a live switching yard, for example:
the minimum space required to conduct wrecking operations in a live switching yard; and the number of tracks to lock out or the safety perimeters required to re-rail equipment.
Human Resources and Social Development Canada incident reporting
CN is a federally regulated company and is governed by the Canada Labour Code under the jurisdiction of Human Resources and Social Development Canada (HRSDC).
Section 15 of the Canada Occupational Health and Safety Regulations (COHSR) requires an employer to take specific action upon being made aware of an accident. Without delay, the employer must appoint a qualified person to investigate the accident, notify and involve the workplace Health and Safety Committee union representative, and take necessary measures to prevent a recurrence. Where there has been a disabling injury to an employee, the employer must submit a report in writing within 14 days, in a form established in the regulations, summarizing the results of the investigation.
CN reported the employee injury to HRSDC two days after the occurrence. However, the local Health and Safety Committee union representative was not immediately involved and there were no measures put in place promptly to prevent a recurrence. Despite several requests by the local Health and Safety Committee, HRSDC did not investigate this incident.
Canadian National's Safety Management System
The effective management of safety requires an organization to have a culture, structures and processes in place to allow for proactive identification and mitigation of risks. CN has been required to have a safety management system (SMS) in place since 2001. This was highlighted in the investigation into the Lillooet derailment in June 2006 (R06V0136), where the Board recommended that:
Canadian National take effective action to identify and mitigate risks to safety as required by its safety management system, and the Department of Transport require Canadian National to do so.
Transportation Safety Recommendation R09-03, issued May 2009
In the Lillooet investigation, the failure to identify and mitigate risks through effective SMS emerged as a safety deficiency. With respect to the Symington Yard employee injury, no risk assessments had been conducted before the accident to identify and mitigate the risks associated with performing wrecking operations in a live switching yard.
Canadian National's accident investigation protocol and follow-up
CN has a corporate process for accident and incident reporting, investigation, and analysis. This process is documented in the company's Injury/Accident Investigation Standard and Guidelines for Reporting Accidents and Injuries. In addition, the process for tracking, follow-up, and evaluation of corrective action related to injuries and accidents is outlined in CN's Corrective Action/Safety Measure Management Standard. Local or regional supervisors and management are responsible for entering data into the company's tracking and reporting system. Regional and corporate risk management groups are responsible for monitoring the system data and performing data quality checks. The procedures for follow-up to an employee injury at CN include conducting a re-enactment, advising company managers and executives, and conducting follow-up discussions with supervisors. If it is determined that an employee is not completely compliant with all policies and procedures, the employee is disciplined or corrective coaching takes place and, in most cases, the investigative process ends.
In this case, CN conducted a re-enactment about two weeks after the accident. A close-out report on the incident with proposed corrective actions was completed in December 2008. Corrective action was implemented in September 2009, then updated and re-issued in November 2009. There was little follow-up within the local Health and Safety Committee, which had had raised concerns, both before and shortly after this accident, about re-railing cars in a live switching work environment. At the time of the accident and in the months following the accident, these concerns had not been addressed by the company.
Analysis
There were no equipment or track defects present that were considered contributory in this occurrence. The analysis will focus on training for wrecking crews, wrecking operation policies including coordination required, and the safety of wrecking crews during rail yard operations.
The accident
It was dark as the beltpack assignment approached the derailment location. The assistant yard conductor was riding on the locomotive engineer's side of the locomotive (south) and was not in a position to observe the wrecking operations.
The employee was situated directly beside the crane, which was blocking his view to the east. The employee's peripheral vision was further reduced by the hood of his jacket, which was raised to protect against the weather. Consequently, the employee did not see the yard assignment approaching. During re-railing operations, the crane's engine noise drowned out warning sounds such as the locomotive bell and shouts from co-workers. As a result, the employee's ability to see or hear the approaching assignment and to respond to warnings was reduced by darkness, weather, and engine noise from the crane.
The employee was turned with his back to track LO02 so he could monitor the crane's outriggers. His co-workers observed the yard assignment and began yelling and waving their arms to try and get his attention. Unable to hear his co-workers, the employee assumed that they were warning him that the lift was shifting. Unaware that the yard assignment was approaching from the east on track LO02, the employee began to move around the outrigger and was subsequently struck by the locomotive.
A high volume of rail traffic passes through Symington Yard each day. Timely processing of this rail traffic requires that the hump and associated classification tracks are fully operational to meet on-time processing targets. When several tracks are involved in a derailment, it becomes difficult to process traffic and maintain on-time standards. In this occurrence, the four tracks that were locked out for re-railing slowed the productivity of the hump and delayed train building. To meet operational demands, track CO29 was returned to live status. Tracks LO02 and R09 were not locked out because they were the only switching leads for the yard assignment to pull cars from the majority of the local classification tracks. Had tracks LO02 and R09 been locked out for wrecking operations, there would have been a severe negative impact on yard productivity. This influenced the decision as to which tracks to lock out, reducing the size of the wrecking operation work site and, therefore, the level of protection.
Outriggers are used by the crane for stability. When the wrecking crew set up the crane for the lift, the outriggers extended to within four feet of track LO02. This left minimal space between the outrigger of the crane and the passing locomotives. When the locomotive of the yard movement passed beside the crane's outrigger, there was not sufficient space for the employee to safely manoeuvre around the outrigger without fouling the live switching lead. The locomotive struck the employee because the physical space required to safely conduct re-railing activities was insufficient and the protective measures in place were inadequate.
Job briefings are conducted to ensure that employees are able to work efficiently and safely. As the job proceeded, the proximity of track LO02 increasingly confined the workplace of the wrecking crew to the point where the employee monitoring the outriggers was no longer positioned with a safe exit route. The job briefings conducted were inadequate to identify the restricted physical space and to take timely preventive action.
Wrecking crew operations in a live switching yard
While the wrecking crew was trained to re-rail cars with the use of a crane, no instructions were given on working near equipment while in proximity to live yard tracks. No instruction was given outlining a safe work perimeter. There was also no guidance as to the standard distance or number of tracks to lock out to establish a safe working zone. These decisions were left to the senior officer on site. Without specific policies, guidelines, or training for safe working perimeters (for example, number of tracks to lock out), there is an increased risk that work crews can move onto or foul of live track, leading to a collision or injury.
In addition, no risk assessments were conducted before the accident to identify and mitigate the risks associated with performing wrecking operations in a live switching yard. The effective management of safety requires an organization to have a culture, structures, and processes in place to allow for proactive identification and mitigation of risks. Without conducting a risk assessment for wrecking crew operations in a live switching yard, the risks to these employees may not be appropriately identified and mitigated.
Job briefing
Job briefings provide an opportunity for work crews to discuss the job at hand and how to execute it in the best possible manner. In this occurrence, items such as safe working perimeters and the number of tracks to lock out were not adequately discussed during the job briefing. In addition, the switching crews working in the immediate area were not provided with an appropriate job briefing and were therefore unaware of the extent of the wrecking operations occurring on track LO01. When the yard conductor on the switching crew inquired with tower personnel about the wrecking operations, he was told to use the locomotive bell if necessary when approaching the work site. Where switching crews are not briefed on yard work that may affect their activities, they may not take adequate safety precautions—increasing the risk of collision or injury.
Canadian National's accident investigation protocol and follow-up
Following this accident, CN's internal processes for investigation and implementation of corrective action were not followed. Once arrangements had been made to transport the employee to hospital, completing the wrecking operation became the priority. Those in charge did not promptly conduct an investigation, interview employees, and stage a re-enactment at the accident site.
CN conducted the re-enactment two weeks after the accident with no local Health and Safety Committee involvement. The close-out report on the incident was not widely distributed and corrective action was not implemented until almost a year later. Following an accident, it is important for organizations to thoroughly examine what happened and why so they may quickly identify risks in their operations and put in place measures to reduce those risks.
Findings
Findings as to causes and contributing factors
- The employee's ability to see or hear the approaching assignment and respond to warnings was reduced by darkness, weather, and engine noise from the crane.
- Unaware that the yard assignment was approaching from the east on track LO02, the employee began to move around the crane's outrigger and was struck by the locomotive.
- Operational considerations influenced the decision to continue switching operations on track LO02, reducing the physical space available to the wrecking crew and, therefore, the level of protection.
- The locomotive struck the employee because the physical space required to conduct re-railing activities was insufficient.
- The job briefings conducted did not adequately identify and mitigate the risks associated with working in the restricted physical space.
Findings as to risk
- Without specific policies, guidelines, or training for safe working perimeters or the number of tracks to lock out, there is an increased risk that work crews can move onto or foul of live track, leading to collisions or employee injuries.
- Without conducting a risk assessment for wrecking crew operations in a live switching yard, the risks to these employees may not be appropriately identified and mitigated.
- Where switching crews are not briefed on yard work that may affect their activities, they may not take adequate safety precautions, which may increase the risk of collision or injury.
- Following an accident, it is important for organizations to thoroughly examine what happened and why, so they may quickly identify risks in their operations and put in place measures to reduce those risks.
Safety action taken
Canadian National (CN) developed and implemented track protection procedures for derailment clearing operations within the Winnipeg Terminal.
CN implemented a protocol requiring a transportation officer to lead the investigation of all incidents to ensure compliance with all investigation recording and reporting requirements.
CN initiated a series of internal audits at Symington Yard and other rail yards throughout Canada as part of its data quality initiatives. Where non-compliance to company policies was identified, corrective action was initiated.
Human Resources and Social Development Canada (HRSDC) followed up with CN and with the Health and Safety Committee to ensure awareness of their responsibilities under the Canada Labour Code.
This report concludes the Transportation Safety Board's investigation into this occurrence. Consequently, the Board authorized the release of this report on .